Article Text

Abstract
Background The angioarchitectural features of an arteriovenous malformation (AVM) provide key information regarding natural history and treatment planning. Because of rapid filling and vascular overlap, two-dimensional (2D) and three-dimensional (3D) digital subtraction angiography (DSA) are often suboptimal for evaluation of these features. We have developed an algorithm that derives a series of fully time-resolved 3D DSA volumes (four-dimensional (4D) DSA) at up to 30 frames/s from a conventional 3D DSA. The temporal/spatial resolution of 4D reconstructions is significantly higher than that provided by current MR angiography and CT angiography techniques. 4D reconstruction allows viewing of an AVM from any angle at any time during its opacification. This feasibility study investigated the potential of 4D DSA to improve the ability to analyze angioarchitectural features compared with conventional 2D and 3D DSA.
Methods 2D, 3D, and 4D DSA reconstructions of angiographic studies of six AVMs were evaluated by three cerebrovascular neurosurgeons and one interventional neuroradiologist. These observers evaluated the ability of each modality to visualize the angioarchitectural features of the AVMs. They also compared the information provided using the combination of 2D and 3D DSA with that provided by a 4D DSA reconstruction.
Results By consensus, 4D DSA provided the best ability to visualize the internal features of the AVM including intranidal aneurysms, fistulae, venous obstructions, and sequence of filling and draining. 2D and 3D images in comparison were limited because of overlap of the vasculature.
Conclusions In this small series, 4D DSA provided better ability to visualize the angioarchitecture of an AVM than conventional methods. Further experience is required to determine the ultimate utility of this technique.
- Arteriovenous Malformation
- Angiography
- Technique
- Vascular Malformation
Statistics from Altmetric.com
Introduction
The presence of intranidal aneurysms, venous ectasias, venous stenosis, patterns of filling and drainage, location (supratentorial vs infratentorial and superficial vs deep locations), and direct arterial venous fistula are all considered important factors in predicting the natural history of an arteriovenous malformation (AVM).1 ,2 Although non-invasive techniques such as CT and MRI are widely used for imaging of AVMs, conventional catheter angiography is still considered the gold standard.3 However, because of the combination of rapid filling and vascular overlap, conventional two-dimensional (2D) digital subtraction angiography (DSA) images may be suboptimal for evaluation of these angioarchitectural features. The use of three-dimensional (3D) DSA may partially overcome this limitation but, because the 3D models are not time-resolved and comprise all the vascular structures opacified during the acquisition, vascular structures that are adjacent to one another are often obscured by superimposition. We have recently developed an algorithm that allows reconstruction of a conventional 3D DSA acquisition into a series of fully time-resolved 3D DSA volumes—that is, four-dimensional (4D) DSA—at frame rates of up to 30/s. These 4D DSA images provide higher temporal and spatial resolution than current MR angiography and CT angiography.4 Because the 4D reconstructions allow viewing of the vasculature from any angle at any time point, it was our hypothesis that the 4D DSA would facilitate evaluation of complex vascular lesions by providing the ability to view the anatomy not only in any desired view but also to do this at any desired phase of vascular filling, thereby eliminating the problem of vascular overlap.4 Since a single 4D DSA provides this capability, we also believe that this will reduce the need to obtain multiple 2D acquisitions, thus reducing the radiation exposure and contrast medium dose required for a comprehensive angiographic evaluation. This study investigated the feasibility for 4D DSA to offer these advantages when used for assessment of complex AVMs.
Materials and methods
Patient selection
Under an institutionally approved protocol, 2D, 3D, and 4D DSA image data were acquired in nine consecutive patients with AVMs or atrioventricular fistulae (AVFs) who underwent selective catheter angiography between July 2013 and December 2013. Of the nine patients, only six had complete 2D, 3D, and 4D studies for review. One patient with a very small intraorbital venous malformation was excluded from analysis due to lack of visualization of the malformation in all datasets. In the other two the 3D acquisition protocol was not long enough to allow full visualization of the venous drainage of the AVM.
The cases and a brief description of the AVMs are shown in table 1. The ages ranged from 24–67 years. Eight were supratentorial and one was infratentorial.
Demographic characteristics of patient population
Angiography and image processing
Angiography was performed using a commercial biplane angiography system (Siemens Artis zee biplane; Siemens Healthcare, Forchheim, Germany). Using standard angiographic techniques, all patients were studied with 2D and 3D DSA acquisitions as felt necessary by the operator. The 3D acquisitions for all of the AVMs were done using a 12 s rotational acquisition. This protocol acquired 304 projections over a 260° rotation over 12 s. A 6 s acquisition, which consisted of 177 projections acquired over a 260° rotation for a duration of 6 s, was used only for the patient with dural AVF. In all patients a hand injection of contrast was used for the 2D acquisitions; a power injection was used for the 3D acquisitions. The injection rate for the power injector was 3 mL/s with no X-ray delay for a duration of 6 s (6 s protocol) or 8 s (12 s protocol). There was no dilution of the contrast medium. All 2D and 3D DSA data were transferred to a research workstation running both commercial software (syngo X-workplace VB21, Siemens Healthcare, Forchheim, Germany) and the 4D DSA prototype software. Automated 4D DSA reconstructions were performed for all datasets. The result of the reconstruction is a series of fully time-resolved 3D volumes with a temporal sampling of approximately 30 volumes/s. Once reconstructions were completed, the imaging data were stored on the research workstation until the time of evaluation.
Image evaluation
The ability to visualize intranidal aneurysms, fistulae, venous obstructions, and the sequence of arterial filling and venous drainage as well as the overall quality of each image was assessed individually by three fellowship trained cerebrovascular neurosurgeons and one interventional neuroradiologist. No clinical data were provided.
The reviewers were first presented with the 2D DSA images, followed by the 3D DSA images, and then finally with the 4D DSA images. Each reviewer was asked to complete an evaluation form assessing each of the abovementioned characteristics in a commonly used four-point grading scale.5–7
Once the images were scored for each modality, the reviewers were asked to state if any one modality was acceptable as a single imaging modality that provided all necessary information to evaluate the AVM and plan a treatment strategy. Thus, in total, the four reviewers evaluated six cases yielding 24 independent evaluations for 2D, 3D, and 4D DSA.
Results
For three of the six patients (50%) there was 100% agreement among the four evaluators that 4D DSA was sufficient to be used as a standalone modality and was also the preferred modality. For these patients, by consensus, 4D DSA also provided the best overall ability to assess the angioarchitectural features of the vascular malformation. 2D and 3D images in comparison were of limited utility, largely because of the presence of overlap of the vasculature.
For two of the remaining patients (33%) there was agreement among two of the four reviewers (50%) that 4D DSA was the most useful modality. The two other reviewers (50%) thought that 2D DSA was the preferred modality. In one case (17%) there was no consensus agreement among the reviewers regarding the preferred modality.
Illustrative patients
Patient 1
The patient had an incidental finding of a right frontal AVM measuring 2×4 cm. The arterial supply was from the lenticulostriate arteries, the anterior choroidal artery, and the lateral posterior choroidal branch of the right posterior cerebral artery. Venous outflow was exclusively through the galenic system, which was dilated and tortuous, with a venous varicosity of the internal cerebral vein.
A flow-related aneurysm present on a lenticulostriate artery supplying the AVM was not recognized on the 2D or the 3D image. It was partially obscured by overlapping vessels. This abnormality was more clearly seen on the early time frames of the 4D DSA, as illustrated in figure 1.

Flow-related feeding artery aneurysm. The left panel shows a two-dimensional digital subtraction angiography (2D DSA) image, the middle panel shows a three-dimensional DSA image, and the right panel shows an early time frame of a four-dimensional (4D DSA) image. A very small aneurysm is clearly visible inside the blue circle, which is more clearly visualized in the 4D DSA image with elimination of vascular overlap.
There was also an intranidal aneurysm present in the inferior anterior portion of the nidus (figure 2). This was identified prospectively only on 4D reconstructions by two out of the four reviewers; in retrospect, the others agreed it was present on 4D but still could not clearly identify it on 2D or 3D. As shown in figure 2, this aneurysm is hardly visible on the 3D DSA and clearly visible on the 4D reconstruction.

Intranidal aneurysm. The left panel shows a two-dimensional digital subtraction angiography (2D DSA) image, the middle panel shows a three-dimensional (3D DSA) image and the right panel shows a four-dimensional (4D DSA) image. The aneurysm can hardly be visualized on 3D DSA due to overlap, while it is clearly visible using an early time frame of 4D DSA.
The sequence and full extent of the arterial feeders can also be better visualized on 4D DSA, as illustrated in online supplementary video 1.
Patient 3
The patient had a large right frontal AVM discovered during investigation for orthostatic falls. The supply came from the right middle cerebral artery (MCA), anterior cerebral artery via the left internal carotid artery/anterior communicating artery with a minimal contribution from the right posterior cerebral artery. The nidus has two large fistulous components supplied by two cortical branches of the MCA. One of these was visualized on the 3D DSA while both were visualized well on the 4D DSA, as illustrated in figure 3.
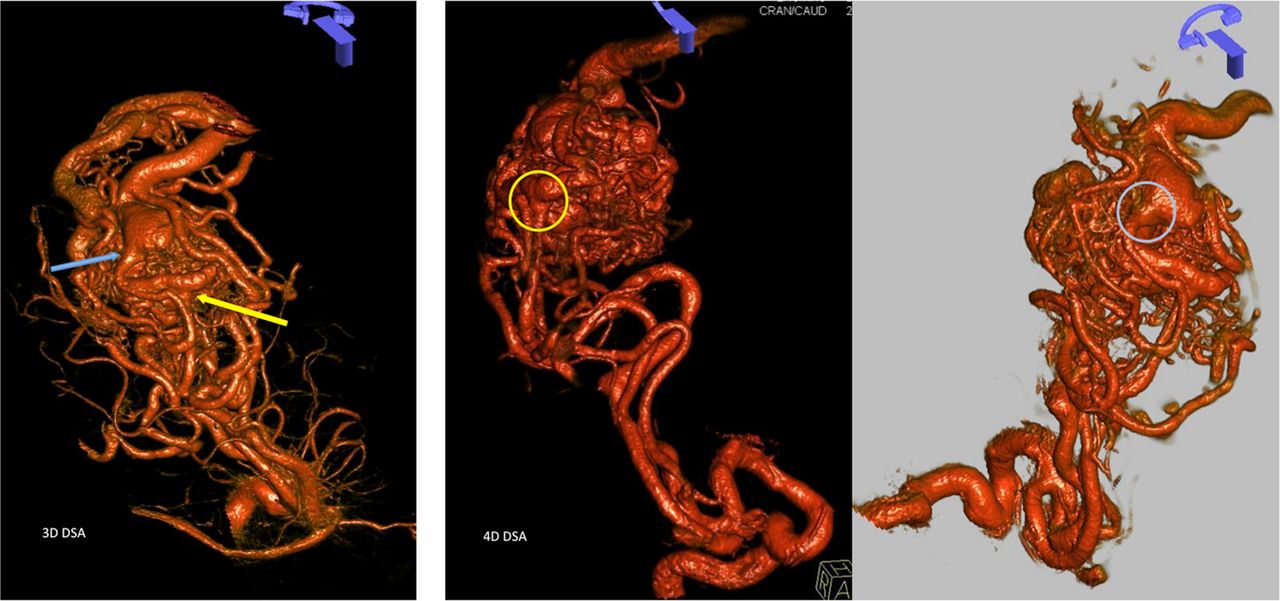
The three-dimensional image (left panel) shows one fistula clearly (blue arrow) while the second one is not well visualized (yellow arrow) due to vessel overlap. Four-dimensional digital subtraction angiography allows two views (middle and right panels) from separate early time frames, each showing one of the direct artery-to-vein fistulae.
Discussion
A detailed understanding of the vascular anatomy and angioarchitectural characteristics of a vascular malformation is helpful both in estimating the risk of bleeding and in treatment planning. In this feasibility study we have demonstrated how the availability of time-resolved 3D images (4D DSA) can enhance the ability to obtain this information. Because of the extremely rapid opacification of complex AVMs, images from conventional angiograms are often inadequate to show the malformation features clearly. This is sometimes the case due to vascular overlap, even if the images are obtained at rapid frame rates, from a variety of projections, and despite attempted microcatheter injections aimed at providing images that will allow ‘dissection’ of the AVM nidus. While 3D reconstructions allow an AVM to be viewed from any angle, vascular overlap is an intrinsic feature of the technique. This is true because the 3D models comprise data from a series of rotational projections, each one obtained with vascular structures fully opacified. The 3D reconstruction consists of what might be thought of as the weighted average (sum) of these projections, thus making it impossible to see the features present during early filling of the nidus. Areas of the vascular anatomy without significant vessels in proximity (eg, the cavernous segment of the internal carotid artery) are therefore well visualized while dynamic vascular pathology in close proximity or subject to significant overlap can be poorly represented. 4D DSA allows for full utilization of the spatial and temporal information obtained during a 3D acquisition.
The projections for a 4D DSA are acquired by starting the rotational acquisition just before or simultaneous to the contrast medium entering the vasculature. This allows the contrast bolus to be ‘tracked’ through the vasculature so that, when the projections are reconstructed, the opacified vasculature can be viewed at any time point and at any angle. It also allows for the reconstruction of a standard 3D DSA without loss of anatomic information. Thus, the projections acquired for 4D DSA can also be used to reconstruct a conventional 3D DSA. In our experience, such 3D DSAs have comparable image quality to 3D DSA acquired using a standard injection protocol—for example, rotation started after initial filling of the vasculature. Figure 4 illustrates the rapid filling of the AVM in one of the patients in our series and the several earlier time points at which the malformation can be studied in comparison with the single fully opacified view provided by a standard 3D image. Once again, the 4D technique allows any view to be obtained at any time during the passage of the contrast bolus.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Left panel: a fully reconstructed three-dimensional image. The overlapping arteries and veins obscure the angioarchitecture of the nidus. Right panel: two views of a series of time frames from the four-dimensional digital subtraction angiography reconstruction showing the rapid filling of the arteriovenous malformation. Each image is separated by 0.2 s. Notice how the structures seen on the earlier time point are obscured by overlapping vessels at a later time.
With 4D DSA the treatment planning phase of the intervention may be condensed and simplified. The viewer can ‘dissect’ the nidus of an AVM, looking at the malformation from any desired view while displaying the sequences of filling and drainage at time intervals as short as 1/30th of a second. This is not possible with any other imaging technique. We believe that 4D DSA will expand the ability to assess the risk of bleeding and enhance treatment planning through improved understanding of the vascular anatomy/angioarchitecture. It is also possible that, by reducing the need for multiple 2D DSAs, this technique could decrease the X-ray and contrast medium dose required for angiographic evaluations. Our study did not directly address this potential benefit.
In our practice a typical angiographic assessment of an AVM would consist of a 2D DSA biplane acquisition with injection into all the major vessels supplying the lesion. This would then be followed by a rotational 3D DSA acquisition, which is used to identify possible useful 2D projections. Often multiple 2D images are acquired in order to understand the arterial input, nidus, and venous outflows. Additional 2D images are acquired which identify the route of the supplying arteries to the nidus without vascular overlap. If there is an additional supply to the malformation from a second or third artery, this sequence would be repeated until the entire arterial input has been evaluated. Our proposed workflow would replace 3D DSA with 4D DSA. Again, this may potentially mitigate the need for multiple 2D acquisitions resulting in equivalent or decreased radiation or contrast dose.
We have not formally assessed the advantages and disadvantages of different viewing formats for the 4D DSA reconstructions. Overall, the reviewers agreed that both surface rendered and maximum intensity projection (MIP) displays each had advantages. For example, MIP visualization seemed to provide superior small vessel details over surface rendering. Because of the difference in contrast concentration in arterial and venous structures, images viewed as MIPs were also helpful in differentiating arteries from veins, especially those that were in or immediately adjacent to the nidus. Our reviewers found that the volume rendered images provided better details of the morphology of the vascular anatomy as well as a better understanding of the depth and spatial relationship of the vascular structures.
We have insufficient experience to predict the role that 4D DSA may take in the diagnosis and endovascular treatment of patients with cerebrovascular diseases. Our initial impression is that it will be particularly useful in conditions like AVMs and AVFs where the understanding of high flow and complex anatomy are key in the therapeutic decision-making process. However, it may also be useful in understanding flow-related details of aneurysms and, as has been seen before, possibly in the critical evaluation of patterns of collateral flow in ischemic disease.8
The time required for reconstruction of a 4D DSA is minimal (2 min currently for the 6 s acquisition protocol and 3 min 30 s for a 12 s). This means that 4D studies will be available for review in a time frame that will not detract from the current workflow. Our implementation of the software is a prototype and not optimized for performance. The software, memory allocation, and data output are the same for either protocol.
This study was limited by the small number of malformations evaluated. Despite the limitation, we believe that this series clearly shows the feasibility of creating 4D DSA reconstructions that provide information that is either not available with other techniques or that is more clearly and easily seen than is the case with other techniques. There could be an observer bias introduced by the order in which images were evaluated as 4D reconstructions were always presented after 2D and 3D images. Future studies randomizing the order in which images are shown to the evaluators could potentially limit this possibility. Studies to understand the differences in various acquisition and injection protocols are underway. Optimization of current protocols and further investigation looking into additional applications of this technology and indications for its use are also ongoing.
Conclusion
Although this was a small study with limited scope, the results indicate that 4D DSA potentially provides better ability to visualize the angioarchitcture of an AVM than conventional 2D and 3D DSA. Eliminating vascular overlap and providing an ability to see any time point of filling from any angle enables one to visually dissect the nidus of an AVM in a way that cannot be achieved using conventional methods.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video
Footnotes
Contributors All authors made substantial contributions to the conception, acquisition, analysis, and interpretation of data for the paper, have participated in the drafting and final revision of the content and agree to be accountable for all aspects of this work.
Funding This work was supported by National Institutes of Health grant number R01 144-PRJ68DN.
Competing interests None.
Ethics approval Ethics approval was obtained from the University of Wisconsin Ethics Committee and IRB Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All our data are deposited in a password-protected institutional database concordant with previously approved hospital protocols. Anonymised imaging data are available on reasonable request.