Article Text

Abstract
Introduction The PulseRider is a novel device intended for use in the treatment of aneurysms arising at bifurcations. We present the initial results of the first three cases in the USA employing the PulseRider device.
Methods Aneurysms intended to be treated with the PulseRider device at a single institution were identified prospectively. Aneurysms arising at either the carotid terminus or basilar apex that were relatively broad-necked were considered candidates for treatment with the novel device.
Results Patients were pretreated with dual antiplatelet therapy. All cases were performed under general endotracheal anesthesia. An appropriately sized PulseRider device was deployed across the neck of the aneurysm. A microcatheter was then navigated over a 0.014 inch microwire through the device into the aneurysm. Complete occlusion of the aneurysm was achieved in all cases without intraprocedural complications.
Conclusions We have found in our early experience with the Pulse Rider device that its use is safe and effective as an adjunct in the treatment of bifurcation aneurysms arising at the basilar apex or carotid terminus. As such, it represents a useful addition to the armamentarium of the neuroendovascular specialist.
- Aneurysm
- coil
- device
- stent
- wide-necked
Statistics from Altmetric.com
Introduction
Since the International Symptomatic Aneurysm Trial (ISAT)1 and the Barrow Ruptured Aneurysm Trial (BRAT)2 firmly established endovascular therapy as a valid method for treating intracranial aneurysms, development of new techniques has broadened the scope of practice to allow for the treatment of geometrically complex aneurysms.3–8 Advances in endovascular techniques including balloon remodeling as well as the use of stents have allowed more of these challenging aneurysms to be treated with coil embolization. A novel device intended for use in the treatment of aneurysms arising at bifurcations is the PulseRider (Pulsar Vascular, San Jose, California, USA).9 It is designed to remodel a bifurcation, providing support at the aneurysm neck while protecting the daughter branches during coil embolization. However, no clinical data for cases exist in the USA. We present the initial results on the first three cases in the USA employing the PulseRider device.
Methods
Aneurysms intended to be treated with the PulseRider device at a single institution were identified prospectively. Aneurysms arising at either the carotid terminus or basilar apex that were relatively broad-necked were considered candidates for treatment with the novel device. Patient demographics, procedural details, and immediate neurologic and angiographic outcomes were recorded retrospectively.
PulseRider device
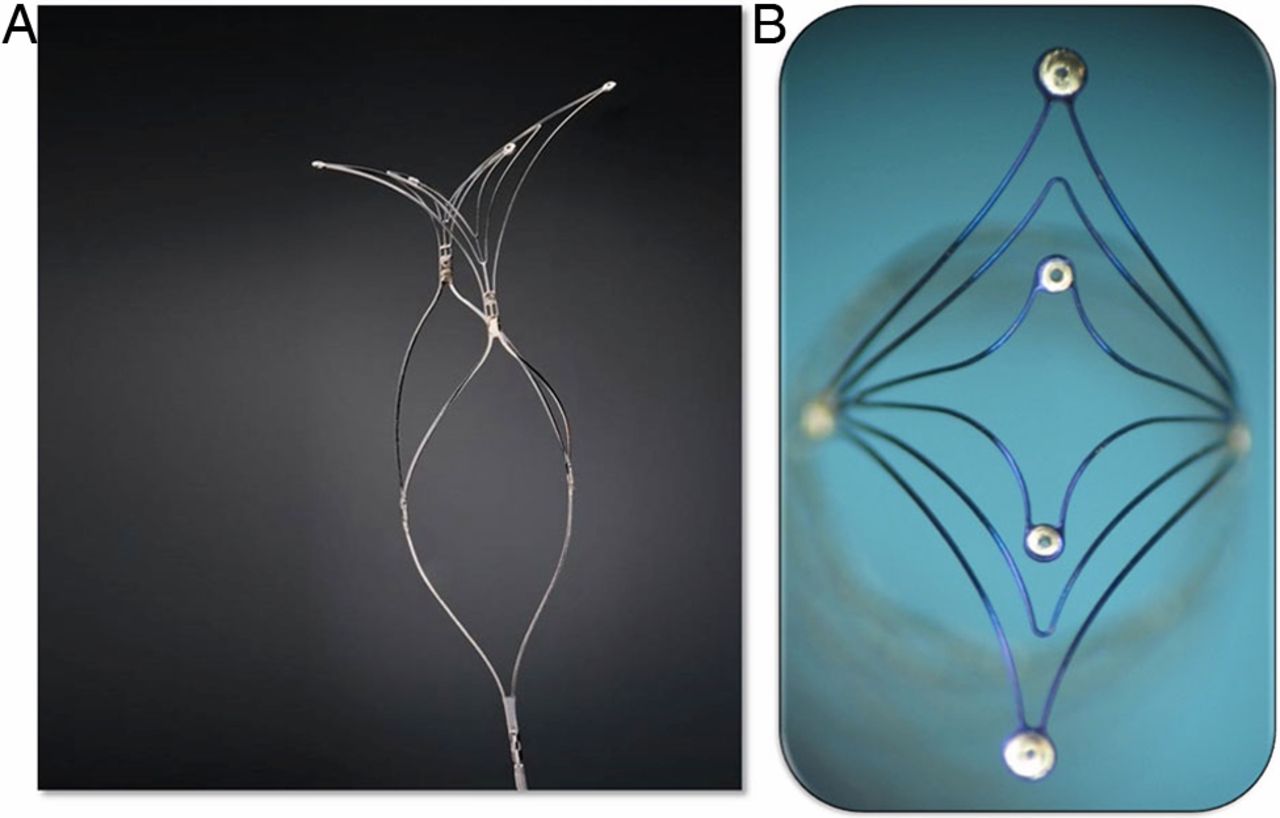
The device is a self-expanding nitinol implant (figure 1A, B) that is delivered on a stainless steel delivery wire within any commercially available 021 diameter microcatheter. The device is fully retrievable and can be repositioned and torqued to fit the relevant anatomy. The device itself has significantly less metal than a conventional stent with the majority of the surface area coverage focused at the neck of the aneurysm. The device is available in both ‘T’ and ‘Y’ configurations, intended to fit the geometry of the daughter vessels arising at the bifurcation. The device is also available in different diameters and lengths.

(A) The Pulse Rider Device is a self-expanding nitinol implant that is fully retrievable and can be repositioned with radiopaque markers to aid in visibility during deployment and manipulation. The device photographed is a ‘Y’-shaped device, although the devices also comes in a ‘T’ configuration and have several different diameters and lengths available. (B) The device itself has significantly less metal than a conventional stent, with the majority of the surface area coverage focused at the neck of the aneurysm.
Coil embolization technique
All patients underwent a cerebral angiogram with three-dimensional reconstruction as deemed necessary prior to the intervention. Patients were pretreated the evening before with clopidogrel (600 mg orally ×1) and aspirin (650 mg orally ×1) and then maintained on daily doses thereafter (clopidogrel 75 mg orally and aspirin 325 mg orally). All cases were performed under general endotracheal anesthesia. After obtaining percutaneous access (transfemoral in two, transradial in one), heparin was administered and an activated clotting time was obtained to achieve a level 2–2.5 times baseline. A guide catheter was positioned into the vessel of interest and working views were obtained in both the anteroposterior and lateral projections. In all cases, a Prowler Select plus 021 microcatheter (Codman Neurovascular, Raynham, Massachusetts, USA) was navigated over a 0.014 inch microwire and positioned at the neck of the aneurysm. An appropriately sized PulseRider device was then deployed across the neck of the aneurysm with limbs in the daughter vessels. A ‘T’ versus ‘Y’ configuration device was chosen at the operator's discretion based on the geometry of the daughter vessels arising at the bifurcation. The device was initially deployed across the neck, but not detached. A microcatheter was then navigated over a 0.014 inch microwire through the device into the aneurysm. Coil embolization was then begun with follow-up angiography throughout the remainder of coiling as required. The device was detached either at or near the conclusion of coil embolization. Table 1 shows the procedural device details.
Summary of patient demographics, presentation, aneurysm location and characteristics, devices used during the procedure as well as the immediate angiographic outcome and any intraprocedural complications encountered
Case reports
Case 1
A patient aged 70+ with a history of hypertension and emphysema suffered a fall from a syncope event. A non-contrast CT scan demonstrated an approximately 15 mm hyperdense lesion in the interpeduncular cistern concerning for a large basilar apex aneurysm. The patient was neurologically intact with a small superficial contusion over the right scalp and left periorbital ecchymosis. Diagnostic cerebral angiography demonstrated an incidental irregular 15 mm basilar apex aneurysm with a 12 mm neck that incorporated the origins of the posterior cerebral artery (PCA) P1 segments bilaterally (figure 2A–D). The patient elected for treatment. Complete occlusion of the aneurysm was achieved without intraprocedural complications employing the coil-through technique with the PulseRider. The patient was discharged on the following day and was maintained on aspirin and clopidogrel.
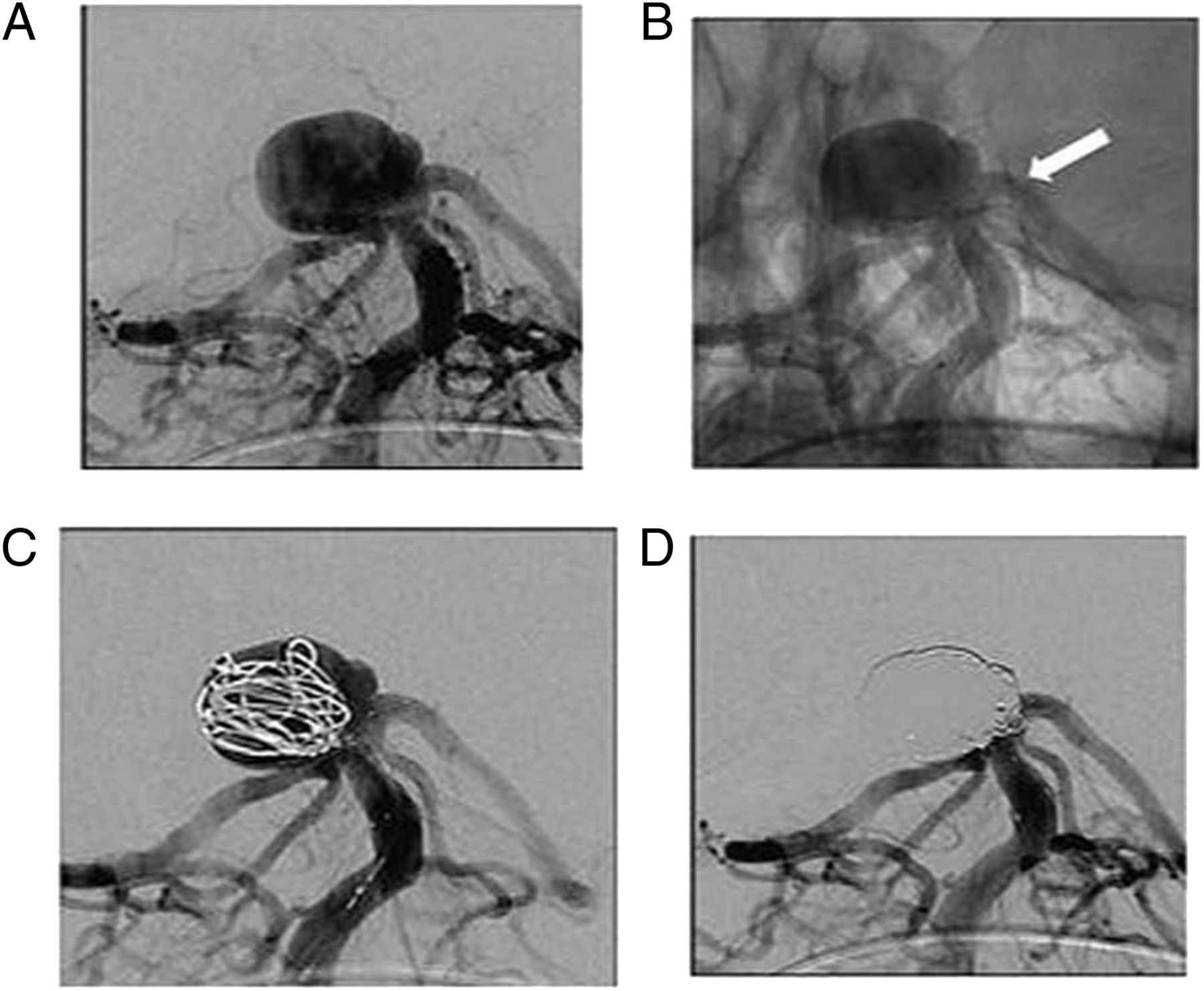
(A) Digital subtraction angiography (DSA) in the anteroposterior (AP) working projection demonstrates a large basilar apex aneurysm with partial incorporation of the posterior cerebral artery origins. (B) Post device deployment in the native view demonstrates the Pulse Rider across the neck of the aneurysm (white arrow). (C) DSA in the AP projection after accessing the aneurysm through the device with deployment of the first coil. (D) Final immediate treatment angiogram in the AP working projection demonstrating complete occlusion of the aneurysm.
Case 2
A patient aged 60+ with a history of hyperlipidemia, anxiety and pacemaker for sick sinus syndrome was evaluated for syncope and recent memory disturbance. Investigation included a MRI study of the brain which revealed a 5 mm right carotid terminus aneurysm with a broad neck (figure 3A–E). The patient elected to undergo treatment of the aneurysm. Complete occlusion of the aneurysm was achieved without intraprocedural complications employing the coil-through technique with the PulseRider. The patient was discharged on the following day and was maintained on aspirin and clopidogrel.

(A) Digital subtraction angiography in the anteroposterior (AP) working projection demonstrates a carotid terminus aneurysm projecting anteriorly and superiorly. (B) Reconstruction from a three dimensional rotational angiogram demonstrates the partial circumferential involvement of the carotid terminus as well as the severe angulation of the bifurcation. (C) Working AP projection roadmap image after accessing the aneurysm (black arrow) through the device demonstrates the device across the neck of the aneurysm (white arrow). (D) Native view of the AP working projection demonstrates the ‘saddle’ of the Pulse Rider (white arrow) maintaining the initial coils within the aneurysm sac. (E) Final immediate treatment angiogram in the AP working projection demonstrating complete occlusion of the aneurysm.
Case 3
A patient aged 60+ with a history of hypertension and left bundle branch block was invstigated for dizziness and found to have a large incidental basilar apex aneurysm measuring 8×7 mm with a 4.7 mm broad neck (figure 4A–D). Complete occlusion of the aneurysm was achieved without intraprocedural complications employing the coil-through technique with the PulseRider. The patient was discharged on the following day and was maintained on aspirin and clopidogrel.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Digital subtraction angiography in the anteroposterior (AP) working projection demonstrates a large basilar apex aneurysm projecting superiorly and slightly posteriorly. (B) Working AP projection roadmap image and (C) angiogram after deploying the Pulse Rider device demonstrates the device across the neck of the aneurysm (white arrow). (D) Final immediate treatment angiogram in the AP working projection demonstrating complete occlusion of the aneurysm.
Discussion
Despite advances in stenting and balloon remodeling techniques, broad-necked aneurysms arising at bifurcations remain a challenge to endovascular treatment. These aneurysms occur at the junction of two essential branching arteries that must remain patent after embolization. Unassisted coiling or single stent techniques are frequently insufficient to protect the remaining daughter vessels and prevent coil prolapse leading to arterial occlusion. Flow diversion stenting is not ideal because this would effectively jail one of the limbs of the bifurcation.
The ‘Y-stent’ technique involves the passage of a second stent through the interstices of the first deployed stent. For example, for basilar apex aneurysms, the distal end of the first stent is positioned in the PCA that arises at the most acute angle from the basilar apex (or the one with the most difficult configuration to navigate), with the proximal end positioned in the distal basilar artery itself. The second stent is navigated through the interstices of the initial stent with the distal end in the contralateral PCA and the proximal half within and overlapping the first stent in the basilar artery (‘Y’), thus reconstructing the neck. The microcatheter is then navigated through the proximal true lumen of the stents and exited through the interstices into the aneurysm to achieve coil embolization (‘coil through’). The use of two stents in a ‘Y’ configuration (Y-stenting) to assist with coil embolization of complex bifurcation aneurysms was first described in 2004.10 Since that time, several reports have been published demonstrating acceptable morbidity and mortality rates associated with Y-stenting, and it has been accepted as a safe and reasonable alternative to clip reconstruction of a select subset of challenging aneurysms.11–24
However, Y-stenting remains technically challenging and requires many steps to be performed successfully. Compared with Y-stent reconstruction, the PulseRider has a very low metal-to-artery ratio with the highest density of metal positioned to cover the aneurysm neck and support a coil mass, thus there is no jailing of daughter branches and there is minimal intraluminal hardware that is not opposed to vessel intima. This device is fully retrievable and can be repositioned and recaptured until it is detached with an electrolytic detachment mechanism. This results in a technically easier procedure which is more streamlined, as only one device is required to be positioned to reconstruct the bifurcation. Fewer steps will theoretically result in fewer technical adverse events during the procedure. In addition, in the era of cost containment, employing a single device for vessel reconstruction may provide a higher value (quality/cost) over strategies using multiple devices.
The PulseRider device has received approval from the Food and Drug Administration for an investigational device exemption to be done under a humanitarian device exemption in the USA for the treatment of carotid terminus and basilar apex aneurysms. It is currently available in the USA only in the context of the Adjunctive Neurovascular Support of Wide-neck aneurysm Embolization and Reconstruction Trial (ANSWER) clinical trial. In our early experience we have found its use to be simple and safe, being readily delivered in a standard method very similar to other available stents, making the procedure more familiar to an operator new to the device. It is conformal and delivered without difficulty through any 021 microcatheter even in torturous anatomy. The device is easily recaptured and can be turned by pulling it back into the catheter while torqueing on the device and then redeploying it until it conforms to the specific anatomy. Once deployed across the neck the device can be crossed readily by navigating a standard coiling microcatheter over a familiar 0.014 inch microwire. Since the majority of the metal mass of the stent is concentrated at the neck, it is likely that patients could be managed safely with shorter dual antiplatelet regimens or even a single antiplatelet medication. Lastly, the metal support at the neck has proved to be sufficient to support a coil mass.
Conclusions
We have found in our early experience with the Pulse Rider device that its use is safe and effective as an adjunct in the treatment of bifurcation aneurysms arising at the basilar apex or carotid terminus. As such, it represents a useful addition to the armamentarium of the neuroendovascular specialist.
References
Footnotes
Contributors Each author made a material contribution to the article, the revision of the article, and the final approval of the article for submission to this journal.
Competing interests None.
Ethics approval Ethics approval was obtained from Medical University of South Carolina IRB.
Provenance and peer review Not commissioned; externally peer reviewed.