Article Text

Abstract
Background In the past decade, preoperative endovascular embolization of cerebral arteriovenous malformations (AVMs) became an essential tool in the treatment of these entities. With the current expansion of technology and wide incorporation of new devices, the indications for the use of endovascular embolization have expanded to include embolization for cure. This has been facilitated by the wide use of the new liquid embolic agents (ethylene-vinyl alcohol co-polymer (EVOH)) in addition to n-butyl cyanoacrylate (NBCA). The aim of this study was to review the current published literature for these two agents and report on permanent neurological injuries and cure rate.
Methods Published literature citing embolization results for AVMs using liquid embolic agents was reviewed. Papers reporting on permanent complication rates and complete angiographic cure were reviewed. A meta-analysis was performed based on these two variables for the two embolic agents.
Results 103 studies met the selection criteria. Poor neurological outcomes for NBCA and EVOH were 5.2% and 6.8%, respectively (OR 1.4; p=0.56). AVM complete obliteration rate was seen in 13.7% in the NBCA group and in 24% in the EVOH group (OR 1.9). This OR decreased to 1.35 in the subgroup analysis for patients treated after the year 2000.
Conclusions NBCA continues to have a trend towards lower permanent complication rates, but EVOH had higher angiographic cure rates. The recent literature has demonstrated an increase in the cure rate of AVMs with endovascular embolization techniques yet with a possible increase in permanent neurological deficits and mortality.
- Arteriovenous Malformation
- Complication
- Embolic
- Hemorrhage
- Liquid Embolic Material
Statistics from Altmetric.com
Introduction
Since the introduction of the embolization of cerebral arteriovenous malformations (AVMs) in 1960 by Luessenhop and Spence using methyl-methacrylate embolospheres,1 the embolization procedure gradually became an integral part of the multimodality paradigm in the treatment of brain AVMs. The goals of embolization have evolved over the past several decades, beginning as preoperative adjuncts to facilitate AVM resection.2 Although not currently approved by the US Food and Drug Administration (FDA), embolization prior to radiosurgery is performed to reduce nidal size or eliminate high risk features.3 Recently, with the expansion of experience and advancement of endovascular techniques, much debate has ensued about the appropriate role of embolization,4 with an emergent trend focusing on performing embolization for angiographic cure.5–,7
A wide variety of embolic agents have been used to treat AVMs although as of the current time only a few agents are widely used. These agents include the liquid embolic agents n-butyl cyanoacrylate (NBCA) (TruFill; Codman and Shurtleff Inc, Raynham, Massachusetts, USA), ethylene-vinyl alcohol co-polymer (EVOH) (Onyx; eV3-Covedien, Irvine, California, USA) and, to a lesser degree, embolic particles such as polyvinyl alcohol (PVA) (Contour; Boston Scientific, Natick, Massachusetts, USA).8 In the USA, both NBCA and EVOH are FDA approved as adjuncts for preoperative surgical resection.9 ,10 NBCA and EVOH received FDA approval in 2000 and 2005, respectively. NBCA has several advantages, including its complete occlusion of vessels, high permanence, and immediate reaction time. The major drawback of NBCA is the high amount of skill required for its proper use. Several complications can arise during use, including catheter entrapment in the occluded vessel.11 Polymerization can also spread distally or reflux proximally to the intended location if NBCA is not used properly and skillfully.
The advantages of EVOH include its non-adhesive nature. This allows for longer injection times and the ability to temporarily suspend embolization and proceed with further angiography mid procedure if necessary. Although the material is not adhesive and will not adhere to the catheter, there is still a risk of embedding the catheter in EVOH as it refluxes around the catheter tip.12
In this paper, we sought to review the published literature and perform a meta-analysis of the reported permanent morbidity/mortality and cure rate using these two agents.
Methods
A systematic review search was done for all available published studies on PubMed and Ovid Medline from January 1980 to November 2013. Reference lists from the identified studies were reviewed to uncover any potential studies that may have been missed in previous searches. Keywords included in the search were ‘N-butyle-2-cyanoacrylate; NBCA; Histoacryl; TruFill; ethylene vinyl alcohol copolymer; EVOH, Onyx’, and ‘brain arteriovenous malformation’. Studies were selected based on the following criteria: (1) clinical trials where at least one of the agents was included in prospective studies, retrospective studies, or an independent arm; (2) NBCA or EVOH exclusively or predominantly used in the studies; and (3) outcomes: all mortalities and permanent morbidity events related to the embolization procedures for each agent were reported as complication events. A secondary outcome was the complete obliteration rate of AVMs with embolization alone.
Exclusion criteria included: (1) studies reporting on more than one agent being used to embolize patients (except if used in small percentages as a complement to the main agent that was intended to treat the patient); (2) studies conducted on very small AVMs (<1 cm in diameter); (3) studies not reporting on outcomes; (4) duplicated studies from a single center (in such cases only the most recent study and inclusive data were selected unless the studies were conducted in different periods on different groups of patients;13 ,14 and (5) non-English articles.
The data elements extracted from each study included: (1) number of patients treated with each agent; (2) mean age; (3) gender; (4) study period; (5) embolic agent(s) used; (6) total number of embolization sessions; (7) percentage of patients with Spetzler–Martin grades I and II; and (8) clinical presentation. The measured results included poor neurological outcomes (permanent neurological morbidity or mortality) and immediate post-embolization complete obliteration events. Recurrence events were not included.
Statistical analysis
We estimated the cumulative incidence (event rate) per 100 patients, and 95% CI for each outcome from each study were applied. Because heterogeneity was found to be high between studies, event rates were pooled across studies using random effects meta-analysis with 95% CI.15 An OR with 95% CI and significance was performed to compare the two agents. A regression coefficient was calculated to determine if there was an association between outcome and study period, Spetzler–Martin grade I and II percentages, or the embolization session rates. Statistical heterogeneity of the studies was measured using the I2 test; levels above 50% were considered significant heterogeneity.15 Funnel plots were used to assess if there was publication bias. The compiled literature involved studies that spanned over the past two decades. Due to changes in treatment goals, procedure improvement, and technological advancements, subgroup analysis was based on the study period for each outcome conducted before and after the year 2000. The middle of the study duration was taken as a reference to categorize those studies conducted before 2000 and those after 2000. The analysis was conducting using OpenMetaAnalys16 and SPSS 18 (IBM, Armonk, New York, USA) software. All statistical tests were two sided, and statistical significance was defined as p<0.05.
Results
Search results
A total of 572 studies and abstracts were found in the primary search. After exclusion of duplicated, non-human, and irrelevant studies by abstract reviewing, 103 studies were selected for full review; 39 of these 103 studies met the selection criteria. Three studies were clinical trials, and the remainder were retrospective studies with a total of 3595 patients (2363 patients embolized with NBCA and 1232 patients embolized with EVOH). Table 1 shows the characteristics of the included NBCA studies and table 2 shows the characteristics of the included EVOH studies.
Characteristics of n-butyl cyanoacrylate studies
Characteristics of ethylene-vinyl alcohol co-polymer studies
Patient presentation and treatment
Mean patient age was 35.8 years and 35 years in the NBCA and EVOH groups, respectively (p=0.8). About 47% of patients in the NBCA group presented with hemorrhage compared with 41.5% in the EVOH group (p=0.3). Seizure was the presenting symptom in 28% of the NBCA group and in 33% of the EVOH group (table 3).
Characteristics of the studies
Heterogeneity test
The heterogeneity test was significantly positive in both groups, assuming the observed estimates of treatment effectiveness can vary across studies. Due to differences in the treatment affecting each study, a random effect model was incorporated to estimate the average treatment effect, and the CI depict the uncertainty around this estimate.17
Poor outcome (permanent morbidity or mortality) and complete obliteration rate
Poor neurological outcomes for NBCA and EVOH were 5.2% and 6.8%, respectively (figure 1A, B), with an OR of 1.4 (p=0.56) (figure 1C). When data for patients treated with EVOH using a detachable tip catheter were excluded, poor outcome of EVOH treatments increased to 7.1% (figure 1C). Due to technical advancements, there have been improvements in the safety of the procedure in the past decade with both agents (figure 2A, B). However, the association between complication rate and study period (January 1980–November 2013) was only statistically significant in the EVOH studies (p=0.02). This difference may be a reflection of the introduction of the detachable microcatheter tip. In the EVOH group, poor outcome with detachable tips was 6.8% compared with 7.1% without detachable tips (p=0.2).

(A) List of published literature and meta-analysis citing poor outcome in patients treated with n-butyl cyanoacrylate (NBCA). Cumulative poor outcome is seen in 5.2% of patients. (B) List of published literature citing poor outcome in patients treated with ethylene-vinyl alcohol co-polymer (Onyx). Cumulative poor outcome is seen in 6.8% of patients. (C) OR of poor outcome comparing Onyx with NBCA. The OR is 1.4 favoring a worse outcome in Onyx treated patients. (D) List of published literature citing poor outcome in patients treated with Onyx. Studies citing use of detachable microcatheters were excluded from this analysis. Cumulative poor outcome is seen in 7.1% of patients.
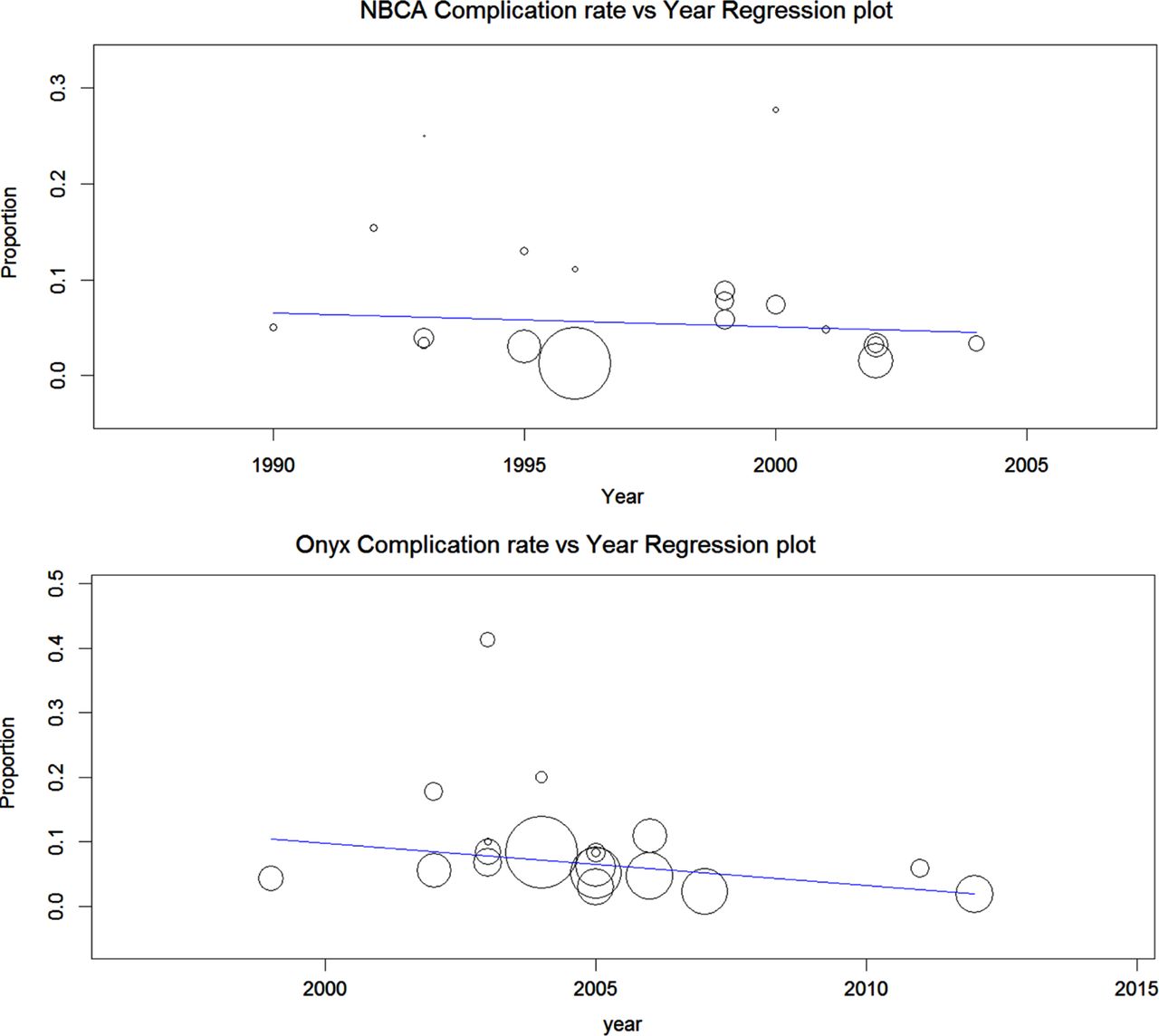
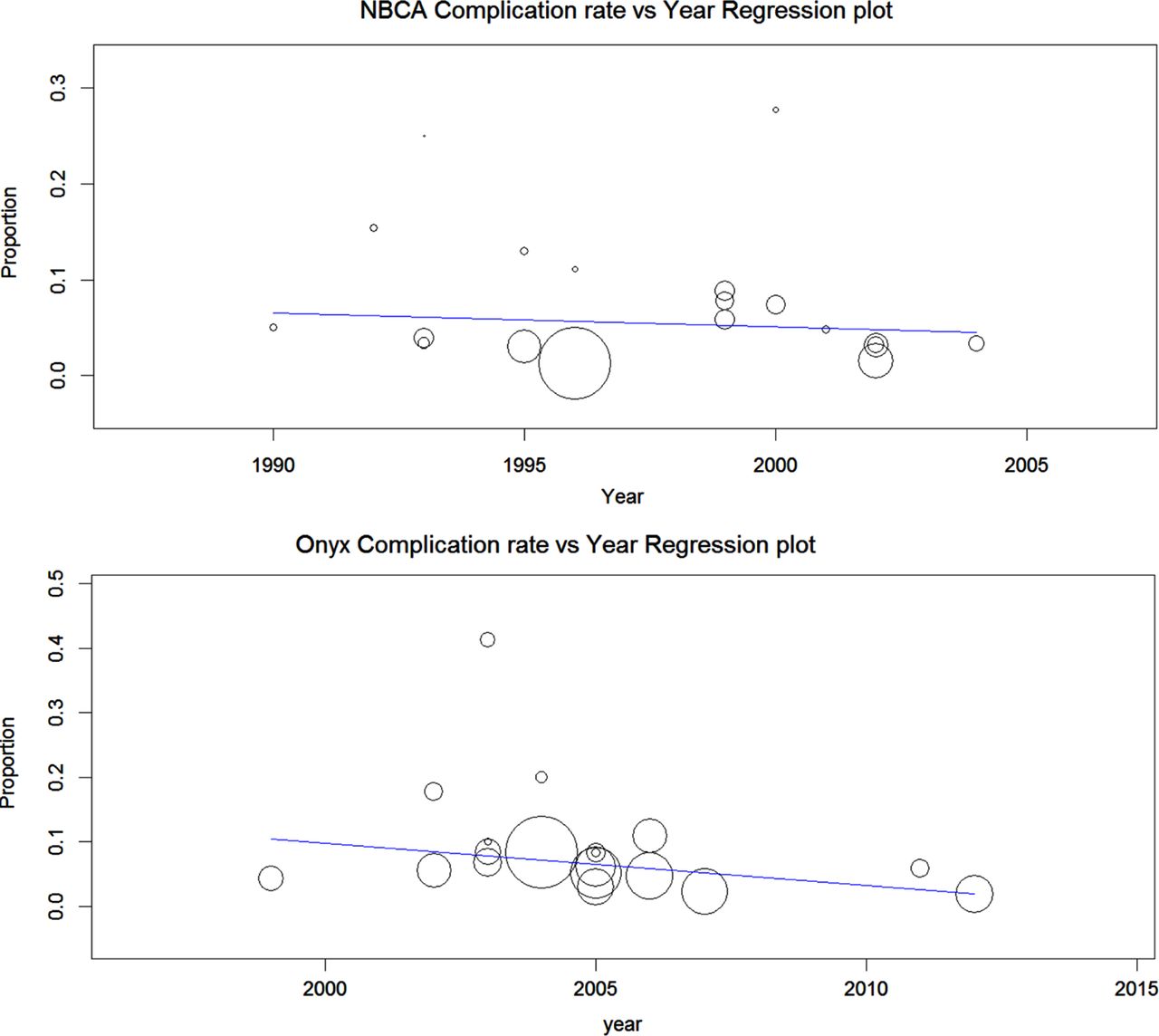
(A) Year regression plot for poor outcome in patients treated with n-butyl cyanoacrylate (NBCA). (B) Year regression plot for poor outcome in patients treated with ethylene-vinyl alcohol co-polymer (Onyx).
There was no significant change in poor outcome rates for NBCA between 1993 and 2012 (figure 2B). A subgroup analysis of the complication rates for 1549 patients on the studies conducted before 2000 (date of FDA approval in the USA) and for 631 patients on the studies conducted after 2000 showed poor outcome rates of 5.7% and 4.6%, respectively (p=0.1). After control for study period, there was no significant difference in poor outcomes between EVOH and NBCA (OR 1.4, p=0.56), but there was an overall trend towards poorer outcomes for EVOH over NBCA.
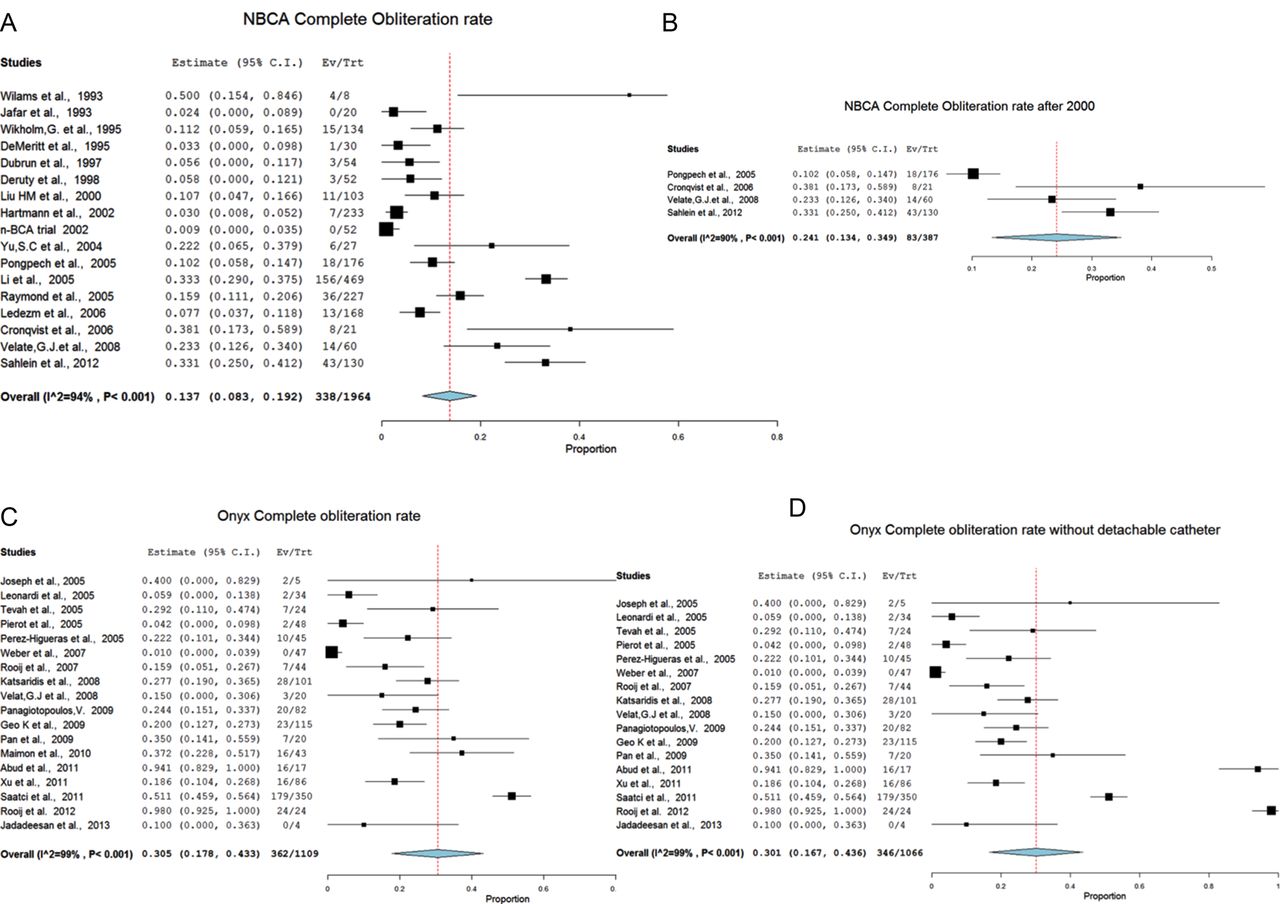
The complete obliteration rate for all NBCA studies was 13.7% (figure 3A). A subgroup analysis of 387 patients in the studies conducted after 2000 showed that the complete obliteration rate with NBCA treatment increased to 24% (figure 3B). The overall EVOH complete obliteration rate was 30.5% (figure 3C) in all studies and 30.1% (figure 3D) in studies that did not use a detachable microcatheter tip. There was a trend towards an increase in obliteration rates in both NBCA and EVOH with time (p=0.03, p<0.001, respectively) (figure 4A, B). The overall OR for complete obliteration was 1.94 (95% CI 0.937 to 4.016; p=0.074) favoring EVOH; this OR decreased to 1.35 in the subgroup analysis after the year 2000 (95% CI 0.72 to 2.54; p=0.34) (figure 4C, tables 4 and 5).
Complication rates between NBCA and Onyx divided before year 2000 and after year 2000
Meta regression comparing the two embolic agents with response to the complication rates and the cure rate
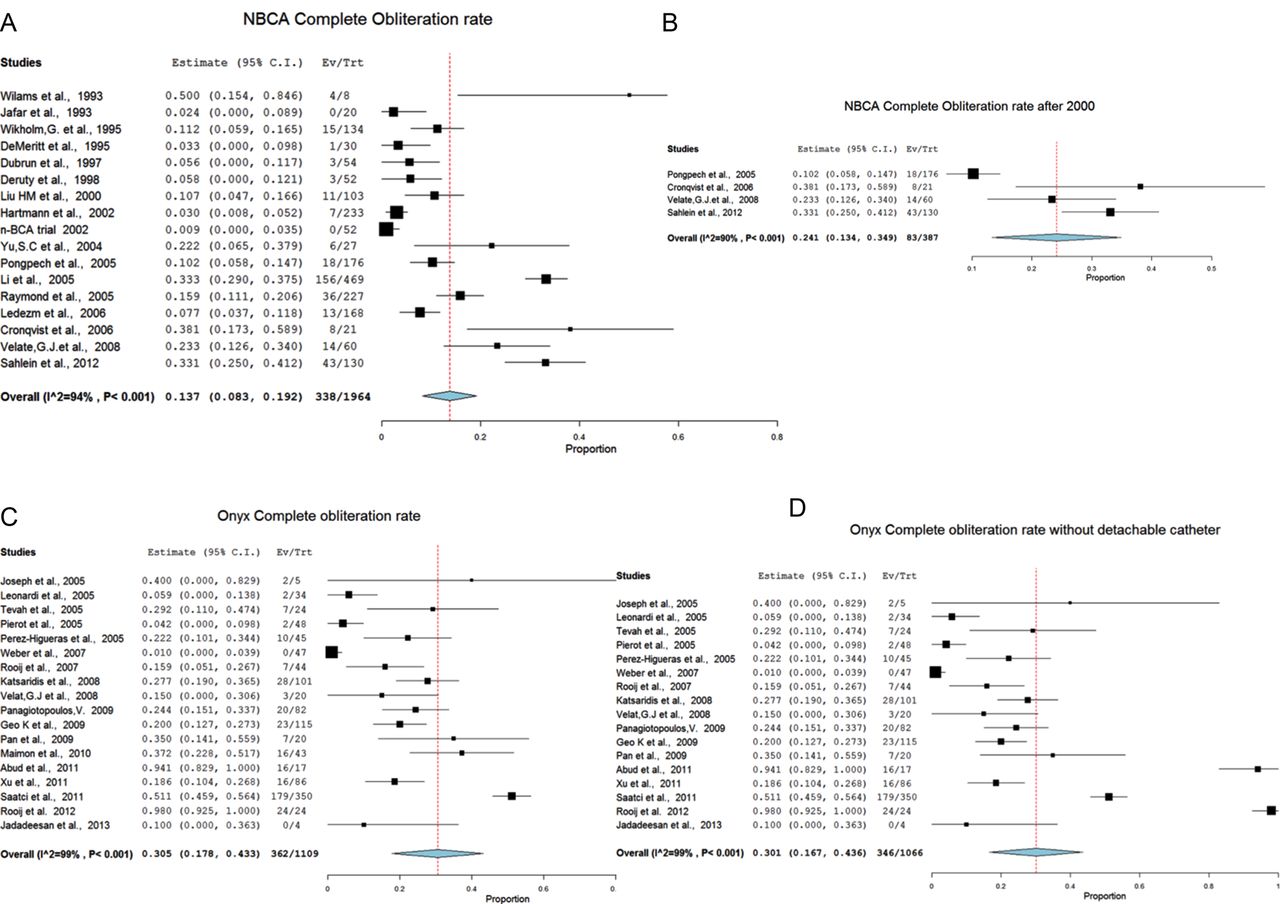
(A) List of published literature and meta-analysis citing complete obliteration rates in patients treated with n-butyl cyanoacrylate (NBCA). Complete obliteration is seen in 13.7%. (B) List of published literature and meta-analysis citing complete obliteration rates in patients treated with NBCA after the year 2000. Complete obliteration is seen in 24.1%. (C) List of published literature and meta-analysis citing complete obliteration rates in patients treated with ethylene-vinyl alcohol co-polymer (Onyx). Complete obliteration is seen in 30.5%. (D) List of published literature and meta-analysis citing complete obliteration rates in patients treated with Onyx; published literature citing the use of detachable microcatheters was excluded and hence there was a decrease in the complete obliteration rate to 30.1%.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Year regression plot for complete obliteration in patients treated with n-butyl cyanoacrylate (NBCA). (B) Year regression plot for complete obliteration in patients treated with ethylene-vinyl alcohol co-polymer (Onyx). (C) OR of complete obliteration in patients treated with NBCA versus Onyx after the year 2000. OR of 1.35 in favor of complete obliteration with Onyx.
Discussion
Our meta-analysis review of endovascular treatment of brain AVMs demonstrated fairly poor outcomes with both agents (5.3% in the NBCA group and 6.8% in the EVOH group), which is similar to a previous meta-analysis involving 975 patients treated with endovascular embolization for brain AVMs. They did not specify which agent(s) was used; the total complication rate leading to permanent morbidity and death occurred in a median of 6.6% of patients, ranging from 0% to 28% after embolization alone.18
Recently there has been a trend towards aggressive embolization of brain AVMs with embolization performed as the sole treatment with intent for cure.14 This trend has gained momentum with the increased utilization of EVOH. EVOH use gives the surgeon a much longer injection rate, without fear of microcatheter retention (especially with the use of detachable microcatheter tips outside of the USA). This is reflected by a steeper rise in cure rates with EVOH compared with NBCA, but also with a trend towards worse neurological outcomes. Conversely, there was a higher cure rate with NBCA (10% before 2000 to 24% after 2000) without a significant increase in poor neurological outcome. These rates could be explained by surgeons gaining experience and working with a better selection of patients without using aggressive embolization with the goal of cure. Although the use of detachable microcatheter tips was introduced in an effort to reduce hemorrhagic complications related to pulling the microcatheter, the current meta-analysis does not support the theory that patients embolized with detachable tip microcatheters have better neurological outcomes. This may be related to the fact that when surgeons using detachable microcatheters became more aggressive with embolization, there were increases in hemorrhagic complications related to venous obstruction instead of microcatheter pulling.
In the recent multicenter clinical trial ARUBA19 (A Randomized trial of Unruptured Brain Arteriovenous malformations; designed to compare medical intervention (embolization, surgical, and/or radiosurgery) with medical therapy of unruptured AVMs), a 30.7% composite endpoint (symptomatic stroke or death) in the intervention arm was reported compared with a 10% endpoint in the medical treatment arm over a mean period of 33 months. Yet in this trial, 30/116 of patients (allocated to the interventional group) were treated solely with AVM embolization, which currently represents an off-label use of these embolic agents (NBCA, EVOH) without surgical resection. This incidence complies with our meta-analysis observation for more aggressive embolization performed with an intention for cure in the most recent literature. The combined poor outcomes in the intervention arm of the ARUBA trial (30%) are much higher than that for embolization reported in our meta-analysis (5.2% for NBCA and 6.8% for EVOH). It is not clear from this trial how much of the poor outcome was related to the embolization, surgical resection, or delayed bleeding from altered AVM flow post embolization. The fact that a large proportion of patients were treated with embolization (alone or in combination with multiple treatment modalities) suggests that a significant morbidity is related to embolization procedures. The study does not report on delayed hemorrhagic complications related to the embolization procedures alone, a phenomenon that may be related to partial embolization (without surgical resection) that might have a worse natural history than untreated AVM. This poor outcome is higher than the rates in published studies for surgical resection of AVMs (0.34–2.2% in grades I–II).20 ,21 This discrepancy might be explained by poor selection of patients and patients treated with the intention to cure with embolization alone (as 25.8% of patients were treated only with embolization procedures).
Our study has some limitations. The validity of a meta-analysis depends on the quality of the selected studies. Most of our selected studies were retrospective, and so our study is limited by the retrospective design of most of the selected studies. Many details were lacking from the included studies, such as recurrence rate, and patients with vein of Galen malformations and associated aneurysms.
Conclusion
NBCA continues to have a trend towards lower permanent complication rates, yet EVOH has higher angiographic cure rates. Recent literature has demonstrated an increase in the cure rate of AVMs with endovascular embolization techniques yet with a possible increase in permanent neurological deficits and mortality. Proper selection of patients remains the most influential determinate of outcome of embolization in patients with brain AVMs.
References
Footnotes
Contributors AE: review of the literature, compiling the data, statistical analysis, and drafting of the manuscript. VAA: concept design, review of the results, and drafting of the manuscript. AA: concept design, statistical analysis, review of the results, drafting of the manuscript, and overall supervision of the project.
Funding The study was partially supported by grant UL1TR000050 awarded to the Center for Clinical and Translational Research at University of Illinois at Chicago.
Competing interests AA and VAA are consultants for Cordis-Codman.
Provenance and peer review Not commissioned; externally peer reviewed.