Article Text

Abstract
Background Bioactive coils were introduced in 2002 in an attempt to improve aneurysm healing and durability of angiographic results. Evidence demonstrating superior efficacy to justify the routine use of bioactive coils over bare coils is limited. We compared the periprocedural and clinical outcome after bioactive and bare platinum coiling for intracranial aneurysms.
Methods MEDLINE, EMBASE, Cochrane Library, and ISI Web of Knowledge Conference Proceedings Citation Index—Science were searched for randomized clinical trials (RCTs) comparing bioactive and bare coils. The methodological quality was evaluated to assess bias risk. Periprocedural outcomes and mid-term outcomes were compared.
Results Five independent RCTs comparing bioactive (n=1084) and bare coils (n=1084) were identified. Periprocedural outcome was similar for both groups. Bioactive coiling increased the rate of complete aneurysm occlusion (47% vs 40%; RR 1.17 (95% CI 1.05 to 1.31); p=0.006) and reduced the rate of residual aneurysm neck at 10 months compared with bare coiling in the mid-term (26% vs 31%; RR 0.82 (95% CI 0.70 to 0.96); p=0.01). There were no differences in aneurysm recurrence, aneurysm rupture, stroke, neurological death, modified Rankin Scale score and reinterventions. Subgroup analysis for the three RCTs on hydrogel coils demonstrated reduction of residual aneurysms compared with bare coiling (25% vs 34%; RR 0.76 (95% CI 0.58 to 0.99); p=0.04).
Conclusions Bioactive coils ensure a higher rate of medium-term complete aneurysm occlusion while reducing the rate of residual neck aneurysms compared with bare coiling in the mid-term. Hydrogel coils reduce residual aneurysms compared with bare coils. While there is level 1a evidence to show more complete aneurysm occlusion, longer term follow-up is needed to determine if this translates into clinical significance.
- Aneurysm
- Bioactive
- Coil
Statistics from Altmetric.com
Introduction
Neurosurgical clipping has long been the only treatment for intracranial aneurysms. Since the early 1990s, Gugliemli detachable coiling has provided a minimally invasive alternative for clipping of ruptured and unruptured intracranial aneurysms.1 The International Subarachnoid Aneurysm Trial has demonstrated improved clinical outcome compared with clipping and has provided level 1 evidence for endovascular coiling as the treatment of choice for ruptured aneurysms.2–5 Traditionally, bare platinum coils are used, but these coils are associated with angiographic recurrence in up to 18% of cases,6 although only about one-third of recurrences need reintervention. Therefore, bioactive coils were introduced in 2002 in an attempt to improve aneurysm healing and durability of angiographic results. These coils consist of a platinum core that has been enhanced with bioactive components such as polyglycolic acid (Cerecyte coil), polyglycolic acid/lactide (Matrix2 coil) and hydrogel (HydroCoil).
However, previous studies have failed to demonstrate a consensus regarding the benefits of bioactive coils over bare coils. Bioactive coils are more costly, yet it remains to be demonstrated whether there are any benefits to justify their routine use. A review of cohort studies on various bioactive coils published up to 2007 lacked a comparison with bare coils.7 This paper concluded that there has been a hype around the introduction of bioactive coils,8 with very little evidence for any improvement in angiographic outcomes.7 It was therefore recommended that bioactive coils should be used sparingly outside randomized controlled trials (RCTs).7 Another review based on publications up to 2011 chose angiographic recurrence as the only comparator and did not identify statistical differences between bioactive and bare coils either.9 Since the date of the literature search of these reviews, a single RCT was published in 2012,10 followed by another three RCTs last year.11–13
The results of these individual RCTs do not show significant differences and have not provided a definitive answer. One of the RCTs concluded that “these studies provide the potential to carry out high-quality systematic reviews, which along with other randomized evidence already published, will provide reliable and valuable information”.10 The proposed systematic review which combines all level 1 evidence has not yet been published. The present study aimed to review and perform meta-analyses of all RCTs comparing bioactive with bare coiling for intracranial aneurysms, and to generate the highest level of evidence to determine which coil should be regarded as the endovascular therapy of choice.
Materials and methods
Study selection
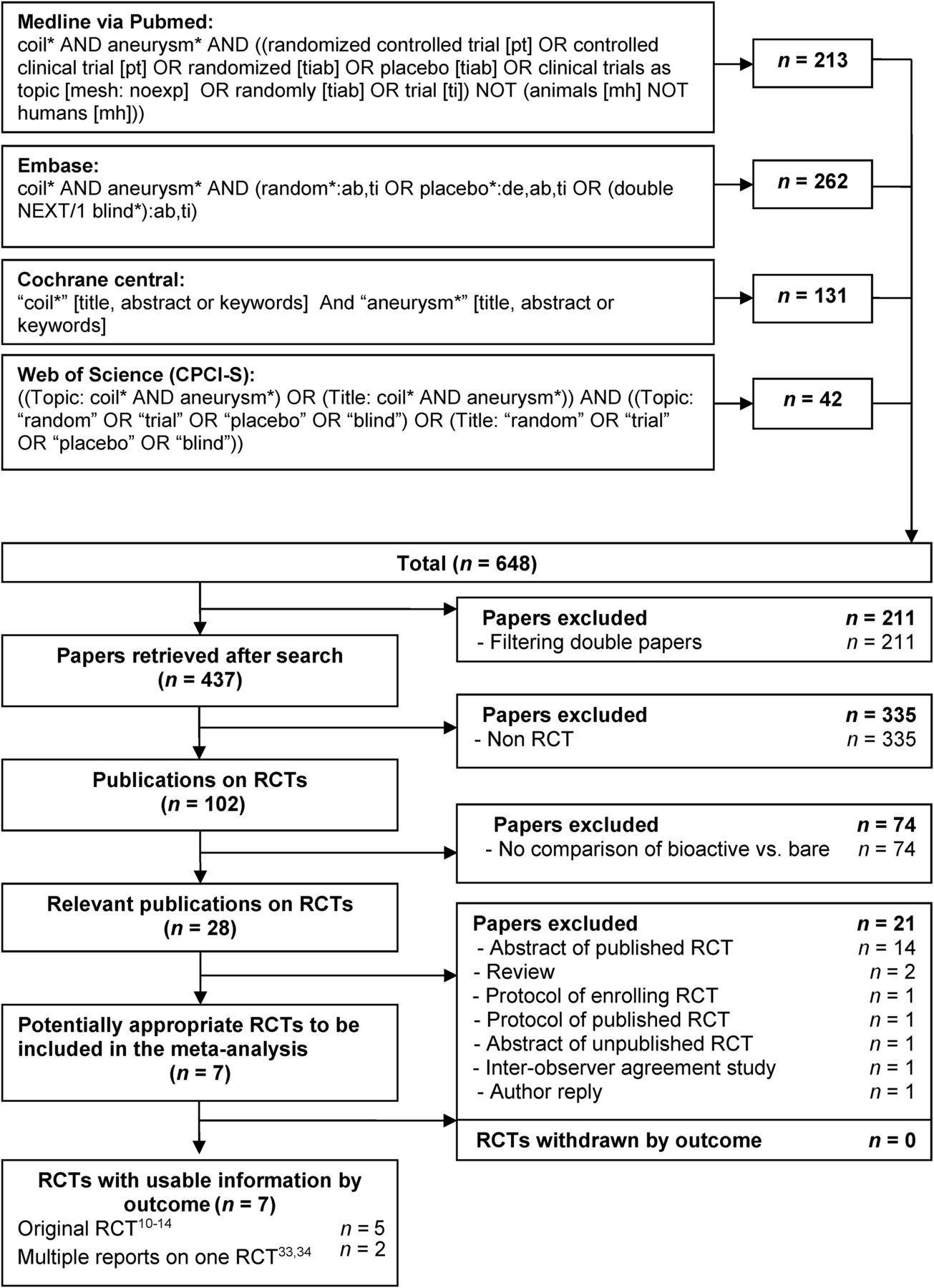
A systematic literature search with predefined search terms was carried out in MEDLINE (from 1960), EMBASE (from 1980), Cochrane Library (issue 1, 2012) and the ISI Web of Knowledge Conference Proceedings Citation Index—Science (CPCI-S; from 1990) databases on 13 December 2014 (figure 1). All identified articles were screened for cross-references. Language restrictions were not applied.

Flowchart illustrating the details of the search strategy and study selection process according to the Quality of Reporting of Meta-analyses (QUOROM) statement.16–18 RCT, randomized clinical trial; MesH, Medical Subject Heading; CPCI-S, Conference Proceedings Citation Index—Science.
Inclusion criteria
The title and abstract of all identified articles were screened and selected according to the following inclusion criteria: study population (adult patients with ruptured or unruptured cerebral aneurysms undergoing endovascular coiling); intervention (clearly documented endovascular treatment with bioactive or bare platinum coils); study outcomes (at least one of the outcome measures reported below); study design (patients assigned to either bioactive or bare platinum coils by random allocation); publication (published as a full article in a peer-reviewed journal).
Exclusion criteria
Studies were excluded from analysis if they did not meet the inclusion criteria, or if the corresponding author was not able to provide data requested and it was impossible to extract or calculate appropriate data from the published results. Abstracts of RCTs were excluded as the endovascular technique, methodological quality, and the risk of bias of these studies could not be assessed.
Outcomes of interest and definitions
Periprocedural outcomes measured were: failed procedures, perforation, aneurysm rupture, thromboembolic complications, hydrocephalus, complication rate, morbidity, modified Raymond Scale,14 adverse (deterioration vs baseline or dependence (mRS >2)) modified Rankin Scale (mRS; 0, no symptoms; 1, no significant disability; 2, slight disability; 3, moderate disability; 4, moderately severe disability; 5, severe disability; 6, dead), and mean and adverse (World Federation of Neurosurgical Societies (WFNS) >2) WFNS grade (1, Glasgow Coma Scale (GCS) 15; 2, GCS 13–14; 3, GCS 13–14 focal neural deficit; 4, GCS 7–12; 5, GCS <7; 6, death),15 and inability to be discharged home.
Mid-term outcomes included: modified Raymond Scale, aneurysm recurrence since procedure, aneurysm rupture or re-rupture since procedure, ischemic stroke, hemorrhagic stroke, neurological death, mean and adverse mRS score and reintervention. Subgroup analysis for different coil types was performed if two or more trials could be pooled in meta-analyses.
Data extraction
Titles and abstracts of all retrieved records, and subsequently full-text articles, were examined according to the Quality of Reporting of Meta-analyses (QUOROM) guidelines.16–18 The following data were extracted separately for all studies meeting the inclusion criteria: reference of study, study population characteristics, study design, inclusion and exclusion criteria, and number of participating subjects for each endpoint. For dichotomous outcomes, the number of events was recorded and for continuous outcomes means and SDs were registered.
Authors of all the original RCTs were contacted and all but one agreed to provide missing data. The senior author of the latter trial could not contribute due to time constraints and consequently only published data were used for meta-analysis.11
Risk of bias assessment
Risk of bias was assessed for all articles using both the Cochrane Collaboration's tool for assessing risk of bias19 and the Jadad scoring system.20
Statistical analysis
Statistical analyses were performed following the recommendations of the Cochrane Collaboration and QUOROM guidelines.16–18 Outcomes reported by two or more studies were pooled in meta-analyses. Dichotomous and continuous outcomes were presented as risk ratios (RRs) and weighted mean differences (WMDs), respectively. Data were pooled using the Mantel–Haenszel method for dichotomous outcomes and the inverse variance method for continuous outcomes. Trials with zero events in both arms were excluded from meta-analysis. Trials with zero events in one arm were included in the analysis by adding a continuity correction of 0.5 to all cells in the 2×2 table of that study. As a robustness assessment, meta-analyses with RCTs with zero events in one arm were also performed using risk differences in a sensitivity analysis. For all analyses the 95% CI was calculated.
Heterogeneity was calculated using the Higgins χ2 test21 and inconsistency in study effects was quantified by I2 values.19 ,22 The fixed-effects model was used if no heterogeneity was present (χ2 p value >0.1 and I2 <50%). If excessive heterogeneity was present, data were first rechecked and the DerSimonian random-effects model was used when heterogeneity persisted.23 Funnel plots were used to help identify the presence of publication or other types of bias.24–26 Review Manager software (RevMan V.5.0.16) provided by the Cochrane Collaboration was used for data management and statistical analyses.
Results
Description of studies
A total of 836 potential relevant publications were identified (figure 1). One hundred and two papers on RCTs were identified, of which 28 compared bioactive and bare coils. Two reviews were identified.7 ,9 One potentially relevant RCT that had been published as an abstract only without a peer-reviewed publication was excluded.27 Another abstract is currently enrolling patients and was also excluded.28 Finally, seven publications from five original RCTs comparing bioactive and bare platinum coils were identified. The bioactive component was polyglycolic acid/lactide in one trial,11 polyglycolic acid in another trial,10 and hydrogel in the remaining three RCTs.12–14
The five included trials were published between May 2011 and November 2014. A total of 2168 endovascular coiling procedures (bioactive, n=1084; bare, n=1084) were performed. Mean follow-up was 10 months (range 1–18 months; table 1). Age, sex, number of patients who presented with a ruptured aneurysm, and use of an assist device were divided equally between both arms (table 2).
Details of included RCTs comparing bioactive versus bare coils
Patient characteristics
Methodological quality of included studies
The trials had good methodological quality with a mean Jadad score of 4 (range 3–5; table 3). All but one trial12 reported a sample size calculation, prospective registration in a clinical trial registry, allocation concealment, and blinded observers. Three trials10–12 did not blind patients and one trial did not report the method of sequence generation.11 All trials had an adequate report on loss to follow-up and were free of other sources of bias.
Risk of bias summary
Periprocedural outcome
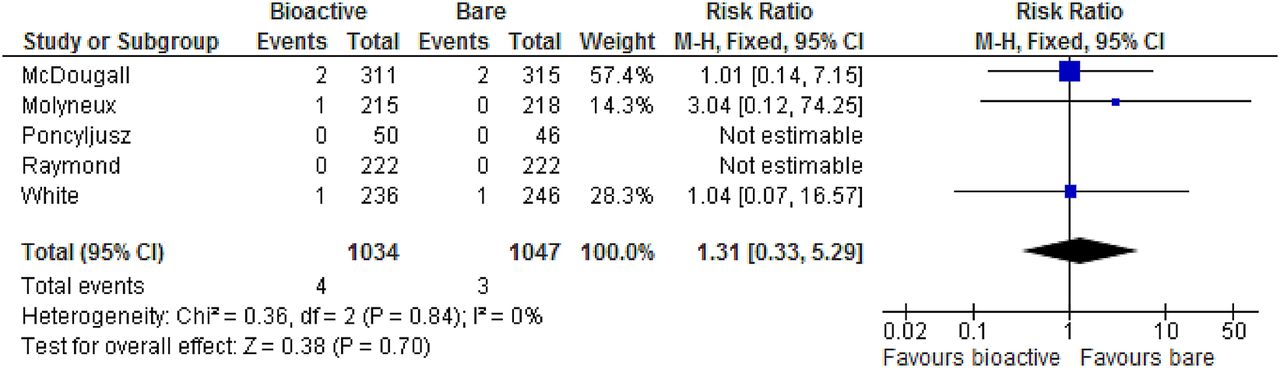
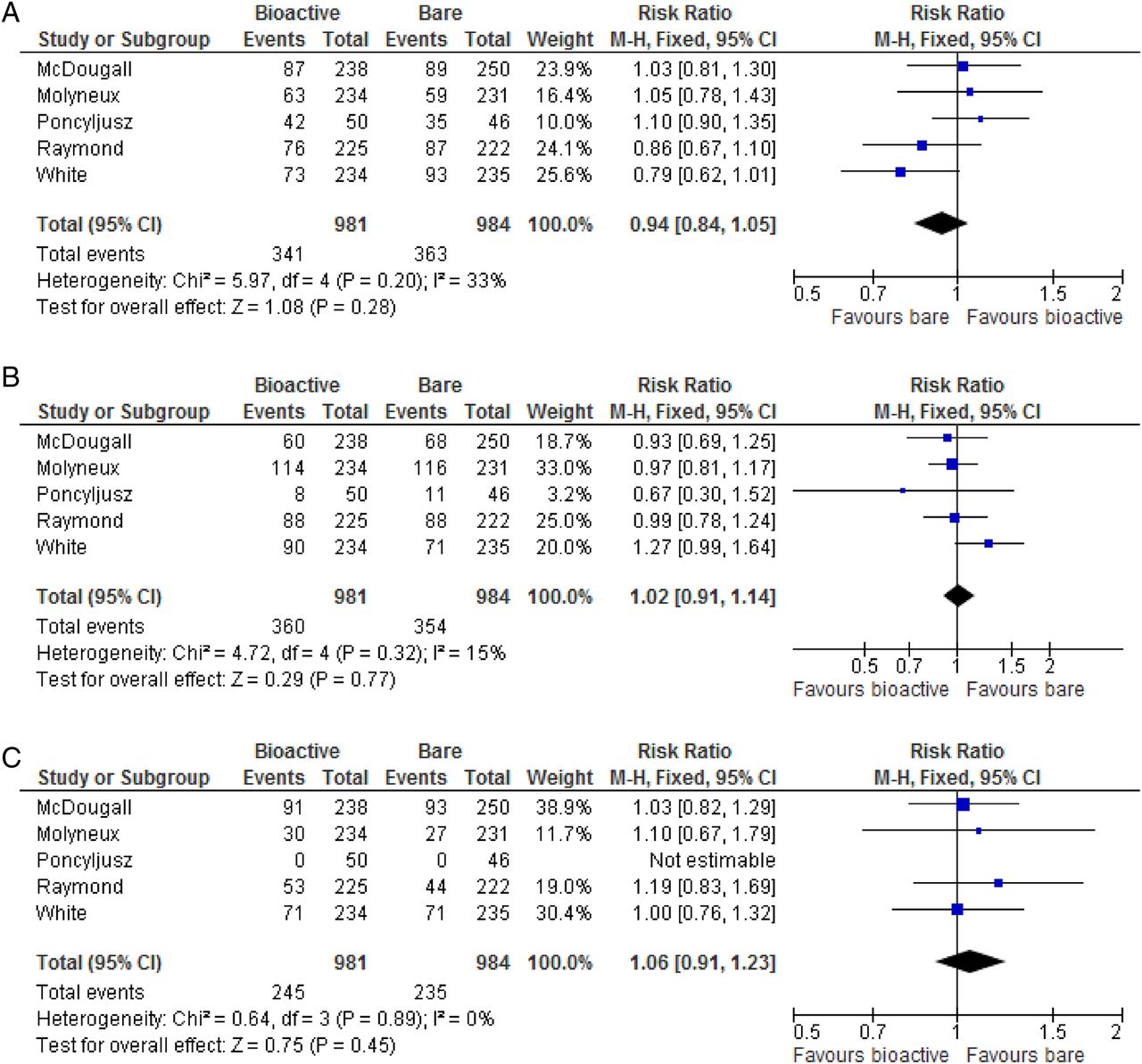
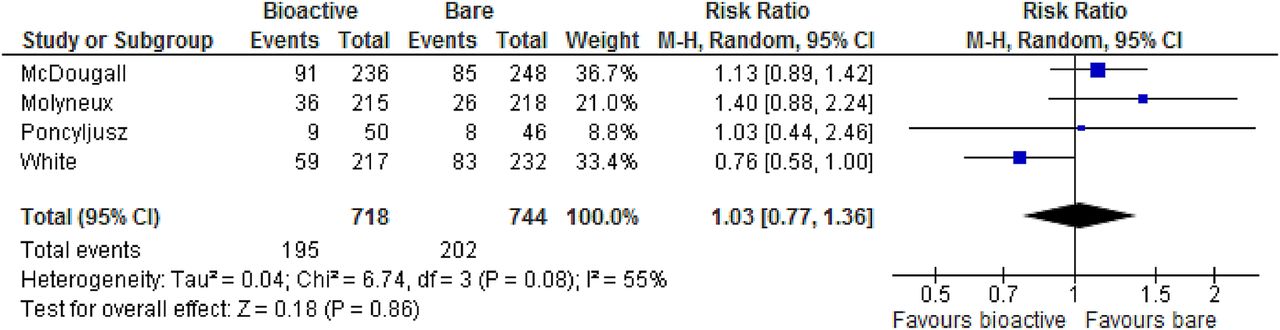
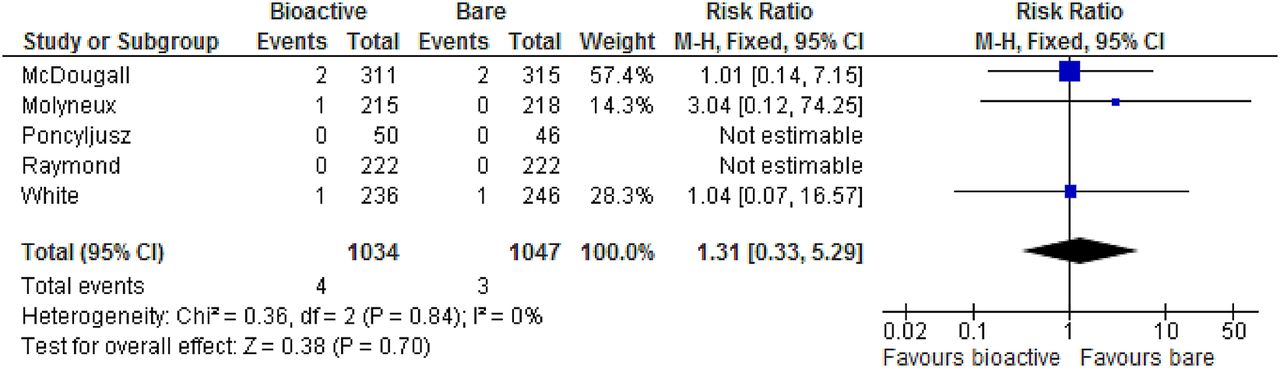
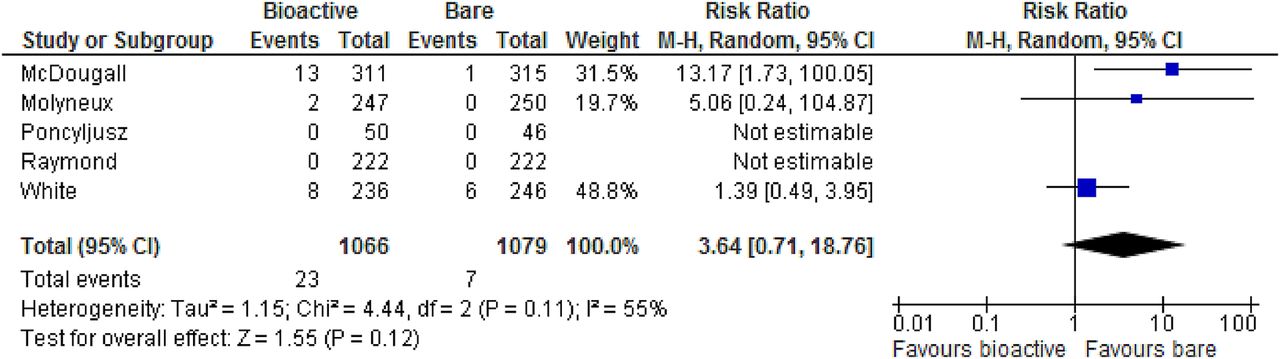
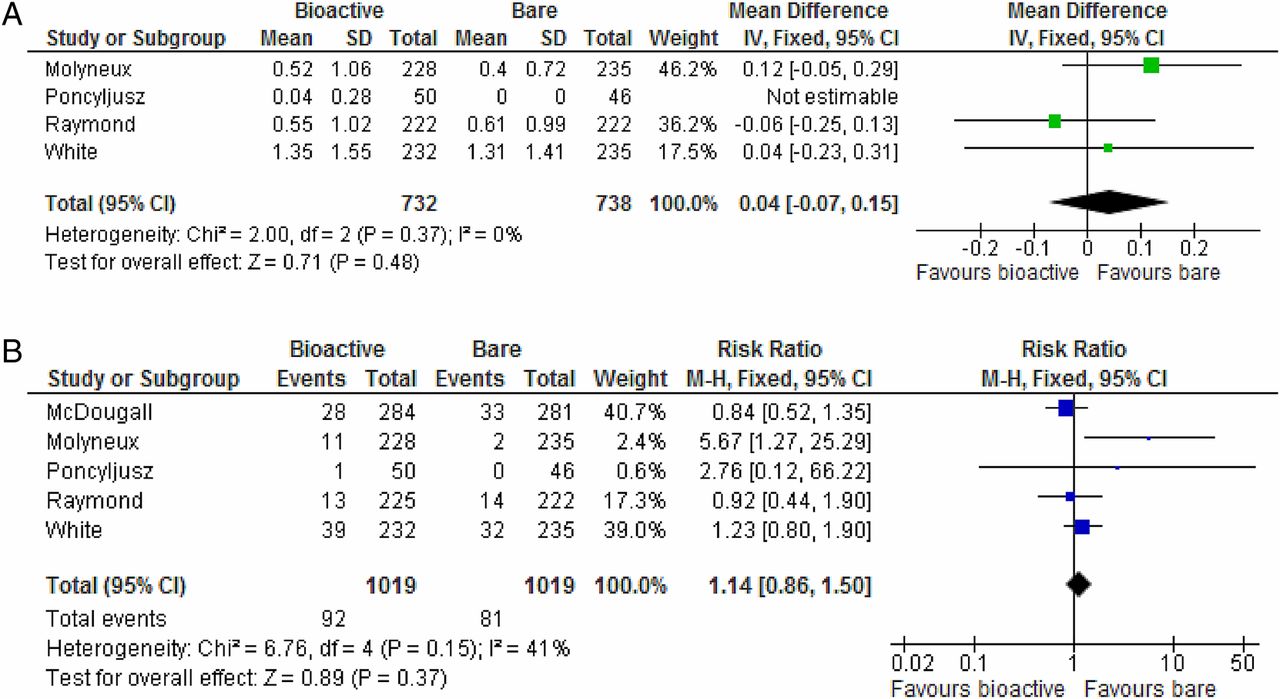
All outcome measures were reported by three or more trials. The number of failed procedures (figure 2), perforation (figure 3), aneurysm ruptures (figure 4), thromboembolic complications (figure 5), hydrocephalus (figure 6), complication rate (figure 7), morbidity (figure 8), and modified Raymond Scale (figure 9) were similar for both groups. Funnel plots did not demonstrate evidence of publication bias (figure 10). The adverse mRS score (figure 11), WFNS grade (figure 12), and ability to be discharged home (figure 13) were also similar for the two groups. Subgroup analysis of three RCTs on hydrogel coils also found that periprocedural outcomes were similar to bare coils.

Forest plot showing failures (periprocedural).

Forest plot showing perforation (periprocedural).

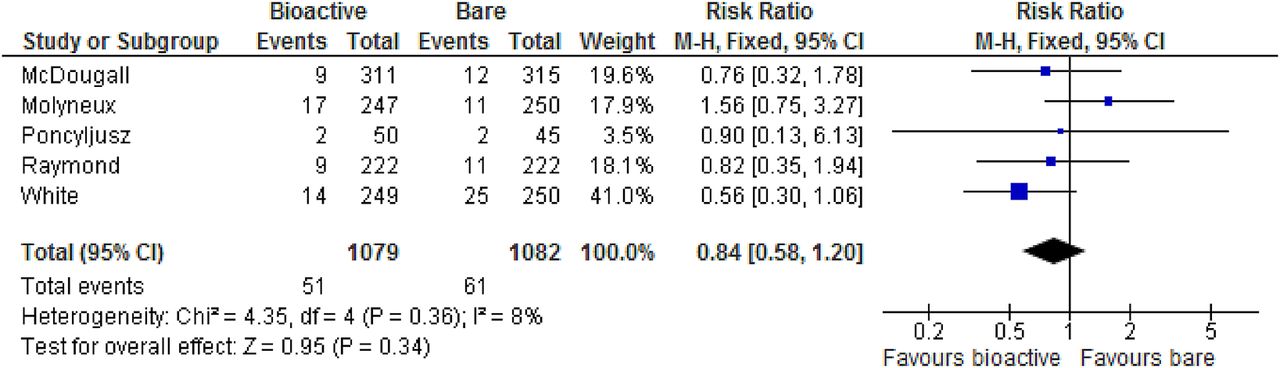
Forest plot showing aneurysm rupture (periprocedural).
Forest plot showing thromboembolic complications (periprocedural).

Forest plot showing hydrocephalus (periprocedural).

Forest plot showing complications (periprocedural).
Forest plot showing morbidity (periprocedural).

Forest plots showing (A) Raymond Scale grade 1: complete aneurysm occlusion (periprocedural); (B) Raymond Scale grade 2: residual aneurysm neck (periprocedural); (C) Raymond Scale grade 3: residual aneurysm (periprocedural).
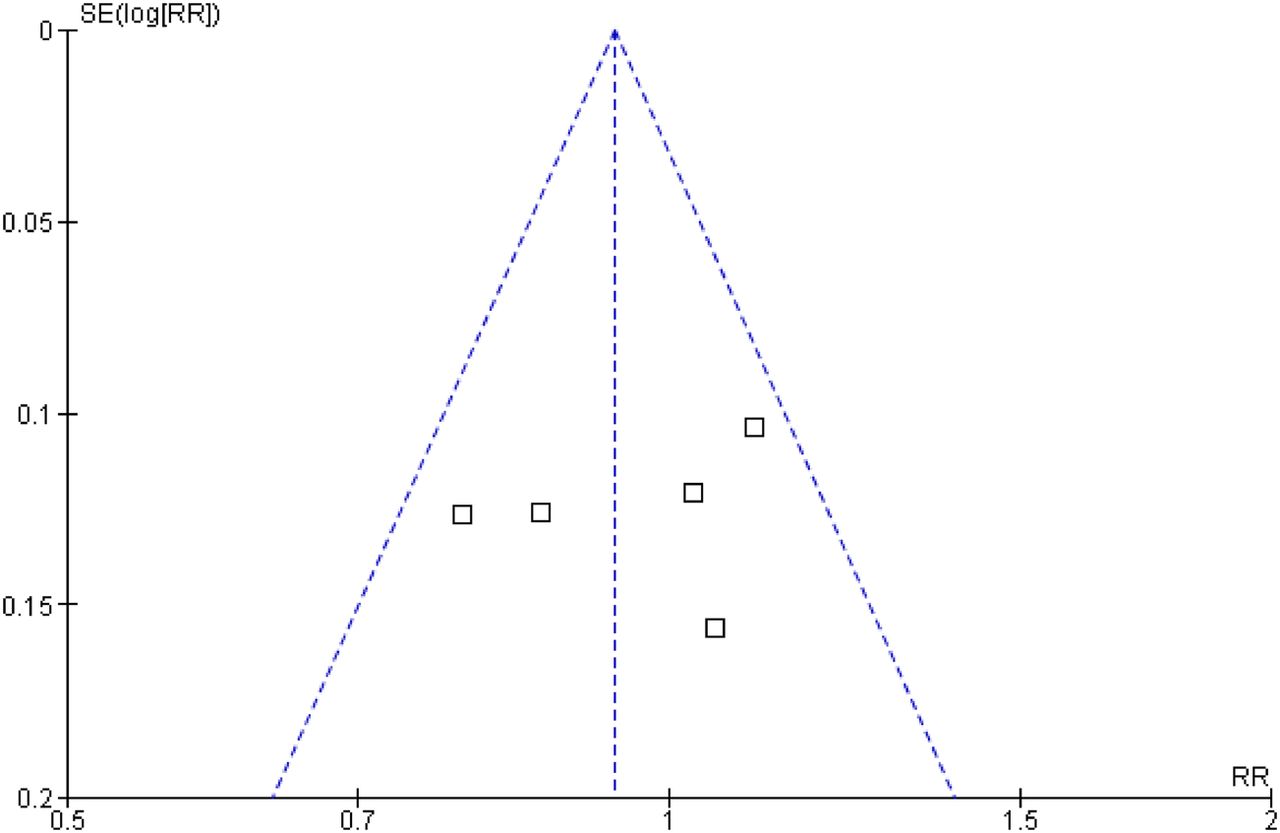
Funnel plot of Raymond Scale grade 1: complete aneurysm occlusion (periprocedural).

Forest plot showing adverse modified Rankin Scale score (periprocedural).

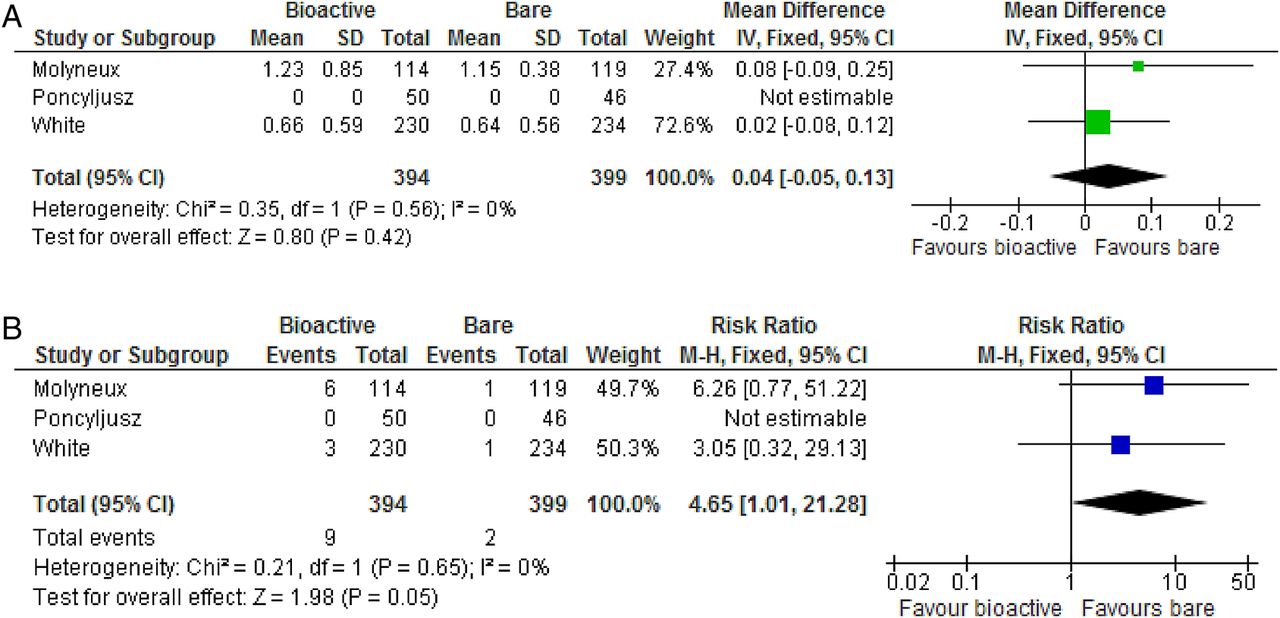
Forest plots showing (A) mean World Federation of Neurosurgical Societies (WFNS) grade and (B) adverse WFNS grade (periprocedural).

Forest plot showing inability to be discharged home (periprocedural).
Mid-term outcome
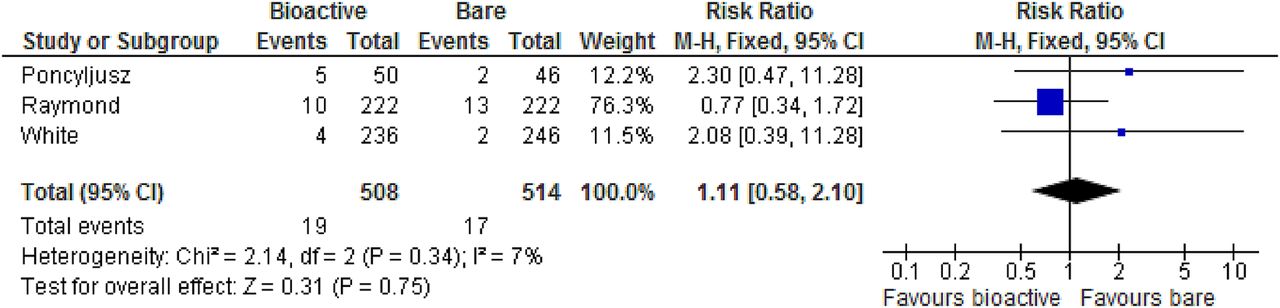
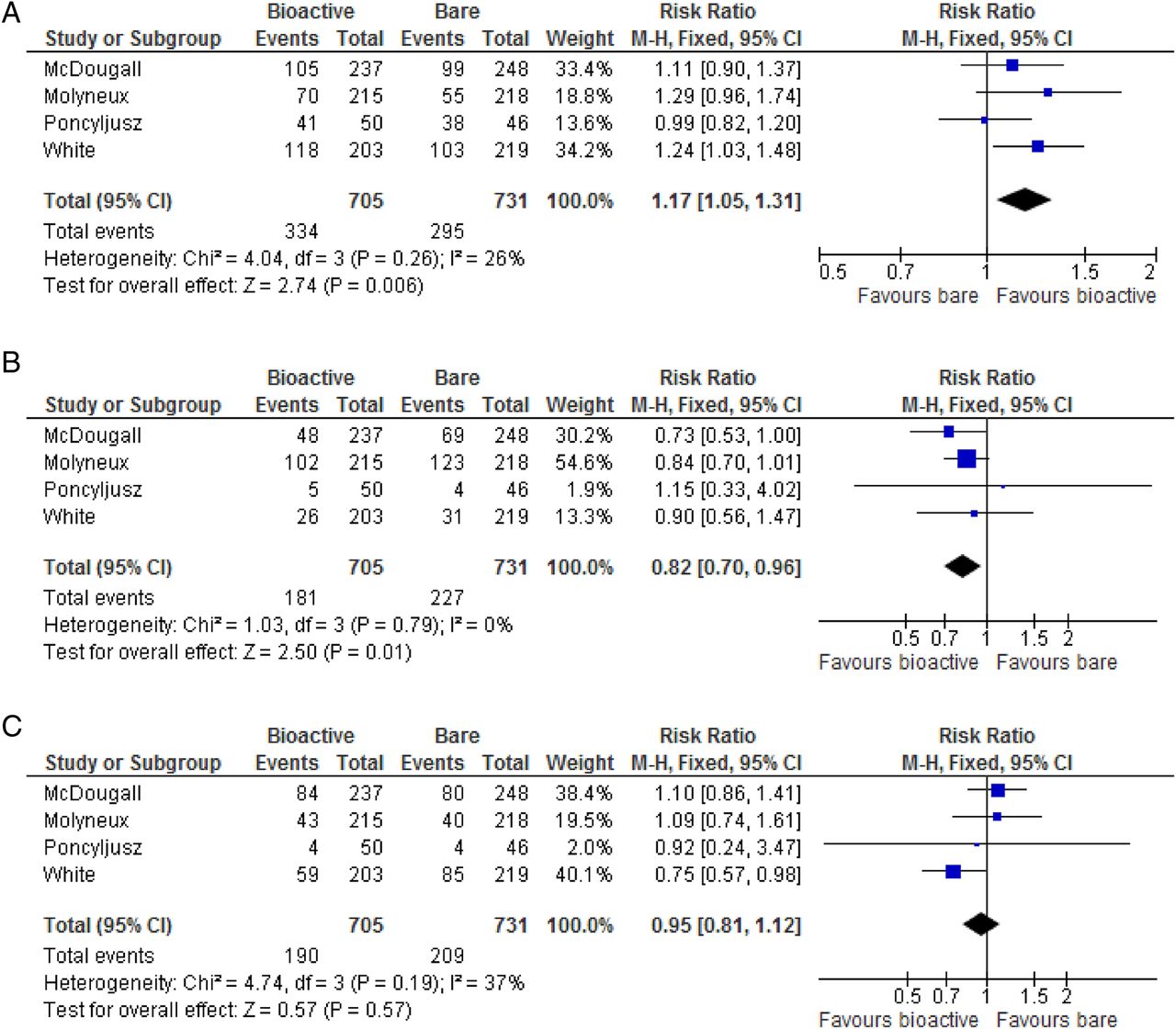
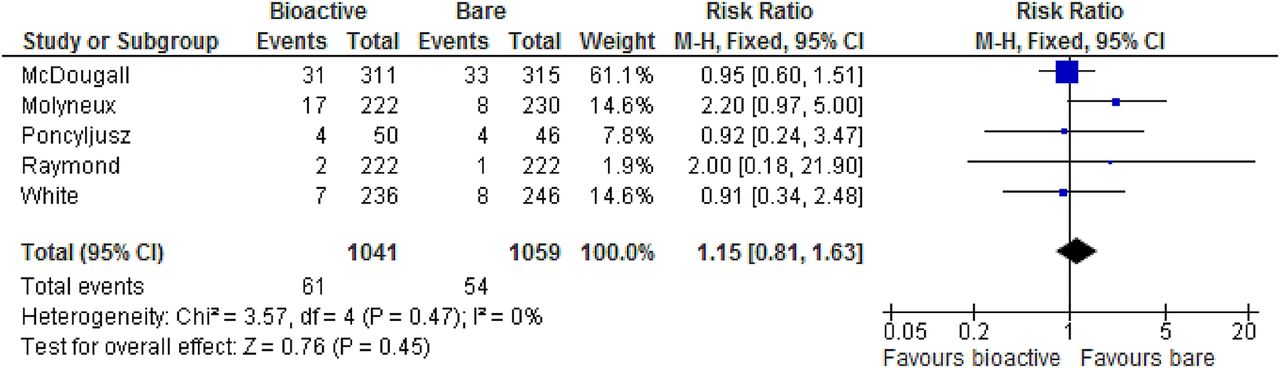
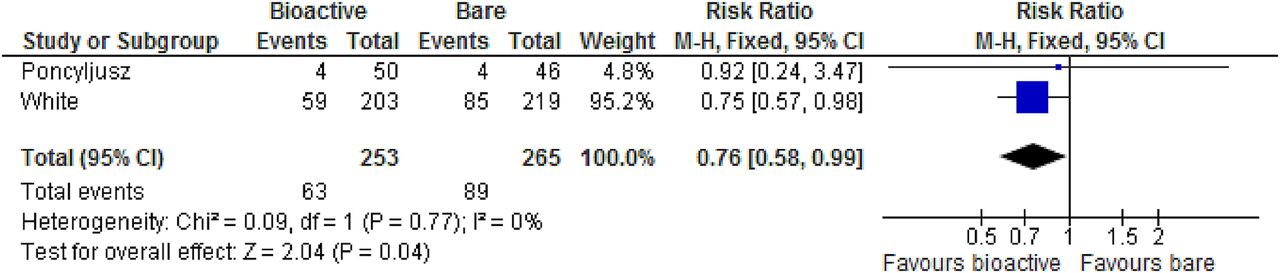
All outcome measures were reported by three or more trials. Bioactive coiling was associated with superior angiographic results on the modified Raymond Scale. The number of patients with complete aneurysm occlusion was higher after bioactive coiling than after bare coiling (47% vs 40%; RR 1.17 (95% CI 1.05 to 1.31); p=0.006; figure 14A). This was accompanied by a reduction in the rate of residual aneurysm neck after bioactive coiling compared with bare coiling (26% vs 31%; RR 0.82 (95% CI 0.70 to 0.96); p=0.01; figure 14B). There was no difference in residual aneurysm (figure 14C), aneurysm recurrence since procedure (figure 15), aneurysm rupture or re-rupture since procedure (figure 16), stroke (figure 17), neurological death (figure 18), mRS score (figure 19), or reinterventions (figure 20). The results of subgroup analysis for the three RCTs on hydrogel coils were in line with the main analysis, demonstrating superior angiographic results on the modified Raymond Scale. Hydrogel coiling reduced the number of patients with residual aneurysms compared with bare coiling (25% vs 34%; RR 0.76 (95% CI 0.58 to 0.99); p=0.04; figure 21). All other mid-term outcome measures were also similar for bare and bioactive coils in the subgroup analysis.

Forest plots showing (A) Raymond Scale grade 1: complete aneurysm occlusion (mid-term); (B) Raymond Scale grade 2: residual aneurysm neck (mid-term); and (C) Raymond Scale grade 3: residual aneurysm (mid-term).
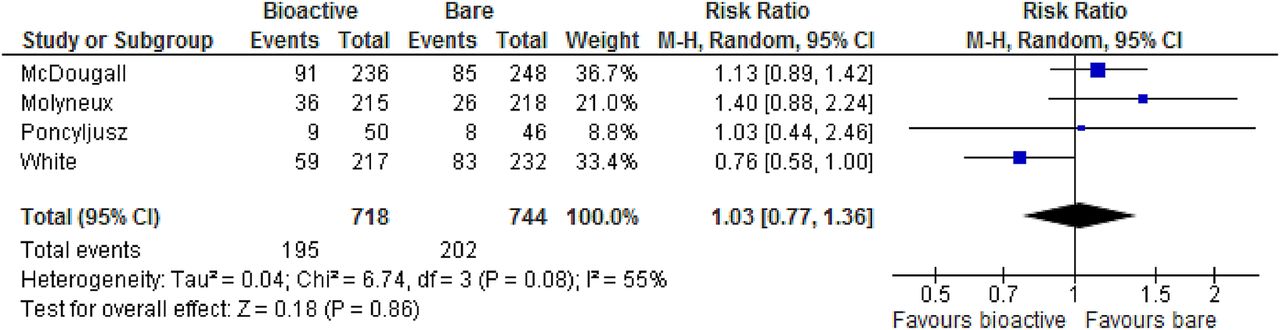
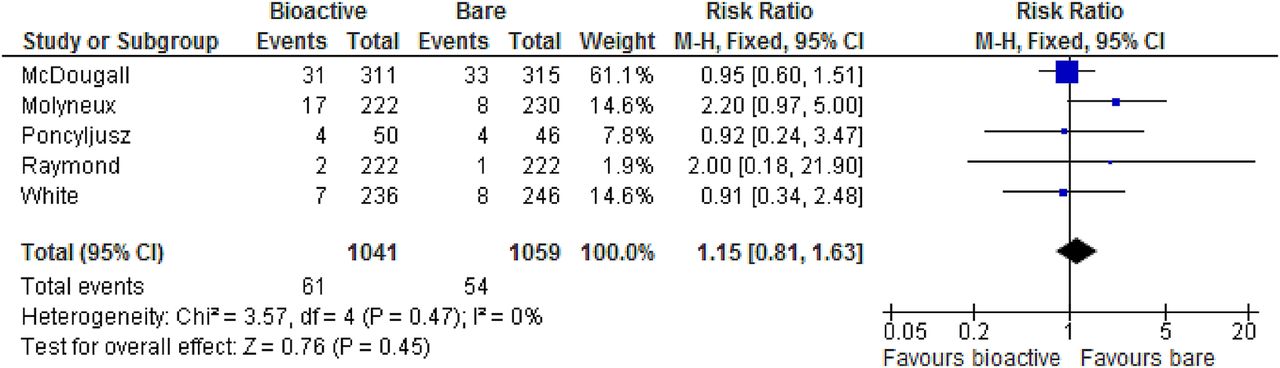
Forest plot showing aneurysm recurrence since procedure (mid-term).
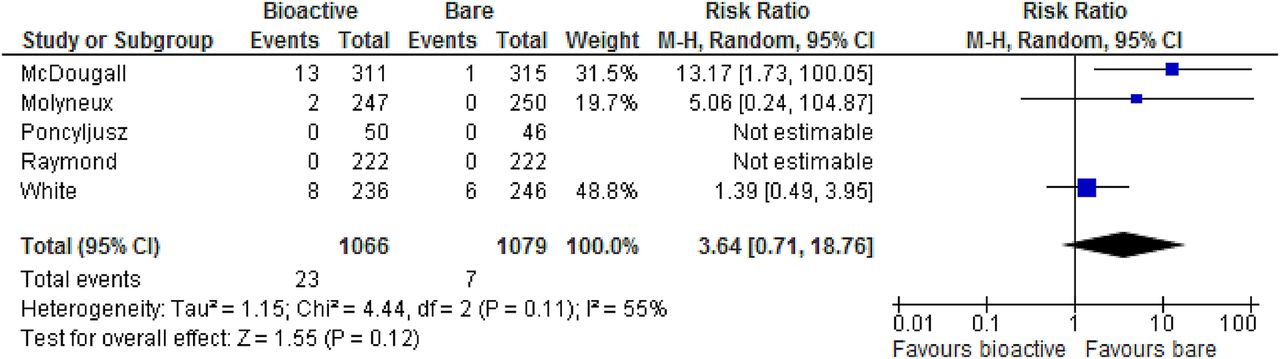
Forest plot showing aneurysm rupture or re-rupture since procedure (mid-term).
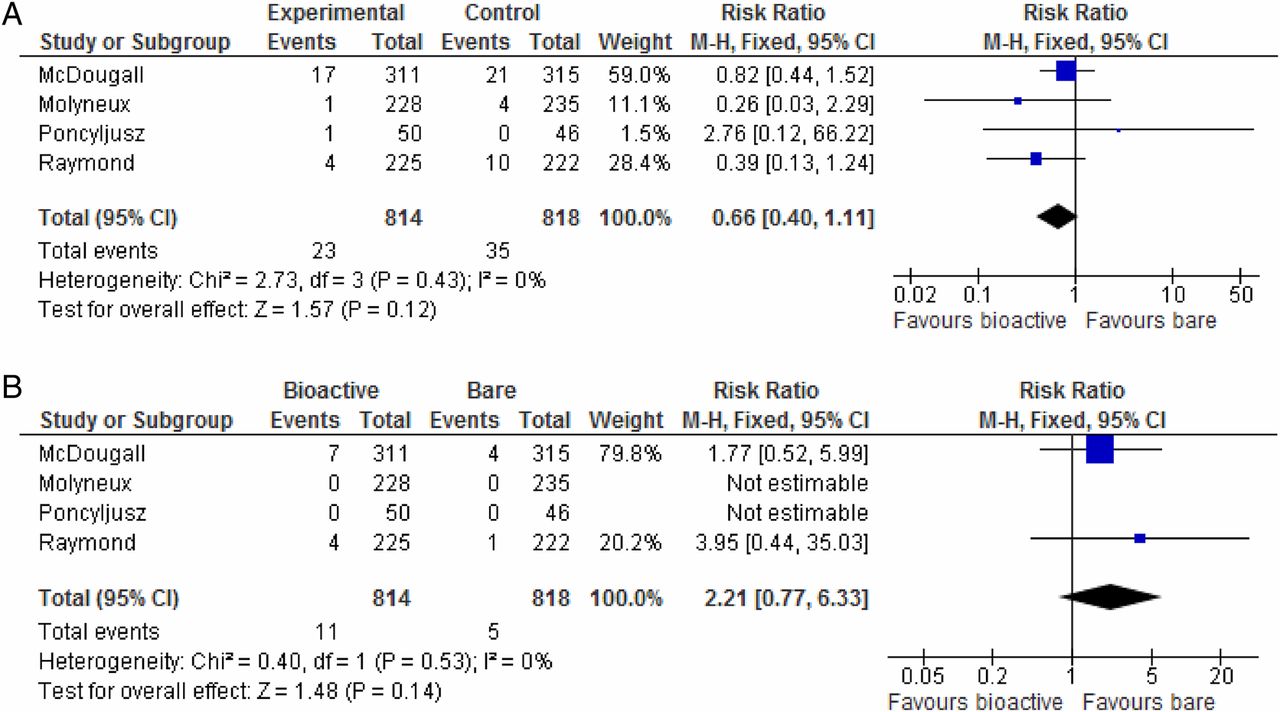
Forest plots showing (A) ischemic stroke (mid-term) and (B) hemorrhagic stroke (mid-term).
Forest plot showing neurological death (mid-term).

Forest plots showing (A) mean modified Rankin Scale (mid-term) and (B) adverse modified Rankin Scale (mid-term).
Forest plot showing reintervention.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing Raymond Scale grade 3: residual aneurysm in hydrogel subgroup (mid-term).
Discussion
Endovascular coiling is the treatment of choice for ruptured intracranial aneurysms2–5 and a minimally invasive alternative for neurosurgical clipping in unruptured aneurysms. The Achilles heel of this minimally invasive technique is angiographic recurrence, with a rate of up to 18% reported by a recent systematic review.6 Bioactive coils were therefore introduced in 2002 in an attempt to improve aneurysm healing and the durability of the angiographic results. Previous studies have varied in their conclusion about the superiority of bioactive coils over bare platinum coils. Two systematic reviews have found that the methodological quality of studies published up to 2011 was poor due low follow-up rates, small sample sizes, and lack of independent assessment and sample size calculations.7 ,9 These factors result in a high risk of bias, and a paucity of randomized studies was noted.7 ,9 Both reviews concluded that there is very little evidence for any improvement in the angiographic outcome and recommended that bioactive coils should be used sparingly outside RCTs.7 ,9 Since the date of the literature search of these reviews, four medium-sized RCTs comparing bioactive with bare coils have been published.10–13 These individual studies have not been able to identify significant differences either.10–13 Bioactive coils have a substantial cost premium and consequently it is still questionable whether there is any improvement in efficacy to justify their routine use. The current review aims to evaluate the potential benefits and disadvantages of bioactive coils by bringing the evidence base up to date.
The shortcomings in methodology identified by the previous reviews have been overcome by the RCTs that have been published subsequently. The methodological quality of the five RCTs included in the current meta-analysis was good, with a mean Jadad score of 4. All but one trial12 reported a sample size calculation, prospective registration in a clinical trial registry, allocation concealment and blinding of observers. Patient populations were comparable among the trials, with all but one trial including both patients with ruptured and unruptured aneurysms. Baseline patient characteristics were similar between the arms of each trial. The use of an assist device aims to reduce recurrence and retreatment rates. Stents are also used to allow coiling of aneurysms that are unable to be coiled because of a wide neck. The use of assist devices and other endovascular techniques was identical, ensuring that coil type was the only difference between the groups. All the trials had adequate reports on loss to follow-up and were free of other sources of bias.
Previous systematic reviews were solely7 or predominantly9 based on non-randomized studies. These reviews found that the bioactive and bare groups were heterogeneous for preprocedural aneurysm size (bioactive 6.3 mm vs bare 8.2 mm)9 and the percentage of ruptured aneurysms (bioactive 55% vs bare 66%) at baseline.9 These are well-known risk factors that are believed to degrade procedural morbidity, angiographic recurrence, and mortality.29 Pooling the results of uncontrolled studies with groups that are heterogeneous for such risk factors at baseline is therefore flawed. In contrast, all patients in the current meta-analysis were randomized, which is the best method to equally divide risk factors across treatment groups. The internal validity of the current study is high because the analysis was based on high-quality RCTs of adequate size with high follow-up rates and low risk of bias. The trials were performed across five continents, which increases the external validity of this meta-analysis. The results of this meta-analysis are generalizable to routine practice since patients with ruptured and unruptured aneurysms were included and there were no constraints on the use of assist devices. The most recent review did not approach authors for missing data and excluded most studies for incomplete reporting of outcomes.9 This is an important source of bias. In contrast, it is notable that the senior authors of all but one trial agreed to provide missing data for the current study.11 This ensured that no studies were excluded for incomplete reporting of outcomes. Potentially, there could be differences in efficacy between polyglycolic acid coils, polyglycolic acid/lactide coils, and hydrogel bioactive coils. However, heterogeneity analysis did not identify bioactive coil type as a source. In addition, subgroup analysis of a homogenous group consisting of three RCTs on hydrogel demonstrated similar results, with hydrogel coils reducing residual aneurysms compared with bare coils.
Individual RCTs have concluded that the outcome after bioactive and bare coiling is similar. This could potentially be due to a type 2 error and therefore it is valuable to increase the power of statistical analysis by pooling the results of these RCTs in meta-analyses. A very large RCT would be necessary to exclude a clinically significant difference in rare events such as perforations and thromboembolic complications. By pooling RCTs, the power of the current meta-analysis is substantial with a patient population of 2168 subjects. As a result, the current study has found that bioactive coiling is associated with superior mid-term angiographic results. Bioactive coils have been designed to reduce recurrence and reintervention rates with the hope that these coils would outperform bare coils in these areas. Angiographic recurrence is a clinically relevant surrogate because it is associated with a risk of aneurysm rupture and can lead to reintervention in the long term.30–32 The current analysis is limited by the fact that long-term follow-up is not yet available. At present, only mid-term outcome has been published for these trials. The mean follow-up for this meta-analysis is 10 months. Differences in rates of aneurysm rupture and reintervention are expected to develop with extension of follow-up beyond 10 months, and therefore the long-term results of these trials need to be awaited and pooled in meta-analyses. Another limitation is the fact that patients were treated between 2004 and 2014. Since then, coil technologies and approaches have improved by, for example, the development of softer bare platinum coils which ensure better packing and aneurysm occlusion. Therefore, once randomized studies based on these novel techniques become available, these trials should be included in meta-analyses with subgroup analyses to identify potential advances compared with the coiling techniques evaluated in this review.
Conclusions
Bioactive coils ensure a higher rate of complete aneurysm occlusion while reducing the rate of residual neck aneurysms compared with bare coiling in the mid-term. Hydrogel coils reduce residual aneurysms compared with bare coils. There was, however, no difference in the periprocedural outcome, rate of late aneurysm rupture, or reintervention. While there is level 1a evidence to show more complete aneurysm occlusion, longer term follow-up is needed to determine if this translates into clinical significance.
References
Footnotes
Contributors All authors participated substantially in the conception and design of this manuscript, the analysis and interpretation of data, drafting the article and revising it critically, and all authors have seen and approved the final version of the manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.