Article Text

Abstract
The WEB is an endovascular flow-disrupting device used in treating wide-necked intracranial aneurysms. Although the device is available in varying sizes, large aneurysms pose a challenge with the need for custom-made devices. We describe the use of coils as an adjunct to the WEB device in successfully treating large aneurysms in two patients, one with an acutely ruptured aneurysm. This novel technique of jailing a microcatheter, deploying the WEB and then coiling the aneurysm saves the need for intracranial stenting, thereby avoiding the need for antiplatelet therapy, which is of benefit in the setting of acute aneurysm rupture.
- Aneurysm
- Device
- Subarachnoid
Statistics from Altmetric.com
Background
The WEB device is a new addition to the armamentarium of embolization agents available for treating intracranial aneurysms and is particularly suited for treating wide-necked aneurysms.1 Although suitable for the treatment of wide-necked aneurysms, aneurysm size is a limitation as larger devices need to be custom made. The largest ‘off the shelf’ WEB device currently available measures 11 mm×9 mm. We overcome this challenge by the concurrent use of coils as an adjunct, also alleviating the need for an intracranial stent and, therefore, dual antiplatelet therapy. This technique of WEB-assisted coiling (WAC) is particularly useful in managing patients with acutely ruptured aneurysms where there is an increased risk of ventriculostomy-related hemorrhage in patients on dual antiplatelet therapy, which is a requirement for stent-assisted coiling.2 Avoiding a stent may also be of benefit in patients with unruptured aneurysms as stent-assisted coiling poses more risks than coiling without a stent.3 The WEB device is used to seal the neck of the aneurysm while coils are used to fill the dome and any residual space left by the WEB device to achieve adequate aneurysm packing, thereby minimizing the risk of recurrence. WAC may also potentially shorten the procedure time, with benefits of reduced irradiation and shortened anesthetic time compared with coiling alone with an assist device.
Case presentations
Case 1
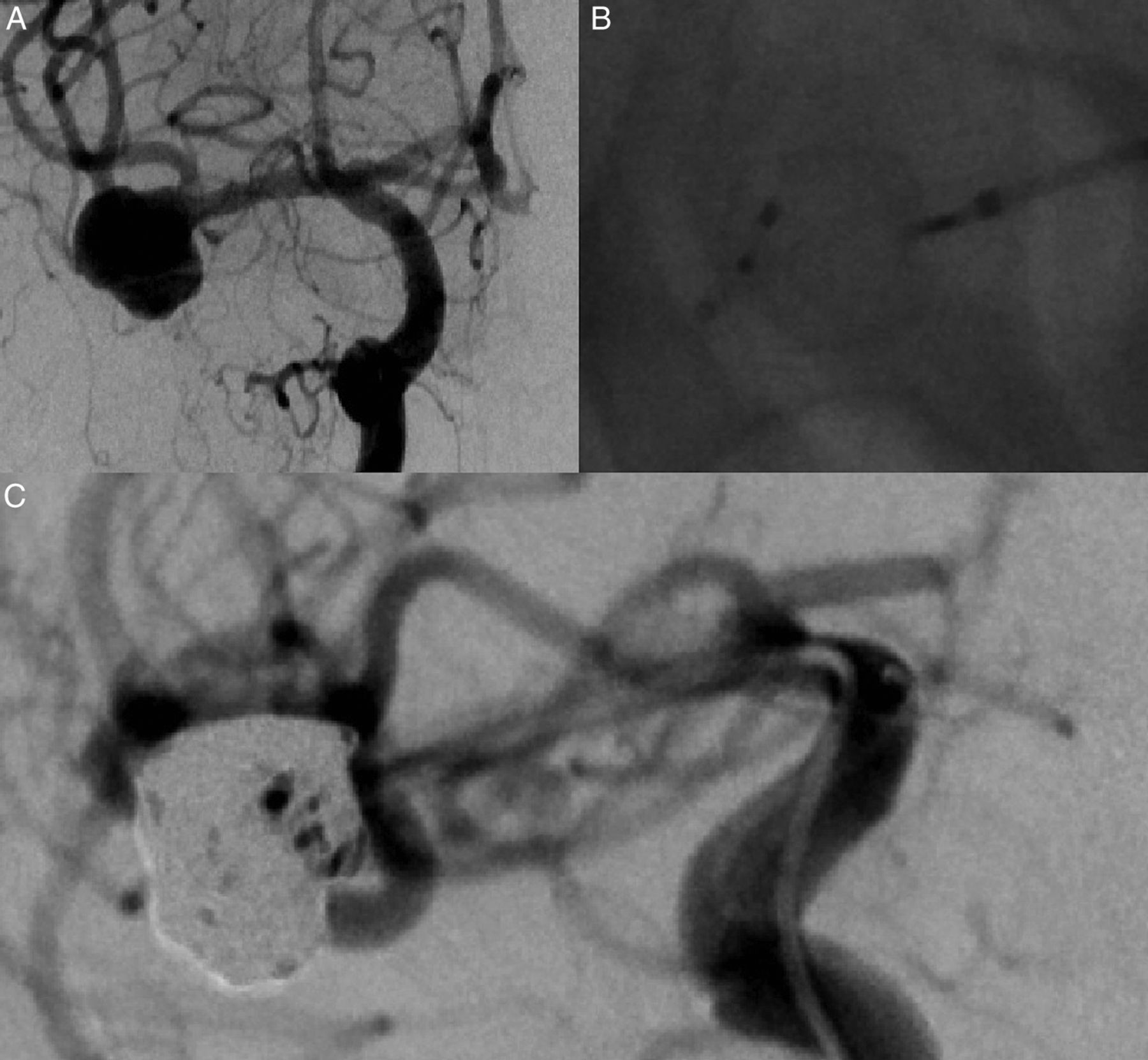
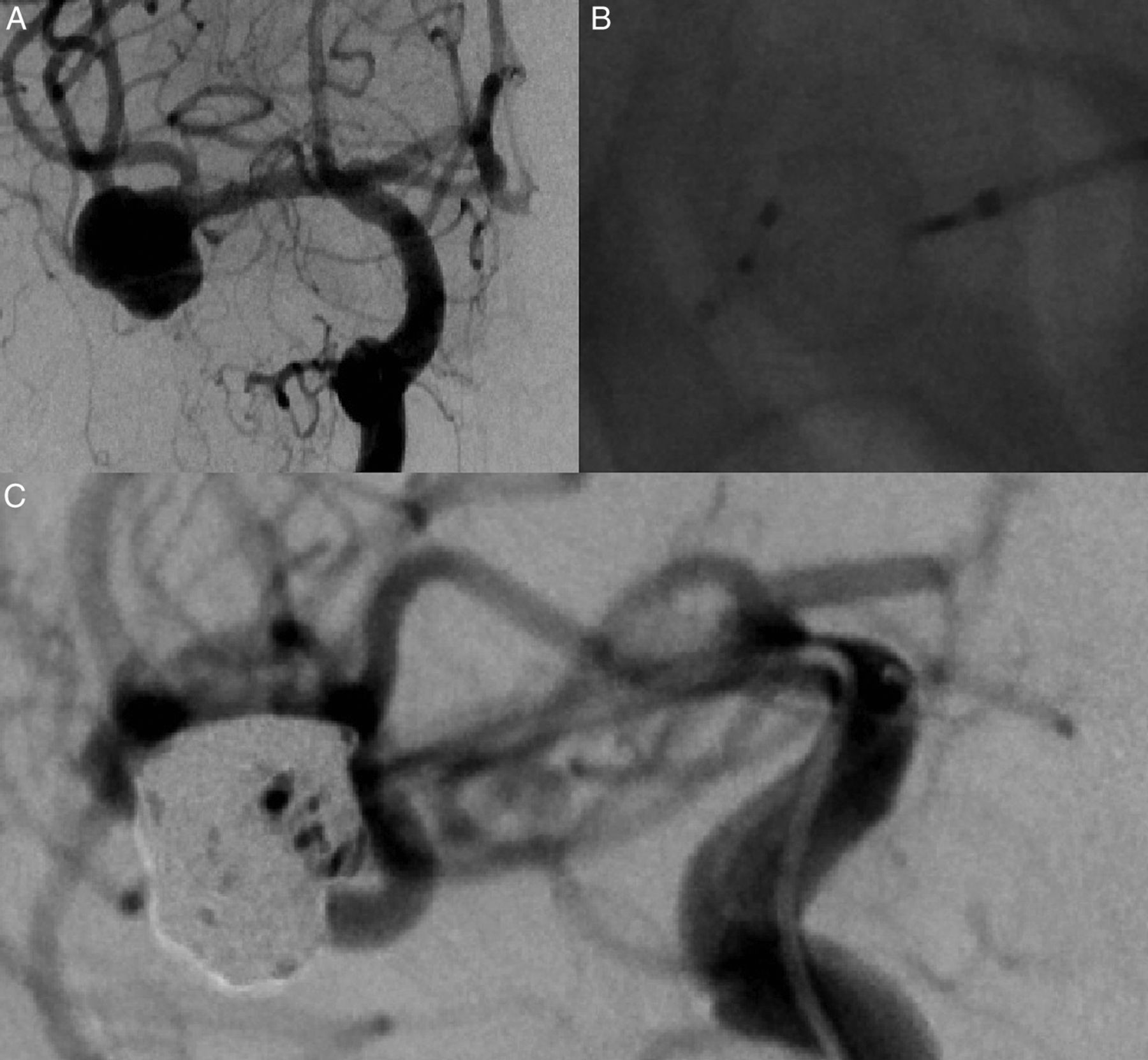
A 60-year-old man presented to the emergency department of a peripheral hospital with collapse and seizures and a Glasgow Coma Score of 14/15. The patient's pre-procedure mobility was impaired, using a zimmer frame, with right leg and left arm weakness presumed to be due to spondylitis. An unenhanced CT scan revealed Fisher grade 4 subarachnoid hemorrhage. CT angiography confirmed the presence of a solitary large wide-necked left middle cerebral artery (MCA) aneurysm. A conjoint decision was made by the neurovascular team for endovascular treatment, which was performed 4 days after presentation. Conventional angiography confirmed the same and also vasospasm (figure 1A, B). Balloon-assisted coiling was not attempted due to the wide neck measuring 9 mm. The aneurysm was embolized with a 11 mm×8 mm WEB SL device and eight coils ranging in size from 15 mm×50 cm to 6 mm×20 cm (figure 1C, D) after administration of intra-arterial nimodipine for vasospasm. The procedure was completed without any complication. The WEB device was positioned reconstructing the MCA bifurcation with no encroachment of the vessel lumen of either of the MCA branches.

(A) Three-dimensional digital subtraction angiogram (DSA) showing the wide-necked left middle cerebral artery (MCA) aneurysm. (B) DSA showing vasospasm; compare the caliber of the M1 segment of the MCA with the MCA branches, showing spasm in the M1 segment. (C) Coiling microcatheter jailed in the aneurysm with the WEB device delivered into the aneurysm. (D) Post-coiling angiographic run showing the WEB device and coils in the aneurysm, together securing the aneurysm.
The patient remained confused after the procedure and deteriorated 24 h after the procedure with reducing verbal output. This was presumed to be due to vasospam and was treated medically with no further intra-arterial therapy. The patient had to be re-intubated within 48 h of the procedure for sepsis. Upon extubation the patient had worsened right-sided weakness with an unenhanced CT scan showing ischemic changes in the left MCA territory. The patient was discharged to a rehabilitation unit and was able to mobilize with the assistance of one person at the time of discharge from hospital and with a walking aid post-rehabilitation.
Case 2
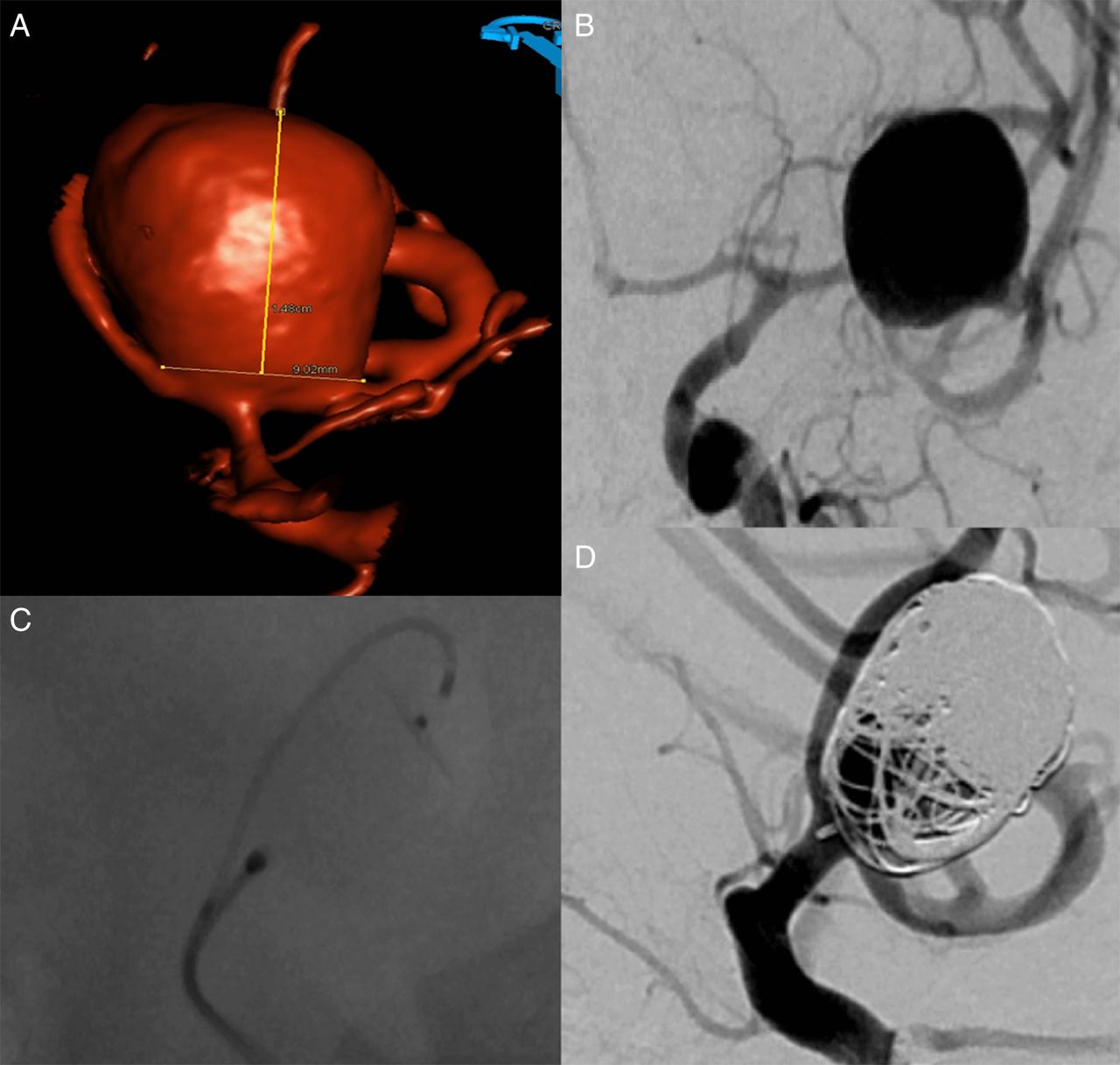
A 64-year-old woman was found to have an incidental right MCA aneurysm (figure 2A). The patient decided to undergo endovascular treatment given the size of the aneurysm and risk of rupture. Uncomplicated treatment of the aneurysm was completed with a 8 mm×6 mm WEB SL device and six coils ranging in size from 14 mm×40 cm to 4 mm×12 cm (figure 2B, C). The patient was discharged the day after the procedure without any complication.
(A) Digital subtraction angiogram (DSA) showing the large unruptured middle cerebral artery (MCA) aneurysm. (B) Coiling microcatheter jailed in the aneurysm with the WEB device delivered into the aneurysm. (C) WEB device protecting the aneurysm neck, preserving the MCA branches with the rest of the aneurysm coiled off.
Treatment
This technique requires bifemoral access with two guide catheters in the parent vessel. This was achieved with an Envoy 5 Fr MPD (Codman & Shurtleff, Massachusetts, USA) and a Navien intracranial support catheter (ev3/Covidien, Irvine, California, USA) in both cases. Support for the Navien catheter was provided with a Neuron MAX catheter (Penumbra, California, USA). The Envoy was used to deliver the coiling microcatheter while the WEB device was then delivered using Via series microcatheters (Sequent Medical, California, USA) through the Navien. The coiling microcatheter was first jailed in the aneurysm followed by the Via microcatheter. The WEB device was then delivered (figure 1C in case 1 and figure 2B case 2). The WEB was corked against the aneurysm neck, concurrently coiling off any residual space in the aneurysm. Post-procedure angiographic runs showed stasis in the WEB device and the dome of the aneurysm was excluded from circulation, securing the aneurysm (figure 1D in case 1 and figure 2C in case 2).
The option of a single large sheath to accommodate both guide catheters could be considered instead of bilateral femoral artery punctures, but bilateral punctures may be preferable as femoral access could be closed with standard 6 Fr and 8 Fr arterial access closure devices.
Outcome and follow-up
Given Fisher grade 4 subarachnoid hemorrhage and delayed deterioration, vasospasm was presumed to be the cause of neurological deterioration in case 1, perhaps also worsened by sepsis. It is not our routine institutional practice to offer additional intra-arterial therapy for vasospam, so medical therapy for vasospasm was continued. Post-procedure thromboembolism as a cause for the neurological deterioration was deemed unlikely, given no vascular compromise of the MCA branches by either the WEB device or coils and substantial institutional experience with the WEB device.
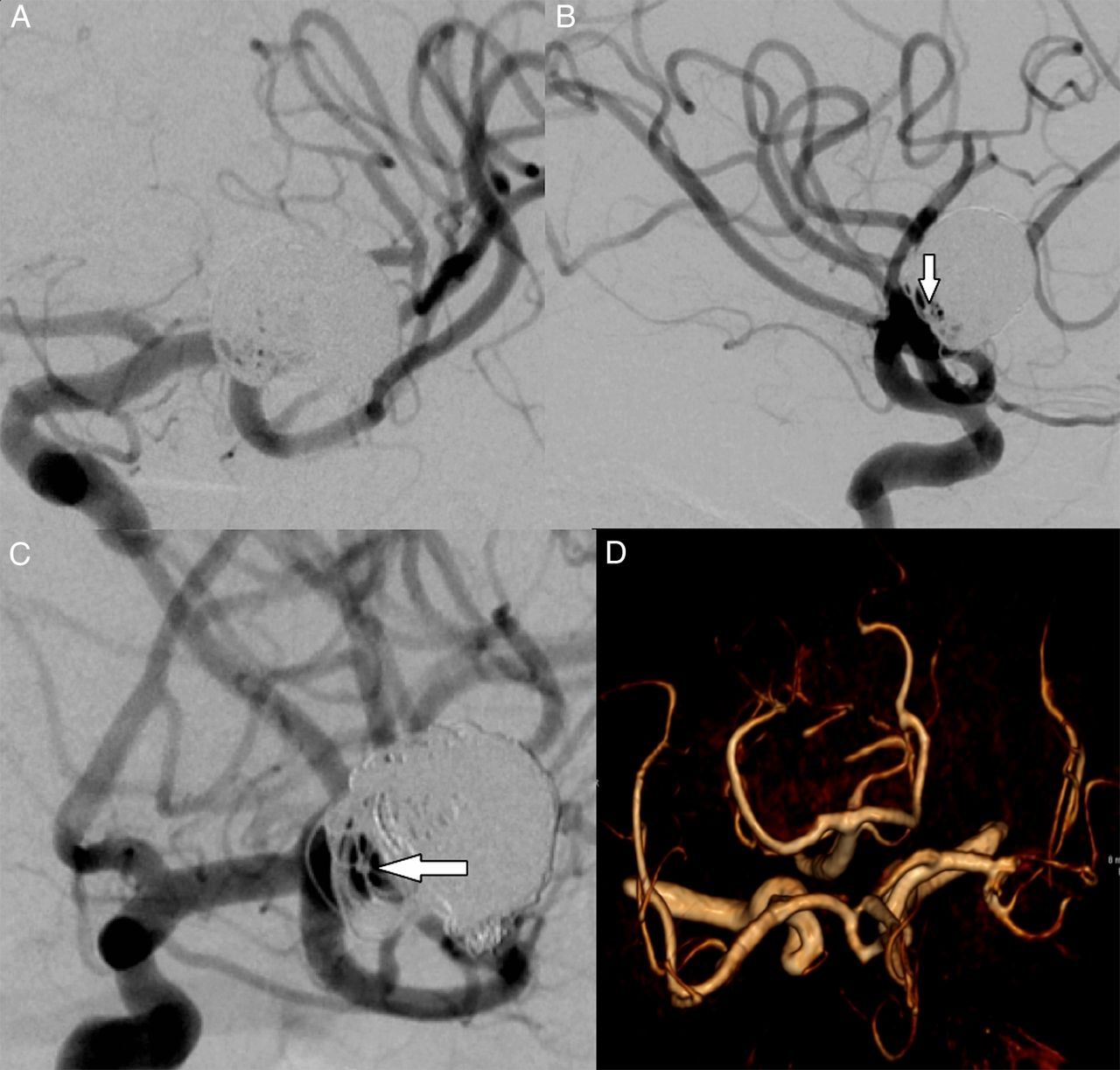
The patient underwent 6-month follow-up MR angiography (MRA) and digital subtraction angiography (DSA) which showed no aneurysm residuum or recurrence. The MCA branches were well preserved with no encroachment of the vessel lumen by the WEB device to support post-procedure MCA branch thrombosis as the cause for neurological deterioration (figure 3A–D).
{kind=link}
{kind=link}
{kind=link}
(A–C) Six-month follow-up digital subtraction (DSA) showing no aneurysm residuum or recurrence and the middle cerebral artery (MCA) branches well preserved. The proximal marker of the WEB device is highlighted (arrow) in (B) and (C). Contrast adjacent to the proximal marker is filling the proximal recess of the WEB device. (D) Six-month follow-up time-of-flight MR angiogram showing the treated aneurysm neck with no MCA branch loss.
Case 2 is to have a follow-up MRA and DSA at 6 months post-procedure as per local departmental protocol.
Discussion
This novel technique of coiling off any residual space left by the WEB device through a jailed microcatheter helps to treat wide-necked large aneurysms. The WEB device is corked at the aneurysm neck with controlled delivery and further manipulation if required. This allows the dome and any further residual space in the aneurysm to be coiled through the jailed microcatheter and is ideally done as a two-person maneuver. A microcatheter with a relatively flexible tip is recommended for this purpose. The WEB device can be detached upon satisfactory coiling of the residual space and the coiling microcatheter retrieved then. No difficulty was encountered in withdrawing the coiling microcatheter in either of our cases.
It is vital to have excellent control during delivery and manipulation of the WEB device and a triaxial system with a distal access with an intermediate catheter is therefore of much benefit. It is also of utmost importance that the operator should have considerable experience with the WEB device before attempting to treat aneurysms with WAC, given the complexity of the procedure. Further studies are needed before this technique can be widely recommended.
Footnotes
Republished with permission from BMJ Case Reports Published 2 May 2015; doi:10.1136/bcr-2015-011649.
Competing interests SL does proctoring for WEB cases.
Patient consent Obtained.
Ethics approval Research and Development, University Hospitals Birmingham.
Provenance and peer review Not commissioned; externally peer reviewed.