Article Text

Abstract
Introduction The SILK flow diverter (SFD) is used for the treatment of complex intracranial aneurysms. Small case series have been reported in the literature but few studies with a large number of patients have been published. We present our experience with the SFD for the treatment of intracranial aneurysms in Canada.
Methods Centers across Canada using SFDs were contacted to fill out a case report form for patients treated with an SFD in their center. Individual centers were responsible for approval from their ethics committee. Image analysis was performed by individual operators. The case report forms were collected and the final analysis was performed.
Results A total of 92 patients were treated with SFDs in eight centers in Canada between January 2009 and August 2013. The aneurysms were located in the posterior circulation in 16 patients and in the anterior circulation in 76 patients. Most aneurysms (75%) were saccular in shape; 22% were fusiform and 3% were blister aneurysms. The size of the aneurysms varied from 2 to 60 mm with the neck varying from 2 to 60 mm. Perioperative morbidity and mortality were 8.7% and 2.2%, respectively. At the last available follow-up, 83.1% of the aneurysms were either completely or near-completely occluded. The rate of complications was higher for fusiform aneurysms (p<0.001).
Conclusions The SFD appears to be an important tool for the treatment of complex intracranial aneurysms. Treatment outcomes and complication rates remain a problem, but should be considered in the context of available alternative interventions. Ongoing analysis of flow-diverting stents for radiographic and clinical performance is required.
- Aneurysm
- Device
- Flow Diverter
Statistics from Altmetric.com
Introduction
Flow-diverting stents have emerged as a promising treatment option for complex intracranial aneurysms. A flow diverter is a self-expanding flexible stent constructed of woven strands with a low porosity whose function is to divert blood flow away from the aneurysm into the distal parent artery to exclude the aneurysm sac. These stents limit flow into and out of intracranial aneurysms, resulting in thrombosis of the aneurysm over time.1 The first flow diverter used in clinical practice was the SILK stent (Balt Extrusion, Montmorency, France) in early 2007. The other commonly used flow diverters include the Pipeline device (Covidien, Massachusetts, USA), SURPASS (Surpass Medical, Miramar, Florida, USA), FRED (Microvention, Tustin, California, USA), and p64 (Phenox, Bochum, Germany). Early experience with these devices has suggested a variable rate of aneurysm closure with limited morbidity.2–18 Flow-diverting stents have been used to successfully treat complex aneurysms with limited therapeutic alternatives, yet their role in general aneurysm management remains to be defined. The results of the recently stopped MARCO POLO trial, which compared the outcome of aneurysms randomized to the SILK flow diverter (SFD) and standard endovascular treatment, will be interesting to evaluate in this context.19
Significant complications, such as delayed aneurysm rupture and distal intracerebral hemorrhage, have tempered enthusiasm for its widespread use. Questions remain regarding the overall efficacy of the devices, the morbidity of treatment, long-term outcomes, and the cost-effectiveness of these expensive devices.
There have been a number of case series presented in the literature using flow diverters.2–18 Most of the larger studies are for the Pipeline device. We present the initial Canadian experience with the SFD. This retrospective analysis provides a real-world sense of the efficacy, limitations, and complications associated with it. To our knowledge, this is the largest study reported with a final outcome on the use of the SFD.
Materials and method
This study is a report of a registry of consecutive patients treated with SFDs in eight centers across Canada between January 2009 and August 2013. All centers in Canada using the SFD were contacted to contribute to our registry. However, despite multiple attempts, we believe we could not get information on another 10 patients treated with the SFD in this time interval.
Individual operators at each center were contacted to fill out a case report form for patients in their center. Image analysis was performed by individual operators. The information was then collected and analyzed. All patients were followed according to the standard of care of the individual institutions. At the end of August 2013, all case report forms were sent to Halifax, Nova Scotia where the final analysis was performed. Approval was obtained from the local research ethics board. For the purpose of this study, the data were anonymized and pooled for retrospective analysis. At the time of the study, the SFD was only available through a Health Canada compassionate-use program. The initial cases at each site were proctored by expert users. The SFD was considered primarily for cases where the alternative—either surgery or conventional coiling—was felt to carry either excessive procedural risk or likely to fail to occlude the aneurysm durably. The SFD was also considered as an alternative to vessel sacrifice for the treatment of large complex anterior circulation aneurysms. Additionally, the SFD was considered in patients thought to have segmental wall disease with multiple aneurysms in the same vessel segment. Stent placement and periprocedural management were not standardized but were generally uniform as a result of training by a small group of proctors. All operators were asked whether these aneurysms could be treated by any means other than flow diverters.
The antiplatelet regimen was decided by individual operators. The standard antiplatelet regimen included daily dual antiplatelet medication (81 mg aspirin and 75 mg clopidogrel) starting 4 days before the procedure and continuing for up to 3 months after the procedure. After 3 months most patients were maintained on only one of the two drugs for the rest of their lives.
Where possible, stents were deployed using a triaxial catheter system consisting of a larger shuttle-type guide catheter, a flexible distal access guide catheter, and a microcatheter (Vasco, Balt Extrusion, Montmorency, France). The number of stents deployed and the use of adjuvant coils was at the discretion of the treating physician. Post-deployment angioplasty was occasionally required to address problems with stent kinking and inadequate vessel wall apposition.
Baseline characteristics were recorded, including patient demographics, mode of presentation, and aneurysm specifics such as location, largest diameter (mm), neck width (mm), and morphology. Periprocedural morbidity and mortality (within 30 days of the treatment) were recorded, as were any significant clinical events during follow-up. Standardized outcome assessments were not routinely performed at each institution and therefore could not be included in our analysis.
Radiographic follow-up consisted of a combination of CT angiography (CTA), contrast-enhanced magnetic resonance angiography (CE-MRA), time-of-flight magnetic resonance angiography (TOF-MRA), and digital subtraction angiography (DSA). Follow-up paradigms—in particular, technique and timing—varied between centers. Aneurysm closure was judged using all available radiographic modalities. Aneurysm filling was categorized as no significant change (95–100% of baseline contrast filling), residual aneurysm (5–95% residual filling), near-complete occlusion (entry remnant, 5% residual filling), and complete occlusion (no filling). The parent artery occlusion was considered as no residual filling of the aneurysm. Standardized assessment of contrast stasis was not available for analysis. In-stent stenosis was recorded for patients undergoing DSA whereas the residual aneurysm mass was estimated from cross-sectional imaging (CTA and MRA).
Data analysis
All data were analyzed using Statistics V.18.0 software package (IBM Corporation, Somers, New York, USA). Univariate and multivariate analyses of outcomes were conducted using logistic regression or Cox proportional hazards modeling, along with the χ2 test and independent t test, where appropriate.
Results
A total of 92 patients (20 men, 72 women) of age range 10–83 years (mean 56.96, median 57.5) with 103 aneurysms were treated at the participating centers between January 2009 and August 2013.
Aneurysms
The presentations of the patients are summarized in box 1. More than half (56.5%) of patients were asymptomatic. A detailed summary of aneurysm location is shown in figure 1. The majority of the aneurysms (83%) were located in the anterior circulation, with most (94%) being on the internal carotid artery. In the posterior circulation the majority (49%) of the aneurysms were located on the basilar artery. Most of these aneurysms (75%) were saccular, with 22% fusiform and 3% blister aneurysms. Most aneurysms in this series were large and wide-necked. The mean aneurysm diameter was 14.4 mm (median 12.5 mm, range 2–60 mm), while the mean neck width was 8.6 mm (median 6.8 mm, range 2.7–60 mm). Only six patients in our series had an aneurysm neck of <4 mm. Partial thrombosis of the aneurysm sac was observed in 22.8% of cases.
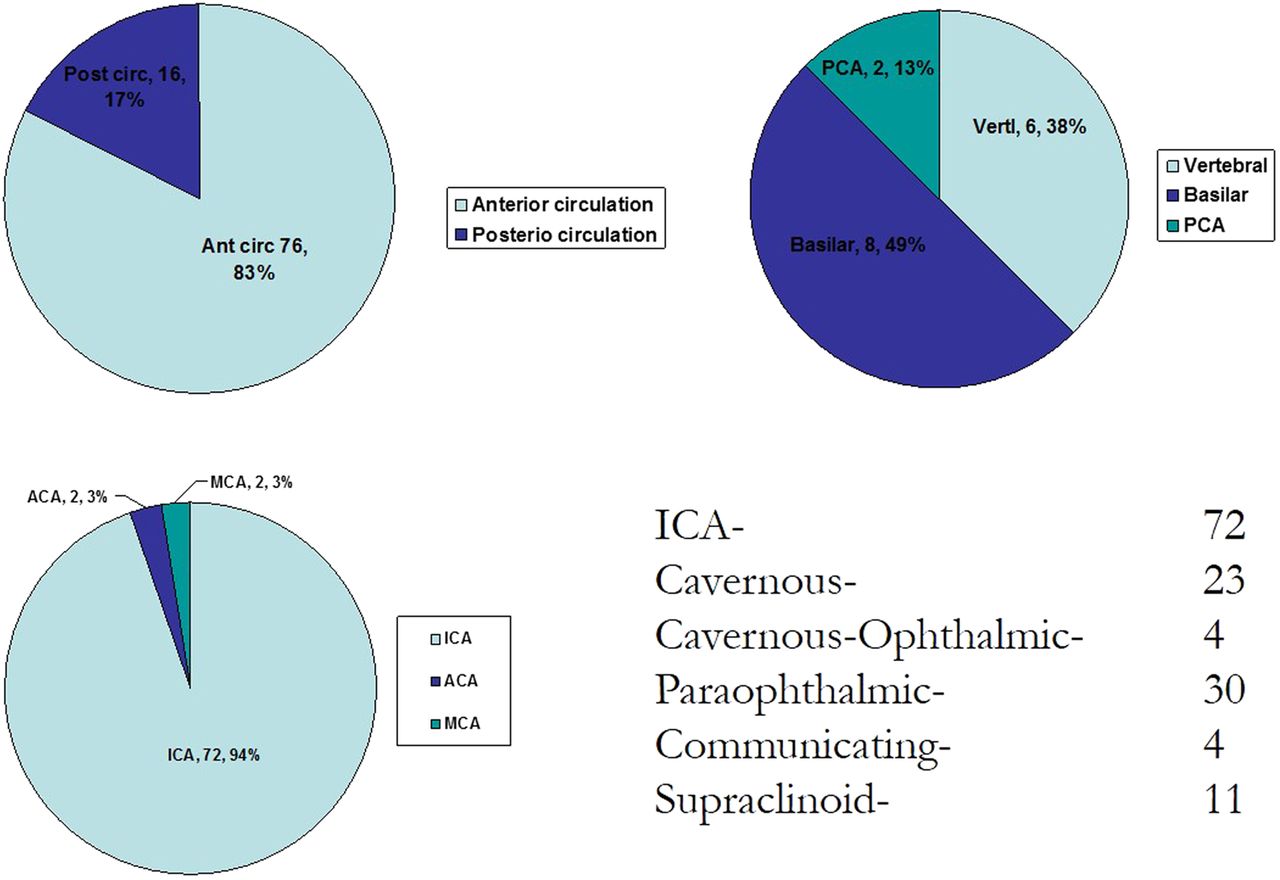
Location of aneurysms in the study.
Clinical presentations of patients in the study
Asymptomatic: 52 (56.5%) (family history: 6)
Symptomatic: 40 (43.5%)
Acute subarachnoid hemorrhage: 7 (17.5%)
Previous subarachnoid hemorrhage: 12 (30%)
Cranial nerve deficit: 17 (42.5%)
Gait disturbance: 1 (2.5%)
Headaches: 3 (7.5%)
Others (dysphagia, vertigo, progressive neurological deficits, epistaxis from pseudoaneurysm by nasopharyngeal carcinoma, hydrocephalus with brain stem compression, progressive increase in size, transient ischemic attack, left cerebellar cerebrovascular accident, bitemporal superior quadrantonopia): 9 (22.5%)
Treatment
According to the operators, 40% of the aneurysms in this series could not have been treated by any means other than flow diverters. A total of 104 SFDs were used in the 92 patients with 103 aneurysms. The majority of these patients (70 patients, 81.4%) were treated with a single SFD, 14 patients (16%) were treated with two SFDs and only two patients (2.3%) were treated with three SFDs. Of the 104 SFDs used, 100 (96.2%) were successfully deployed and only four failed to open.
There was no significant difference in the number of SFDs used based on the shape (saccular vs fusiform) of the aneurysm (p=0.47). Additional coils were placed in the aneurysm sac in 23.3% of cases. In most cases, partial coiling of the aneurysm was undertaken in larger aneurysms. There was also no significant difference in the use of additional devices based on the shape (saccular vs fusiform) of the aneurysm (p=0.69). Anti IIb–IIIa agents were used in 10.5% of patients and steroids were used in 34.9% of patients in the perioperative period.
Clinical outcomes and complications
Device-related periprocedural morbidity and mortality were 8.7% (8 patients) and 2.2% (2 patients), respectively. Of the four patients with technical failure of SFDs, the parent vessel was occluded in two patients without any clinical consequences; the third patient had hemiplegia and the fourth died as a result of technical failure.
Overall, periprocedural hemorrhagic complications were seen in four patients. Of these, two patients developed aphasia and hemiplegia, one patient developed a carotico–cavernous fistula and one patient died. Periprocedural thromboembolic complications (observed on the procedural DSA) developed in 13 patients (15.1%). Of these, 10 patients were treated with anti-IIb–IIIa agents. Six of the 13 patients remained clinically unchanged, two developed transient neurological deficits, and five developed permanent neurological deficits.
There were three deaths in the periprocedural period, only two of which (2.2%) were device-related. The first patient presented with bitemporal superior quadrantanopsia and left hemiparesis and was found to have a 60 mm wide saccular cavernous internal carotid artery aneurysm with a 15 mm neck diameter. A severe in-stent stenosis was noted after deployment of the SFD. The stenosis was re-crossed and another SFD was deployed in a telescopic fashion. No intraprocedural rupture or jets of contrast were noted. However, a post-procedural CT scan showed diffuse subarachnoid hemorrhage. Another patient, who was treated with SFD for a ruptured blister aneurysm, developed vasospasm and died secondary to complications of the subarachnoid hemorrhage and was not included in the final analysis. The third patient with an asymptomatic A1 segment fusiform aneurysm measuring 12 mm in maximum diameter suffered from a large middle cerebral artery territory infarct secondary to incomplete opening of the stent. The patient developed aphasia and hemiplegia and subsequently died secondary to cardiovascular complications during the hospital stay.
At most recent follow-up (3–24 months, median12 months), 88 patients (96.5%) were well, with either no deficit or a stable or improved pre-existing deficit. Two patients developed transient neurological deficit related to parent artery narrowing which improved with reinstitution of antiplatelet medication. Two patients died during the follow-up period. One patient (with a superior cerebellar artery aneurysm) died suddenly 3 months post-procedure. No imaging could be obtained and her family declined autopsy. The other patient (with a 12 mm supraclinoid saccular aneurysm) died of intracranial rupture 1 year post-treatment. The aneurysm did not change in size after treatment and showed an increase in size on follow-up which was treated with a second SFD. The patient developed a subarachnoid hemorrhage after the second treatment and subsequently died.
The overall mortality and permanent morbidity in our series related to SFD were 4.3% (4 patients) and 8.7% (8 patients), respectively.
Radiographic outcomes
Radiological follow-up was available for 77 patients (83.8%). Median follow-up for the entire cohort was 1 year (range 0.25–2 years). At the most recent radiographic follow-up, 83.1% (64 patients) of aneurysms were either completely (61 patients) or near-completely (3 patients) occluded. Aneurysm obliteration was confirmed on DSA in 56%, on CEMRA in 15.8%, on CTA in 15.8%, and on TOF-MRA in 10.5%. Residual filling of the aneurysm was seen in 13 patients (16.9%). The progressive closure of aneurysms over time is shown in figure 2.

{kind=link}
{kind=link}
Progressive closure of aneurysms over 24 months.
Predictors of aneurysm closure were assessed in a univariate proportional hazards model (table 1). Younger patients had a higher chance of complete and near-complete aneurysm closure (p=0.001). Aneurysms in the cavernous (p=0.02) and paraophthalmic (p=0.02) location showed an increased incidence of complete aneurysm closure. No other factors had a significant relationship with the complete and near-complete closure of the aneurysm. Parent artery narrowing was seen in 12 patients (15.6%). The majority of them were asymptomatic; only one patient had transient ischemic attacks. Parent artery occlusion was seen in six patients (7.8%), none of whom were symptomatic.
Predictors of aneurysm closure assessed by univariate analysis. The outcome was dichotomized between residual neck+complete obliteration versus residual aneurysm
Cavernous and paraophthalmic segment aneurysms
Cavernous (n=23) and paraophthalmic (n=30) segment aneurysms represent a unique subset of the overall cohort, 52% presenting with cranial neuropathy. This subset of aneurysms tended to be slightly larger in size (mean diameter 15.8 vs 12.6 mm, p=0.06) but was not significantly different in terms of their neck size (p=0.23). Both minor (p=0.51) and major (p=0.18) complications as well as mortality rate (p=0.35) were very similar to other aneurysms. Complete aneurysm closure was superior (p=0.02) in this location (table 2).
Predictors of aneurysm closure assessed by univariate analysis. The outcome was dichotomized between complete obliteration+residual neck versus residual aneurysm
Fusiform versus saccular aneurysm
Since saccular (n=64) and fusiform (n=17) aneurysms are different pathologies, we compared the complication rate and outcome of the two groups. Device-related morbidity and mortality were significantly higher for fusiform aneurysms than for saccular aneurysms (17.6% and 5.9% vs 7.8% and 0%, respectively; p<0.001). At the last available follow-up there was no significant difference in the complete and near-complete obliteration rate in fusiform and saccular aneurysms (84.6% vs 82.8%; p=0.87).
Treatable versus not treatable aneurysms
The aneurysms in 32 patients (40%) were considered impossible to be treated by any other means than flow diverters. The device-related morbidity (9.4%) and mortality (3.1%) in this group was higher than the morbidity (2.1%) and mortality (2.1%) for rest of the patients but was not statistically significant (p=0.14 for morbidity and p=0.77 for mortality). At the last available follow-up there was a trend toward a higher rate of complete and near-complete obliteration rate for this group of aneurysms compared with the rest of the aneurysms (96% vs 82.5%; p=0.097).
Discussion
While the SFD and Pipeline device are the most commonly used flow diverters, there is a paucity of literature on the SFD. In fact, our series is the largest series on the use of SFDs which includes the final occlusion rate. The Italian multicenter study with 142 patients treated with SFDs only reported the perioperative results and did not report the aneurysm obliteration rate.14
Our Canadian experience with the SFD demonstrates effective angiographic closure of the treated aneurysms, with 83% complete or near-complete occlusion during an average follow-up period of 1 year. It is important to note that the aneurysms in our study were larger and had a wider neck than in the other published series. Despite this, the results are comparable with other studies in the literature which have reported angiographic aneurysm occlusion rates of 74–94%.2–18 In the current study, younger age of the patient at the time of treatment was found to be a significant predictor of complete obliteration of the aneurysm. The most favorable results in our series came from the subset of patients with cavernous and paraophthalmic location aneurysms. These aneurysms were not significantly different in their morphological characteristics from aneurysms at other locations and the complications associated with them were also not significantly different from that of aneurysms at other locations. We believe that location itself is probably favorable for treatment with flow diverters. Similar findings were shown by O’Kelly et al.7 Flow-diverting stents may represent an important treatment option for patients with cavernous and ophthalmic location aneurysms. However, proximal occlusion has also been shown to be a safe and effective treatment in appropriately selected patients.20
The perioperative device-related complications in our series of 10.9% (2.2% mortality, 8.7% morbidity) are comparable to other studies.2–18 These complications are higher than those associated with routine endovascular treatment of aneurysms. Allowing for overlap of specific complications, the overall permanent morbidity and mortality rate in this series is 13% (4.3% mortality, 8.7% morbidity). The aneurysm obliteration rate appears to be lower and the complication rate appears to be higher compared with some other series in the literature.2–18 The relative efficacy and morbidity of this treatment must be considered in the context of available alternative interventions. The morbidity and mortality was significantly higher (p<0.001) for fusiform aneurysms than for saccular aneurysms, where there are limited alternative interventions. The aneurysm obliteration rate with SFDs was similar for fusiform and saccular aneurysms (84.6% vs 82.8%). According to the operators, around 40% of aneurysms in our study were deemed impossible or too risky to be treated with routine endovascular or microsurgical treatments. A trend towards a higher aneurysm obliteration rate for this group compared with the rest of the aneurysms (96% vs 82.5%; p=0.097) suggests that SFDs may be more useful for aneurysms which are deemed impossible or too risky to be treated by routine endovascular or microsurgical treatments.
Surgery for giant aneurysms using bypass and proximal occlusion techniques has a reported mortality of 13% and permanent neurologic morbidity of 9%.21 Similarly, in a series of 105 patients with hypothermic circulatory arrest at the Barrow Neurological Institute, the combined procedure-related morbidity and mortality was 32%.22 Additionally, conventional endovascular approaches such as coiling with balloon or stent assistance may have a relatively lower procedural risk but these interventions have been shown to have diminished efficacy for large complex aneurysms leading to an increased risk of recurrence and retreatment. In a systematic review of giant aneurysms treated with conventional endovascular approaches, the complete occlusion rate was 57%, with recanalization in 27%.23 The rates of morbidity and mortality were 17% and 8%, respectively.23
We observed delayed narrowing of the parent artery in 12 patients (16%) and parent artery occlusion in six patients (7.8%). The incidence of parent artery occlusion has been reported to be as high as 12–28%.10 ,13 ,18 This may be related to the response/resistance of platelets to antiplatelet medications. At the time of the registry there were no means available for testing platelet response/resistance in most of the institutions. The importance of this is being increasingly emphasized in the use of flow diverters. However, the method and results of these tests are yet to be standardized. Increased use of platelet inhibition assays will allow us to identify non-responders to these medications and the use of alternative antiplatelet agents may ultimately minimize thromboembolic complications. In our series, only one of the patients with parent artery occlusion presented with transient ischemic attack. All other patients remained asymptomatic on follow-up. In-stent stenosis, with a unique behavior, is a frequent angiographic finding observed after flow-diverter stent implant. The stenosis is usually asymptomatic; however, close clinical and angiographic monitoring is mandatory for individualized management.24
Given that flow-diverting stents are a relatively recent innovation, their performance during long-term follow-up needs to be evaluated. The mean follow-up in our series was 1 year (range 0.25–2 years). The majority of the patients in our series were followed up by CEMRA but most of the aneurysm obliteration (56%) was confirmed with DSA. CTA can be used for follow-up if no additional devices (such as coils) were used for the treatment of the aneurysm. TOF-MRA is not useful for follow-up assessment as it shows false positive obliteration of the aneurysm and false positive in-stent stenosis. DSA remains the best modality to follow these patients. However, CEMRA can be effectively used for sequential follow-up in all patients, thereby reducing the need for frequent DSA.25
Although all flow diverters act on the same basic principle, they are slightly different in terms of their design and technique of use. Compared with the Pipeline, the other commonly used flow diverter, an average of 1.1 SFDs was used per patient in our registry. An additional SFD was used only when the first SFD did not completely cover the neck of the aneurysm for technical reasons. This potentially makes the SFD cost-effective and technically simpler.15 The proximal holding mechanism of the SFD enables it to be retrieved and reused even when up to 80% of the device is deployed. This was thought to be an important safety mechanism for SFD by the operators in our registry.
The purpose of our study was to report our experience with a novel technology used to treat challenging intracranial aneurysms and to highlight early technical and clinical problems. In theory, SFDs can be used for any type of aneurysm but concerns remain about their use in bifurcation aneurysms and whether they are worth using in small saccular aneurysms with a low recurrence rate after coiling.26 We believe that randomized trials are needed to determine the relative efficacy of flow-diverting stents compared with standard aneurysm treatment.
Study limitations
This study has a number of limitations as it is a retrospective and non-randomized study. Outcomes were self-reported by the treating interventionalist resulting in potential measurement bias. Pre- and post-procedural management was not standardized and was done according to the institutional protocol. Standardized outcome measures such as angiographic grading scales and clinical outcome scales were not uniformly reported and therefore were not available for complete analysis.
The study is also limited by the loss to follow-up of 10 patients. Based on the patient, aneurysm and initial treatment results, these patients were not different from the rest of the patients; however, this has potential for selection bias.
Conclusions
Overall, the SFD appears to be an important tool for the treatment of complex intracranial aneurysms, particularly for aneurysms which are deemed impossible or too risky to be treated with routine endovascular or microsurgical treatments. Treatment outcomes and complication rates remain a problem, but should be considered in the context of available alternative interventions, particularly for fusiform aneurysms. Ongoing analysis of flow-diverting stents for radiographic and clinical performance is required.
References
Footnotes
This paper was presented at the ASNR 2014 Meeting in Montreal, Canada.
Correction notice This article has been corrected since it published Online First. Figure 1 has been replaced.
Contributors JJSS: project development, data collection, manuscript writing. DT, DI, MC, RA, TK, JW, PL, JG and BS: data collection. KR: statistical support. AW: data Collection, manuscript writing.
Competing interests JJSS and TK are proctors for Silk flow diverter in Canada.
Ethics approval All human and animal studies have been approved by the multiple ethics committees including Capital Health ethics committee, Halifax and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Patient consent All patients gave informed consent prior to inclusion in this study.
Provenance and peer review Not commissioned; externally peer reviewed.