Article Text

Abstract
Background Flow diversion is an important tool for treatment of cerebral aneurysms, particularly large and giant aneurysms. The Surpass flow diverter is a new system under evaluation in the USA.
Objective To report our initial experience of 20 cases with the Surpass flow diverter to demonstrate its basic properties, the required triaxial delivery platform, and the methodologies used to deploy it during treatment of large internal carotid artery (ICA) aneurysms
Methods Twenty patients with ICA aneurysms ≥10 mm with ≥4 mm neck treated as part of the Surpass IntraCranial Aneurysm Embolization System Pivotal Trial (the SCENT trial; Stryker) were included. Details of patient demographics, aneurysm characteristics, and technical procedures were collected.
Results Twenty patients (mean age 63.3±1.3 years; range 51–72) with 20 unruptured aneurysms (mean size 13.4±0.9 mm; range 10–21 mm) were treated. For proximal access, 60% of cases had aortic arch ≥grade II, 55% had significant cervical ICA tortuosity, and 60% had cavernous ICA ≥grade II. The Surpass device was implanted in 19/20 (95%) cases. Of 19 cases, a single device was used in 18 cases (95%) and 2 devices in only 1 case (5%). Balloon angioplasty was performed in 8/19 cases (42%). Complete aneurysm neck coverage and adequate vessel wall apposition was obtained in all 19 cases.
Conclusions Surpass is a next-generation flow diverter with unique device-specific and delivery-specific features compared with clinically available endoluminal flow diverters. Our initial experience demonstrates a favorable technical profile in treatment of large and giant ICA aneurysms.
Trial registration number NCT01716117.
- Aneurysm
- Catheter
- Device
- Flow Diverter
- Stent
Statistics from Altmetric.com
Introduction
Flow diversion has emerged as a game-changing endovascular treatment for cerebral aneurysms. Safety, efficacy, and durability have been shown in its initial target aneurysm population, specifically large and giant wide-neck internal carotid artery (ICA) aneurysms.1–3 Beyond this, flow-diverting devices have also been used with success to treat small anterior circulation ICA aneurysms,4 ,5 dissecting aneurysms,6 ,7 posterior circulation aneurysms,8 ,9 anterior cerebral artery aneurysms,10 and middle cerebral artery aneurysms.11
The Pipeline embolization device (PED) is currently the only Food and Drug Administration (FDA) approved flow-diverting device in the USA. It is a 48-strand cobalt–chromium braided mesh device that is delivered through an empty 0.027″ inner diameter (ID) microcatheter. Considering both the success and limitations of the PED, alternative flow-diverting strategies have been developed and implemented in Europe and abroad.12–15 Each of these other flow-diverting stents has a unique implant design and delivery platform.
The Surpass flow diverter (Stryker Neurovascular) is one such device undergoing evaluation in an investigational device exemption clinical study in the USA. In this report, we present our initial experiences using the Surpass device in 20 ICA aneurysms with the aim to demonstrate the basic properties of the device, the required triaxial delivery platform, and the methodologies used to deploy it during treatment of large ICA aneurysms.
Patients and methods
Patients
Between October 2013 and August 2014, an attempt was made by the department of neurosurgery to treat a total of 20 aneurysms in 20 patients with the Surpass flow diverter at the Johns Hopkins University (Baltimore, Maryland, USA). All patients were enrolled in the Surpass IntraCranial Aneurysm Embolization System Pivotal Trial to treat large or giant wide-neck aneurysms (the SCENT trial; Stryker). The SCENT trial is a prospective, multicenter, single-arm trial for FDA approval of the device. Patients enrolled and included in this study had aneurysms ≥10 mm with a ≥4 mm neck located on the ICA up to the termination. The allowed vessel diameters for the implant were ≥2.5 and ≤5.3 mm. Patient demographic data, aneurysm characteristics, and technical details of the interventional procedure were collected.
Device
Technical details of the Surpass flow diverter have been previously described.12 Briefly, the Surpass device is a low-porosity mesh tubular structure constructed of cobalt–chromium alloy intertwined with platinum–tungsten wires for visibility. The device is designed to maintain constant pore density over various diameters of the device. The 3 mm and 4 mm devices have 72 wires, and the 5 mm device has 96 wires. The Surpass device is preloaded at the distal end of a microcatheter delivery system that consists of a 0.040″ ID delivery catheter (microcatheter) and pusher. The entire delivery system is advanced over a 0.014″ microwire inserted through the pusher. The implant is deployed by a combination of advancing the pusher and unsheathing the microcatheter.
Endovascular procedure and access system
Aneurysm treatments were performed on a biplanar flat-panel angiographic system (Artis zee, Seimens, Erlangen, Germany) and under general anesthesia. All patients were preoperatively treated with a dual antiplatelet regimen of aspirin 325 mg daily and clopidogrel 75 mg daily for 7 days. Platelet inhibition was verified according to institutional protocol. Systemic anticoagulation was instituted with heparin and activated clotting time was checked according to protocol. Parent vessel size measurements were determined from calibrated standard digital subtraction angiography (DSA) images.
For all procedures, a triaxial system was used through an 8F femoral access. This consisted of a 6F 087 Flexor shuttle guiding sheath (Cook Medical, Bloomington, Indiana, USA) or an 8F 088 Neuron MAX delivery catheter (Penumbra, Alameda, California, USA), a 5F Navien (058, 115 cm) distal intracranial support catheter (Covidien, Mansfield, Massachusetts, USA) and an XT-27 0.027″ ID microcatheter (Stryker Neurovascular) or Surpass delivery system. The Surpass was deployed under real-time visualization using a combination of native fluoroscopy (7.5 pulses/s), roadmap, and DSA (three frames/s). Proper device expansion and deployment was assessed with native fluoroscopy and DynaCT. Balloon angioplasty was used for postprocessing of the implant when appropriate for improved vessel wall apposition. Control DSA was performed immediately after deployment and at 5 and 10 min after deployment to confirm vessel wall apposition, patency of the parent vessels, and to rule out intraluminal thrombus.
Data collection and statistical analysis
Details of patient demographics, aneurysm characteristics, procedural equipment, grade of the aortic arch, tortuosity of the cervical ICA (defined as a 90° turn, hairpin turn, or corkscrew loop), and grade of the cavernous ICA were collected.16 Data were presented as counts, percentages, and means. When means were presented, the SEM was used to assess sample distribution.
Results
A total of 20 aneurysms in 20 patients were treated. The details of each case are presented in tables 1 and 2. Three cases have been highlighted in figures 1⇓–3.
Patient demographics, aneurysm characteristics, and access
Case properties and technical details

Surpass embolization of 19 mm previously coiled Pcom aneurysm with neck residual in a sexagenarian. (A) Pre-embolization digital subtraction angiography (DSA) angiography (lateral view) of right-sided 19 mm previously coiled Pcom aneurysm with neck residual. (B) The Navien catheter (black asterisk=tip of Navien catheter) advanced to the supraclinoid internal carotid artery (ICA) proximal to the aneurysm. The Surpass delivery system (black arrow=microcatheter tip; white arrow=distal marker of pusher) is being advanced through the Navien. (C) Lateral and (D) transorbital oblique views of the Surpass delivery system navigated past the aneurysm and into the right M1. The Navien tip has withdrawn to the posterior genu. The constrained Surpass device (4 mm×25 mm; black arrowheads) is visualized in the delivery microcatheter. (E) Lateral and (F) transorbital oblique views demonstrating deployment of the distal Surpass device. The Navien was advanced over the Surpass delivery system into the supraclinoid ICA. The distal device (white arrowhead) was deployed with a ‘push’ by advancing the pusher. (G) The device was ‘corked’ by withdrawing the pusher (white arrow) to the microcatheter tip (black arrow). The distal device (white arrowhead) was then repositioned into the M1 segment and out of the bifurcation. (H) Oblique and (I) lateral views demonstrating further deployment of the Surpass device from the M1 to the ICA using a combination of unsheathing with significant forward pressure on the pusher to titrate the opening of the device. (J) Deployment of the proximal device in the straight supraclinoid ICA by unsheathing. After processing of the proximal device, balloon angioplasty was then performed (not shown). (K) Oblique and (L) lateral cine views demonstrate good vessel wall apposition of the device (white arrowhead). (M, N) Final control angiography demonstrates normal filling of the jailed right anterior cerebral artery and significant contrast stasis in the aneurysm that persists into the venous phase (black arrow).
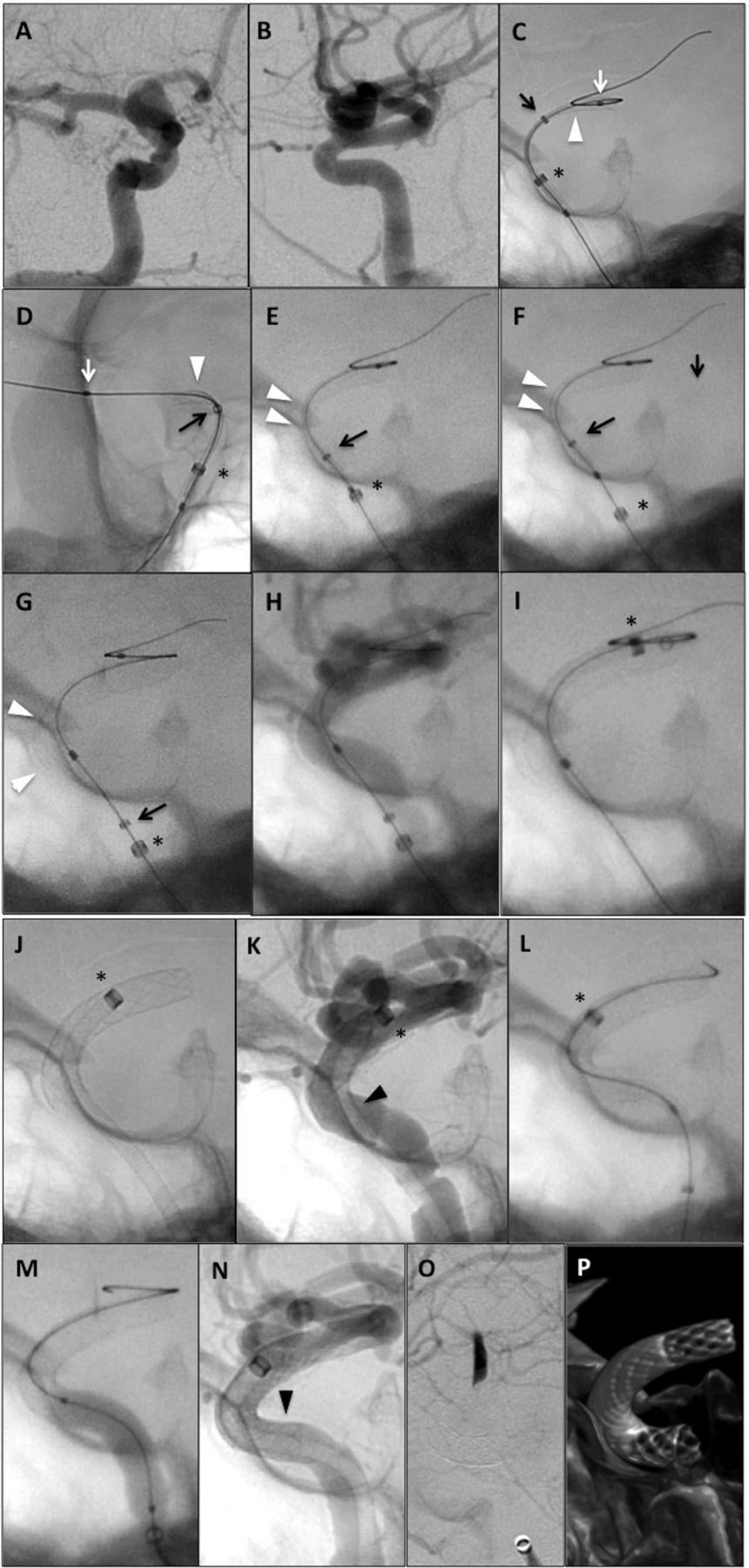
Surpass embolization of 11 mm ophthalmic aneurysm in a sexagenarian. (A) Oblique and (B) lateral pre-embolization digital subtraction angiography (DSA) of right-sided 11 mm ophthalmic aneurysm. (C) lateral and (D) oblique views demonstrating deployment of the distal Surpass device. With the Navien positioned in the distal cavernous internal carotid artery (ICA) (black asterisk=tip of Navien catheter) the device (4 mm×15 mm) was ‘pushed’ out of the microcatheter (black arrow=microcatheter tip) by advancing the pusher (white arrow=distal marker of pusher). The distal portion and belly of the device have been deployed. Improved wall apposition of the device around the anterior genu is achieved by the ‘loading technique’ (E and F), whereby the microcatheter is advanced 1–2 mm with the pusher locked in position, thereby loading the entire system. The Navien tip slides backwards with this maneuver. (G) The proximal device was then deployed with mainly a push of the pusher, allowing the microcatheter to slide back on its own. The pusher was then manipulated back and forth to improve opening of the device. (H) Cine fluoroscopy to assess vessel wall apposition. (I) The Navien is advanced to an endoluminal position by first advancing the microcatheter over the pusher and then tracking the Navien within the Surpass device over the microcatheter. (J) The Surpass delivery system is removed, leaving only the Navien endoluminal within the device. (K) Cine fluoroscopy demonstrates a small region of malapposition (black arrowhead). (L) A second surpass device (4 mm×15 mm) was deployed with the proximal landing zone in the horizontal cavernous ICA. (M) Balloon angioplasty was performed to improve vessel wall apposition of the construct. (N) Final cine fluoroscopy shows excellent apposition of proximal device construct (black arrowhead). (O) Final control DSA demonstrating significant contrast stasis in the aneurysm that persists into the venous phase. (P) DynaCT reconstructed images of the two-device construct.
{kind=link}
{kind=link}
{kind=link}
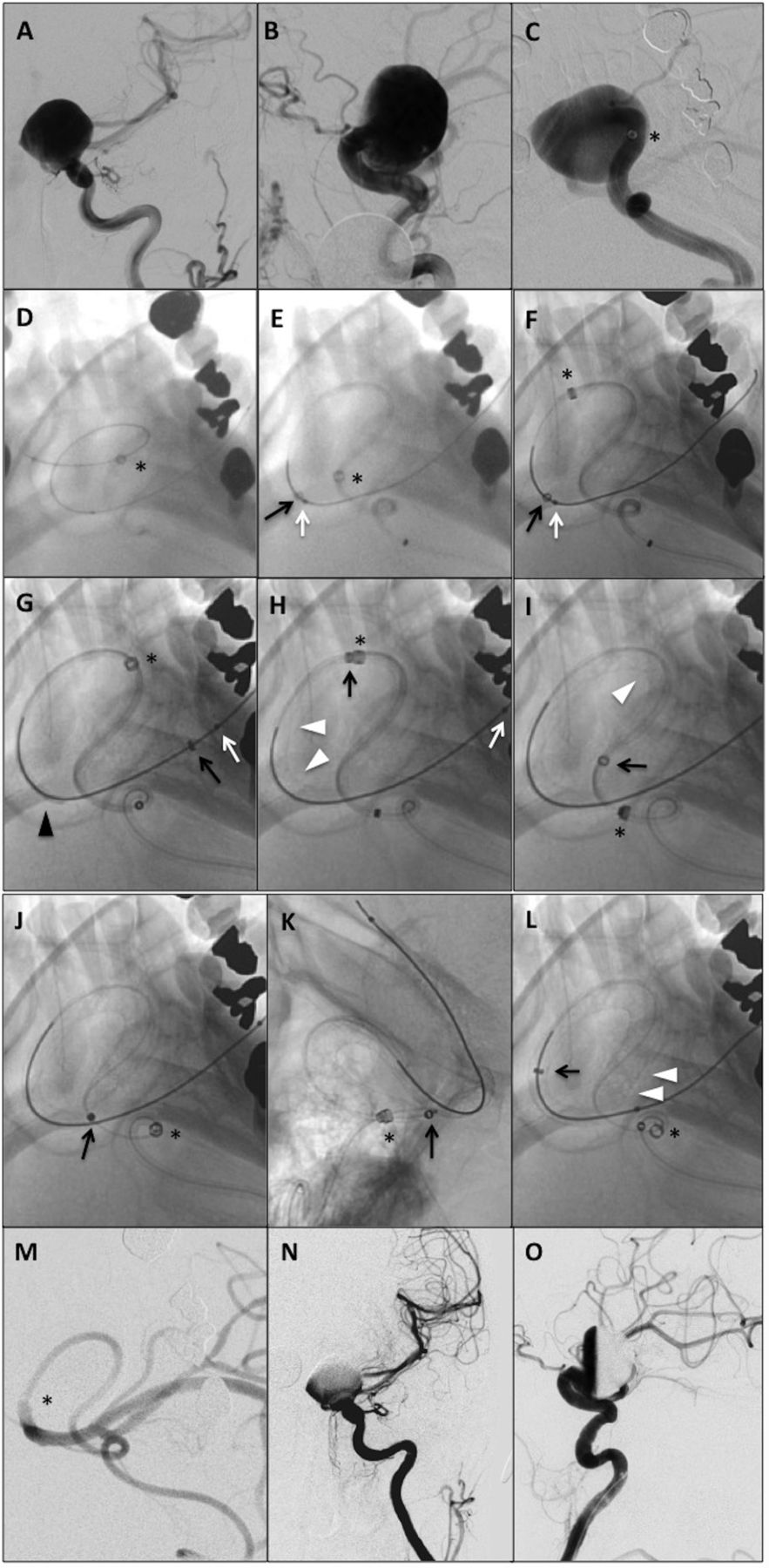
Surpass embolization of previously wrapped, enlarging 21 mm supraclinoid aneurysm in a septuagenarian. (A) Anteroposterior (AP) and (B) lateral pre-embolization digital subtraction angiography (DSA) of left-sided supraclinoid 21 mm aneurysm. (C) Steep caudal/submental view demonstrating the aneurysm outflow tract and the Navien tip in the distal cavernous internal carotid artery (ICA) (black asterisk). (D) The aneurysm was crossed with a SL-10 microcatheter (Stryker Neurovascular) and Synchro-2 standard microwire (Stryker Neurovascular). (E) The Surpass Halo delivery system (white arrow=pusher tip, black arrow=microcatheter tip) was then advanced over an exchange length Chikai 0.014″ wire (Asahi Medical, Japan). (F) The Navien was advanced over the delivery system into the supraclinoid ICA. (G) The delivery system was advanced until the constrained Surpass device (4 mm×40 mm; black arrowhead) was at the distal landing zone. (H) The distal device was deployed (white arrowheads) by retracting the microcatheter with forward pressure on the pusher. (I) Belly of the device (white arrowhead) easily deployed around the anterior genu demonstrating reliable and consistent opening of longer length devices. (J) Steep caudal and (K) lateral views of the proximal device deployed with unsheathing and pushing. (L) The microcatheter was advanced endoluminally over the pusher into the distal device, resulting in improved opening of the proximal device (white arrowheads). The Navien catheter was then tracked over the Surpass delivery system into the M1, and the delivery system was removed. (M) DSA from the Navien demonstrated patency of the middle cerebral artery. With the Navien still endoluminal within the Surpass device, DSA was performed from the shuttle catheter to confirm patency of the ICA and evaluate vessel wall apposition of the device (not shown). The Navien was then withdrawn into the proximal ICA for final control DSA. (N) AP and (O) lateral final control DSA demonstrating significant contrast stasis in the aneurysm and improved opacification of the distal vasculature.
Patient and aneurysm characteristics
Mean patient age was 63.3±1.3 years (range 51–72). Eighteen patients (90%) were women and two (10%) were men. All aneurysms were in the anterior circulation, with the majority being ophthalmic ICA aneurysms (60%). The mean aneurysm size was 13.4±0.9 mm (range 10–21 mm). For aneurysm morphology, 13/20 (65%) aneurysms were saccular, and 7/20 (35%) were fusiform (defined as involving >25% of the parent vessel wall). Of the 20 aneurysms treated, 11/20 (55%) had no prior treatment, 5/20 (25%) were previously coiled, 2/20 (10%) were previously clipped, and 2/20 (10%) had prior treatment with cotton wrapping.
Proximal vascular characteristics
Aortic arch type, cervical ICA tortuosity, and cavernous ICA grade were used as surrogate markers of access and procedural complexity. A grade I aortic arch was present in 8/20 (40%) patients, grade II arch in 10/20 (50%) of cases, and grade III arch in 2/20 (10%) of cases. Significant cervical ICA tortuosity was present in 11/20 cases (55%). Tortuosity was defined as a 90° turn, hairpin turn, or corkscrew loop. There was a wide distribution of cavernous ICA grades among the 20 patients, with 1/20 (5%) grade IA, 6/20 (30%) grade IB, 5/20 (25%) grade II, 7/20 (35%) grade III, and 1/20 (5%) grade IV.
Procedure characteristics
Triaxial systems were used in each case, consisting of a Neuron MAX catheter (17/20 cases, 85%) or Shuttle (3/20 cases, 15%), a 5F Navien catheter, and an XT-27 microcatheter. Exchange techniques were used to advance the Surpass delivery system in 2/20 (10%) of cases, both of which were for the treatment of near-giant aneurysms 19–21 mm in size. After processing of the deployed Surpass device, balloon angioplasty was performed in 8/19 cases (42%) with implantation. Mean heparin dose for the 20 cases was 6170±220 U (range 4400–7000 U), and mean contrast dose was 73±8 mL (range 35–200 mL). Mean fluoroscopy time for the cases was 54.6±7.8 min (range 20.8–182.5 min), and mean radiation dose was 2680±358 mGy (range 680–6966 mGy).
A Surpass device was implanted in 19/20 (95%) cases. In case No 17, the aneurysm could not be crossed by the Surpass delivery system, and a device was not implanted. Attempts to track an empty 0.027″ catheter across the aneurysm neck and into position for PED deployment were also unsuccessful. Of the 19 cases with implantation of a Surpass device, a single Surpass device was used in 18/19 (95%) of these cases. In order to optimize vessel wall apposition, two Surpass devices were implanted in one case (1/19, 5%). Proper vessel wall apposition was achieved in all cases with an implanted device.
Highlighted cases
Case No 9
This is the case of a sexagenarian with a previously coiled 19 mm posterior communication artery aneurysm who underwent flow diversion with the Surpass device system for treatment of an aneurysm neck remnant (figure 1). This patient had complex proximal access, with a type II aortic arch, cervical ICA tortuosity, and a grade III cavernous ICA. As shown in figure 1, the highlights of this case are (1) the distal landing zone of the Surpass in the middle cerebral artery (MCA), (2) using the ‘corking’ technique whereby the pusher is pulled proximally onto the distal end of the device to adjust the position of the distal device, (3) selection of a straight segment of the supraclinoid ICA for the proximal landing zone, and (4) use of cine to assess wall apposition of the device.
Case No 10
This is the case of a sexagenarian with an 11 mm ophthalmic aneurysm found incidentally during investigation for ear pain. As shown in figure 2, the highlights of this case are (1) the “loading” technique to facilitate device opening and improve vessel wall apposition, (2) achieving postdeployment endoluminal access with the 5F Navien catheter to facilitate placement of a second Surpass device, (3) use of a second device to correct a region of malapposition, and (4) the use of balloon angioplasty when needed.
Case No 14
This is the case of a septuagenarian with a remote history of craniotomy for cotton wrapping of a large supraclinoid aneurysm with documented interval aneurysm growth, now measuring 21 mm. This patient had complex proximal access, with a type II aortic arch and a grade III cavernous ICA. As shown in figure 3, the highlights of this case are (1) use of intracranial exchange to advance the Surpass delivery system, (2) the trackability of the Surpass 040 catheter in significant tortuosity, (3) the ‘climbing’ technique to advance the 5F Navien over the Surpass delivery system, (4) use of longer (40 mm) devices that reliably open without twisting, and (5) utility of a postdeployment 5F Navien catheter retrack to improve device opening and vessel wall apposition.
Discussion
Here we present our initial technical and procedural experiences using the new Surpass flow diverter in 20 ICA aneurysms. Flow diversion has emerged as a game-changing treatment for cerebral aneurysms. An increasing number of reports have demonstrated the efficacy and safety of flow diverters for treatment of various classes of cerebral aneurysms, including the initially targeted large and giant wide-neck ICA aneurysms1–3 ,17 ,18 as well as other classes of anterior circulation aneurysms4–7 ,10 ,11 and posterior circulation aneurysms.8 ,9 Concurrently, the introduction of advanced distal intracranial support catheters has enabled and facilitated use of new sophisticated interventional devices, such as flow diverters.18 ,19 The marriage of device and catheter technology has advanced the field of flow diversion, with increased safety and efficacy, and also improved cost-effectiveness20 and decreased radiation exposure21 compared with more traditional endovascular aneurysm treatments, such as coiling.
The Surpass flow diverter and delivery system
The Surpass device implant is a braided mesh stent composed of strands of cobalt–chromium alloy with 12 marker wires of platinum and tungsten for visualization under fluoroscopy. The device is manufactured in diameters of 1 mm increments (eg, 3, 4, and 5 mm), compared with the PED, which is available in smaller 0.25 mm increment diameters from 2.5 mm to 5 mm. The strand number of the Surpass also varies with device diameter, whereas the PED has a fixed number of 48 strands regardless of device diameter. Surpass devices 3 and 4 mm in diameter have 72 strands, and 5 mm devices have 96 strands. The pore density of the device ranges from 21 to 32 pores/mm2. Sadasivan et al22 demonstrated in a rabbit elastase-induced aneurysm model that pore density (number of pores/mm2), as opposed to porosity (metal-free to total covered surface area), is a more important factor for modulating the efficacy of flow-diverting devices. Devices with high pore density and low porosity are thought to be more efficacious. By increasing strand count in larger diameter devices, the Surpass maintains a more consistent pore density than other flow diverters with fixed strand number regardless of diameter.
The percentage foreshortening of a Surpass device varies depends on device diameter, with 38%, 42%, and 26% foreshortening expected for devices of 3 mm, 4 mm, and 5 mm in diameter, respectively. Based on our experience in this series, the Surpass device foreshortens significantly less than a similar-sized PED. The strand count and design of the Surpass device mesh are thought to facilitate device opening.
The Surpass device is packaged preloaded on a pusher within a delivery 0.040″ microcatheter. The Surpass device is on ‘rails’ in between two radiopaque markers, but it is not constrained at its distal or proximal ends. The pusher has a lumen that accommodates a standard 0.014″ microwire that can move independently of the implant. The PED and the FRED, in contrast, are both constrained on a delivery wire. The Surpass delivery system (0.040″ ID, 3.6–3.7 Fr outer diameter (OD)) is larger than a PED delivery system (0.027″ ID, 2.8–3.2 Fr OD) secondary to the size of the 0.040″ ID microcatheter and presence of an indwelling pusher. It is the presence of the pusher that decouples the device from the microwire. The only length of delivery system currently available in the USA investigational device exemption trial is 135 cm. This is targeted and works well for its intended use in large ICA aneurysms.
Navigation and deployment
Advancing the Surpass delivery system is performed with a triaxial access platform consisting of a stable guide catheter/sheath (eg, Shuttle or Neuron MAX) in the proximal ICA, the hyperflexible 5F Navien distal access catheter in the distal ICA, and the Surpass delivery system. The Navien is positioned using either of two main techniques. The first method is to advance the Navien over a 0.027″ microcatheter (eg, XT-27) and appropriate microwire. The second method, named the ‘climbing’ technique, involves advancing the Navien over the Surpass delivery system in a stepwise fashion towards the aneurysm until a distal position of the Navien is obtained. The choice of method depends on the vessel tortuosity, aneurysm size, and aneurysm type. The climbing technique is preferred when possible, as it eliminates the extra steps of advancing a 0.027″ microcatheter distally. For large/giant aneurysms or situations of extreme vessel tortuosity, crossing the aneurysm first with a 0.017″ catheter might be required followed by intracranial exchange for the Surpass system (similar to empty 0.027″ catheter platform). Once the Surpass system is in position across the aneurysm, the Navien can be further advanced over it in a ‘slip-tip’ fashion to provide extra support if needed (figure 3).
The larger size of the Surpass delivery system makes tracking and navigation generally more difficult than flow diverters deployed through an empty 0.027″ microcatheter. However, once in position the Surpass delivery system is more stable. This provides the platform for highly accurate distal device placement. Significant improvements in ‘softness’ and trackability were seen over the course of the experience as numerous engineering modifications were made to the Surpass 0.040″ catheter. Although not quantifiable, we believe these improvements facilitate deployment and allow complex and tortuous cases such as case No 14 (figure 3) to be treated with consistency.
Selection of landing zones is important for Surpass cases, as with procedures using other flow diverters, and straight segments are preferred for both distal and proximal landing sites. Opening the device in a straight segment helps to facilitate adequate vessel wall apposition. This is most important for the proximal device. Suboptimal vessel wall apposition of the proximal device can increase the procedural risk of thromboembolism and/or endoleak. During treatment of a paraophthalmic aneurysm, the preferred proximal landing zone is the horizontal segment of the cavernous ICA. If the device used is too short and lands in the anterior genu, a second device can be used to extend the construct and optimize the apposition (figure 2).
The design of the Surpass implant and delivery system allows for precise positioning of the constrained device at the targeted distal landing zone. The preferred method of positioning the distal device using the Surpass system is called ‘carrying the device’ to the target. This technique involves advancing the entire Surpass delivery system (with device inside) so that the constrained device is positioned at, or just distal to, the distal target zone. This contrasts with techniques used by our group and others to deploy the distal PED by opening the PED in the MCA and dragging it back to position in the ICA. An alternative technique for deploying the distal Surpass device is to position the microcatheter tip at the distal landing zone and push the device out with the pusher. This technique was used frequently during the initial European experience, but has fallen out of favor in North America owing to the re-engineered softer and a more trackable Surpass 0.040″ catheter.
Deployment of the Surpass device is a two-handed technique with the left hand in control of retracting the microcatheter and the right hand in control of the pusher and wire. The distal device is best deployed with an initial unsheathe from the microcatheter while maintaining mild forward system load with the pusher and Navien. Once about 10 mm of the device is deployed, additional forward pressure is applied to the microcatheter (pusher locked) to facilitate opening of the device. This maneuver is known as a ‘load’ or ‘loading technique’. Unlike the current version of PED available in the USA, where the distal device is constrained on a capture coil, the distal Surpass device is unconstrained and independent of wire torque. The wire is best positioned in a MCA division (preferably large and straight) during deployment of the Surpass device in the ICA. The wire is closely monitored throughout the case to ensure safe and continuous wire access across the system.
The belly of the Surpass device is deployed across the neck of the aneurysm with a combination of push and some retraction of the microcatheter. This portion is best done with a push, while allowing the delivery microcatheter to slide back passively. The push helps to facilitate device opening of this braided device as it comes out of the microcatheter. For the Surpass, this can be performed on the outside curvature of the vessel (eg, anterior wall of the anterior genu), which contrasts with the primary use of mid-vessel to the inner curvature for PED deployment. Since the Surpass device is not constrained on a delivery wire, long segments of device can be deployed reliably and consistently.
The landing zone for proximal device deployment is preferably in a straight segment. This is done mainly by retraction of the microcatheter with some forward push of the pusher. In our series, the proximal Surpass device opened completely in 100% of cases using this technique. No ‘string-like’ segments of proximal device or partial openings were seen. After release of the proximal device, the pusher is withdrawn a short distance. This maneuver releases tension from the entire system, facilitates expansion of the device to the inner curvature of the vessel (eg, anterior genu), and results in improved device opening and vessel wall apposition. Afterwards, the pusher is then advanced over the microwire so that the proximal bumper is endoluminal in the Surpass device. The microcatheter is then advanced over the pusher to an endoluminal position. Finally, the 5F Navien is tracked over the microcatheter. These maneuvers facilitate opening of the device and assure robust endoluminal access with the Navien catheter for either postprocessing (eg, balloon angioplasty) or for telescoping a second Surpass device if needed. If the microcatheter or Navien cannot be advanced to an endoluminal position, the standard microwire is removed and an exchange-length wire introduced. The exchange wire is used to maintain endoluminal access for balloon angioplasty or for advancing a second Surpass delivery system. Cine fluoroscopy, with injections through the Shuttle or Neuron MAX, is used throughout deployment to assess vessel wall apposition. In our experience, visibility of the Surpass device with standard fluoroscopy is similar to visibility with the PED. Once the device is adequately opposed, the entire Surpass delivery system can be removed. Final DSA runs are performed through the Navien catheter. Flat-panel CT imaging is performed to assess the device and apposition.
Conclusion
The Surpass flow diverter is a new endoluminal device for treatment of large and giant wide-neck ICA cerebral aneurysms currently being evaluated for FDA approval in the SCENT trial. The delivery system allows for torque-free, over-the-wire deployment of the device that maintains a continuous endoluminal wire access that is uncoupled from the deployment. The use of distal access catheters (such as the 5F Navien) allows for tracking of the Surpass system to the required position even in cases with extreme tortuosity. Our initial experience, presented in this report, demonstrates a favorable technical profile for use of the Surpass device for flow diversion of ICA aneurysms.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors GPC collected and analyzed the data, drafted the manuscript, and critically revised the manuscript for important intellectual content. L-ML assisted in critically revising the manuscript and analyzing the data. JMC assisted with the data collection and analysis. BJ helped to draft the manuscript. BM assisted with data collection. JH and RJT critically reviewed the important intellectual content. ALC conceived the idea, performed data analysis and critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Competing interests ALC is a proctor for the Surpass device (Stryker Neurovascular, Fremont, California, USA) and a consultant for Stryker Neurovascular, a proctor for the Pipeline embolization device (Covidien, Mansfield, Massachusetts, USA) and a consultant for Covidien, a proctor for the FRED (flow re-direction endoluminal device) device (Microvention, Tustin, California, USA) and a consultant for Microvention. GPC is a consultant for Covidien and Microvention. The other authors have no conflict of interest.
Ethics approval This research was approved by the Johns Hopkins institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.