Article Text

Abstract
Background Different endovascular modalities have been applied to the treatment of vertebral artery dissecting aneurysms, the most commonly used being internal trapping and stent-assisted coiling, although the ideal treatment remains controversial.
Objective To perform a meta-analysis to study clinical outcomes of patients with vertebral artery dissecting aneurysms who were treated with internal trapping or stent-assisted coiling.
Materials and methods We conducted a meta-analysis of eight retrospective studies that compared internal trapping with stent-assisted coiling for the treatment of vertebral artery dissecting aneurysms. The primary outcomes of this study were immediate occlusion, long-term occlusion, good outcome ratio, perioperative mortality, and angiographic recurrence. Subgroup analyses were conducted of patients with ruptured versus unruptured vertebral artery dissecting aneurysms.
Results Eight studies comprising a total of 188 patients were included in the analysis. For ruptured cases, in comparison with stent-assisted coiling groups, the patients treated with trapping techniques had a higher rate of immediate postoperative occlusion (OR=0.165; 95% CI 0.067 to 0.405; p<0.01), although there was no significant difference in long-term occlusion (OR=1.059; 95% CI 0.033 to 34.121; p=0.974), good clinical outcome rates, recurrence rates, and perioperative mortality. For unruptured cases, patients in the trapping groups also had higher immediate occlusion rates than those who underwent stent-assisted coiling (OR=0.175; 95% CI 0.043 to 0.709; p=0.015), while rates of both recurrence and good clinical outcome were similar between the two groups.
Conclusions Both internal trapping and stent-assisted coiling are technically feasible for ruptured vertebral artery dissecting aneurysms, with high rates of good long-term neurologic outcomes and low recurrence and mortality rates. For unruptured aneurysms, conservative treatment is recommended. When a posterior inferior cerebellar artery (PICA) origin is involved, bypass surgery or vertebral artery-to-PICA stent placement plus coil embolization should be considered.
- Aneurysm
- Coil
- Stent
- Intervention
Statistics from Altmetric.com
Introduction
Intradural vertebral artery dissecting aneurysm (VADA) has been recognized as an important cause of subarachnoid hemorrhage (SAH) and ischemic stroke.1 Given its minimally invasive characteristics, endovascular treatment of VADA has become the dominant approach. The two most commonly used methods are internal trapping and stent-assisted coiling, although selection of the ideal treatment remains controversial. Ruptured VADA have a high risk of subsequent rebleeding and a high mortality rate.2 Although internal trapping was previously the preferred treatment, with the advent of appropriate use of antiplatelet agents and newly developed flow diverters, stent-assisted coiling has also shown favorable safety and efficacy in treating ruptured VADA. Unruptured VADA usually have a benign course;3 however, the opportune time and appropriate type of treatment are unclear. As most studies on the treatment of VADA are small single-center case series, we conducted a meta-analysis of retrospective studies dealing with internal trapping or stent-assisted treatment of VADA to compare the safety and efficacy of these two common endovascular treatment modalities.
Materials and methods
Literature search
The databases of PubMed, EMBASE, Cochrane Library, China National Knowledge Infrastructure (CNKI), Chinese Biomedical Literature database (CBM), WANFANG, and SINOMED were carefully searched. The keywords “vertebral artery dissection,” “vertebral artery dissecting aneurysms,” “embolization,” “coil,” “stent,” “flow diverter,” and “trapping” were used in both “AND” and “OR” combinations. The search was limited to articles published between 2000 and June 2015 in English and Chinese. The references were also reviewed to identify further relevant studies. All studies reporting patients treated with internal trapping and stent-assisted coiling for VADA were selected. Inclusion criteria were a series of more than patients, which includes both internal trapping and stent-assisted coiling, with data available on clinical and/or angiographic outcomes. Exclusion criteria were a series involving solely internal trapping or stent-assisted coiling, and provision of insufficient information.
Data extraction
The following information was extracted: clinical presentation (ruptured or unruptured), treatment technique (stent-assisted coiling or trapping), long-term good neurologic outcome, immediate angiographic occlusion, long-term angiographic occlusion, perioperative mortality, and recurrence. Of note, the long-term follow-up means not less than 6 months and the immediate following occlusion generally refers to within 3 days, according to previous literature. Good neurologic outcome was defined as a modified Rankin Scale score of 0–2, a Glasgow Outcome Scale (GOS) of 4–5, or a Karnofsky score of 50–100; poor neurologic outcome was indicated by a GOS of 1–3 or a Karnofsky score of 0–40.
Literature quality assessment
Quality ratings were made according to the modified Jadad scale. The Jadad criteria included four aspects: whether the study was described as randomized; whether allocation concealment was described; whether the study was double blind; and whether there was a description of withdrawals and dropouts. The Jadad score ranged from 0 to 7. A score of 1–3 indicates poor quality and 4–7 high quality. We included only studies with a Jadad score of at least 4. Two independent reviewers assigned quality ratings, and resolved any disagreements by discussion and consensus or by consulting a third independent party.
Statistical analysis
For postsurgical outcomes, immediate occlusion rates, long-term occlusion rates, recurrence rate, and mortality, statistical analyses were performed with STATA 12.0 (StataCorp LP, College Station, Texas, USA). For dichotomous outcomes, the OR and 95% CIs for determination of preoperative embolization were calculated. The Galbraith figure, Cochran's Q test, and I2 test (variation in OR attributable to heterogeneity) were all performed to judge the heterogeneity between the included studies. If all the points in the Galbraith figure are located within the area between the up line and the down line, this can be taken as evidence of homogeneity. Heterogeneity was also considered to be significant at p<0.10 for the Q statistic. I2 values of 25%, 50%, and 75% were used as evidence of low, moderate, and high heterogeneity, respectively. If there was no evidence of statistical heterogeneity between studies, a fixed-effects model was applied; otherwise, the random-effects model of DerSimonian and Laird was applied in the presence of significant heterogeneity.
To test the robustness of the results, a sensitivity analysis was performed by the one-at-a-time method, which meant omitting one study at a time and repeating the meta-analysis. If the omission of one study significantly changed the result, this implied that the result was sensitive to the studies included. Potential publication bias was assessed by visual inspection of the funnel plot: an asymmetric plot suggested possible publication bias. An Egger linear regression test at the p<0.01 level of significance was also performed to assess the publication bias. If the included studies were not sufficiently large, meta-regression was not performed.
Results
Literature review
A flow chart showing the procedure for identifying the studies is presented in figure 1. A total of 429 articles were identified through the initial literature search, 378 of which were excluded by the title and abstract review because they were deemed not relevant to our study. Fifty-one studies were reviewed in additional detail, 23 of which were excluded because they were either case reports or provided insufficient information. As this meta-analysis is for retrospective cohort studies with dichotomous data (studies that looked at both treatment techniques head-to-head), those studies investigating only one technique, do not meet the requirements of this kind of meta-analysis, although this does not mean that they were incorrectly done or lacked merit. For this reason, another 20 studies were excluded (these studies would be used to conduct a meta-analysis for single ratios in the future). Eventually, eight studies comprising 188 patients were included.4–11
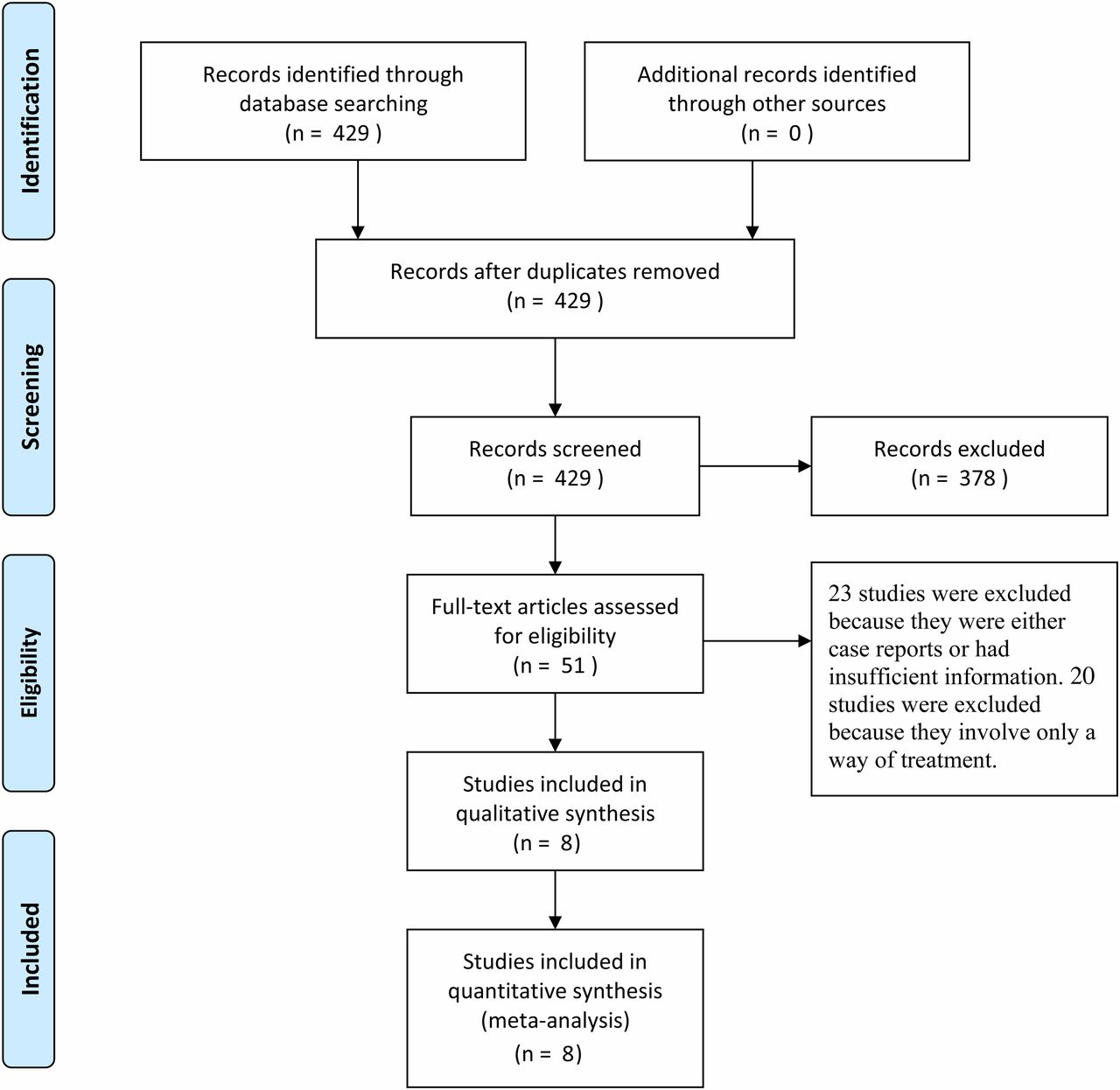
Flow chart showing the study selection procedure.
Baseline characteristics and quality assessment of included studies
One hundred and forty-nine patients (79.3%) presented with ruptured VADA and 39 (20.7%) with unruptured VADA. Ninety-five patients (50.5%) were treated with internal trapping and 93 (49.5%) with stent-assisted coiling. The length of follow-ups of all the included eight studies are listed in table 1.
Detailed data of the meta-analysis in terms of postsurgical outcomes of ruptured aneurysm and the Jadad scores
The meta-analysis covered postsurgical outcomes, immediate occlusion rates, long-term occlusion rates, recurrence rates, and mortality, for both ruptured and unruptured VADA. Detailed data for postsurgical outcomes of ruptured aneurysm treatment are summarized in table 1. Based on the Jadad scale scores, all the studies were rated as high quality (table 1). Among these studies, no patients were treated with flow diverters in the stent-assisted coiling groups, thus subgroup analysis for a flow diverter group could not be performed.
Considering all patients treated with both modalities, the immediate occlusion rate was 81.51% (95% CI 72.83% to 90.74%) and long-term occlusion rate 96.39% (95% CI 86.60% to 102.28%); angiographic recurrence rate was 9.25% (95% CI 4.99% to 14.81%), and perioperative mortality rate 5.32% (95% CI 1.06% to 10.09%). Perioperative mortality for ruptured VADA was 8.01% (95% CI 2.41% to 17.38%) and for unruptured VADA, 0.61% (95% CI −1.14% to 2.80%).
Ruptured VADAs: stenting versus trapping
Data relating to postsurgical outcomes, immediate occlusion, long-term occlusion, recurrence, and mortality were analyzed. Relative parameters involved in this meta-analysis using heterogeneity tests, publication bias tests, and data from Forest plots are summarized in table 2. Taking postsurgical outcomes as an example, from the Galbraith figure (figure 2) we can see that all points fall between the two axes, which can be taken as evidence of homogeneity among these studies (Q=2.78, df=7, I2=0.0%). Consequently, we summarized the data with a fixed-effects model instead of a random-effects model (figure 3). Pooled data showed that patients treated with trapping techniques had higher rates of complete occlusion on immediate postoperative angiography than those treated with stent-assisted coiling (OR=0.165; 95% CI 0.067 to 0.405; p<0.01, although this difference was not statistically significant over the long term (OR=1.059; 95% CI 0.033 to 34.121; p=0.974). Perioperative morbidity rates were similar in the stent-assisted coiling and trapping groups (OR=1.136; 95% CI 0.424 to 3.043; p=0.80). Long-term satisfactory clinical outcome rates were also similar between the two groups (OR=0.666; 95% CI 0.288 to 1.539; p=0.342); the same was true for rebleeding (recurrence) rates (OR=2.121; 95% CI 0.842 to 5.339; p=0.11).
Relative parameters involved in this meta-analysis as measured by heterogeneity tests, publication bias tests, and data of Forest plots

Galbraith figure for postsurgical outcomes of ruptured vertebral artery dissecting aneurysm.

Forest plots for postsurgical outcomes of ruptured vertebral artery dissecting aneurysm.
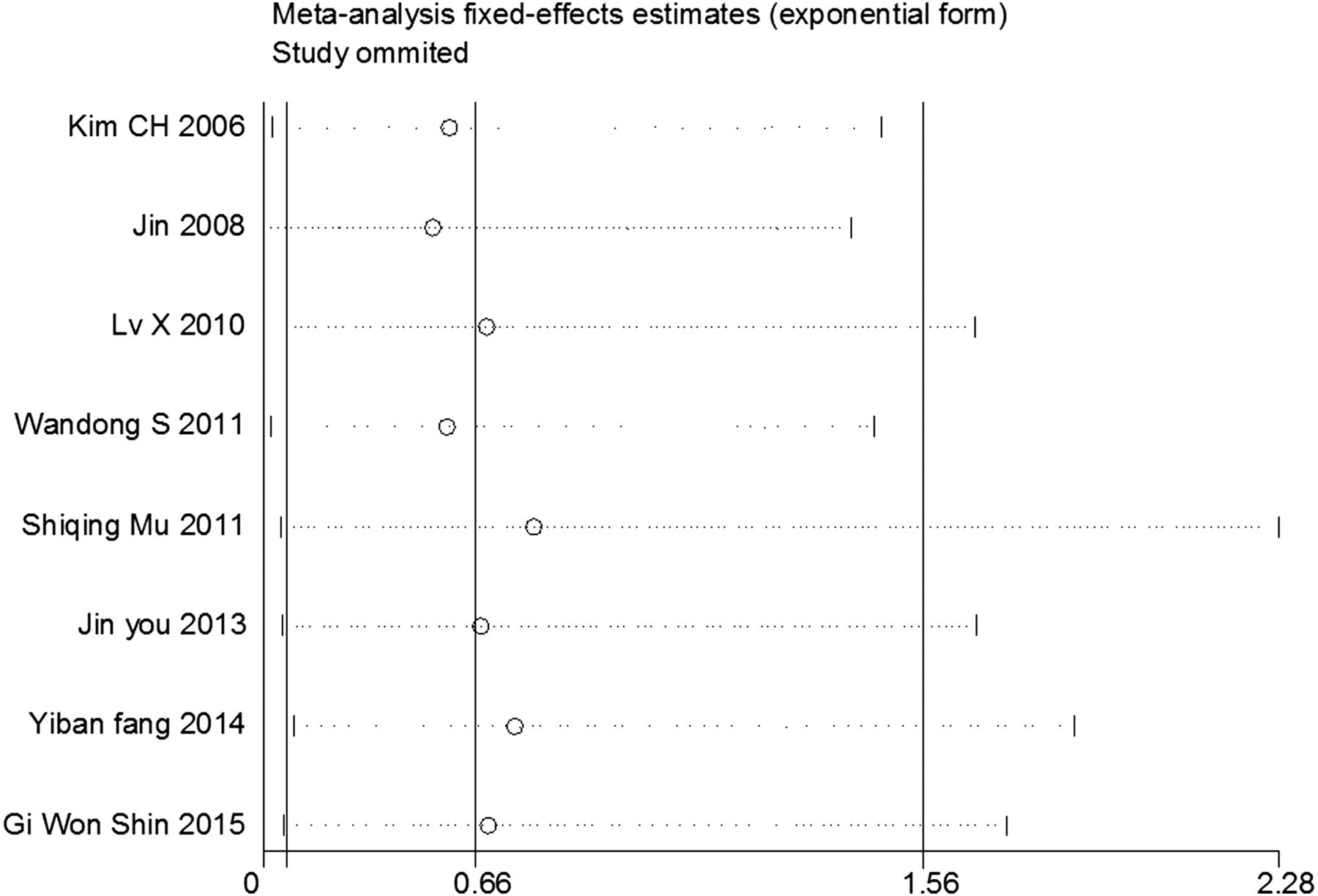
A sensitivity analysis was performed to assess the influence of each individual study on the pooled OR by omitting each individual study one at a time. The results suggested that no individual studies significantly affected the pooled OR (figure 4), indicating a statistically robust result. A funnel-plot analysis of publication bias among the eight relevant studies showed a symmetric distribution (figure 5). A Begg's test and an Egger test also showed no significant statistical evidence of publication bias (95% CI −0.43 to 2.67; p=0.129).

Sensitivity analysis of literature reporting postsurgical outcomes of ruptured vertebral artery dissecting aneurysm. Results were computed by omitting each study in turn. Meta-analysis fixed-effect estimates (exponential form) were used. The two ends of the dotted lines represent the 95% CI.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Begg's funnel plots for postsurgical outcomes of ruptured vertebral artery dissecting aneurysm. Each circle, whose size represents its sample weight, represents a separate study for the indicated association. Logor, natural logarithm of OR. Horizontal line indicates the magnitude of the effect.
Unruptured VADAs: stenting versus trapping
Patients treated with trapping techniques had higher rates of complete occlusion on immediate posttreatment angiography than those treated with stent-assisted coiling techniques (OR=0.175; 95% CI 0.043 to 0.709; p=0.015). Long-term occlusion rates and mortality rates were not analyzed owing to insufficient data. Recurrence rates were similar in the stent-assisted coiling group and the trapping group (OR=2.128; 95% CI 0.626 to 7.234; p=0.226). Rates of good clinical outcome were also similar in two groups (OR=0.634; 95% CI 0.205 to 1.960; p=0.429). Comparative data are presented in table 2.
Discussion
This meta-analysis showed that both internal trapping and stent-assisted coiling techniques are effective in the treatment of ruptured and unruptured VADA. Both techniques resulted in high rates of favorable long-term neurologic outcome and similar low rates of recurrence and mortality.
The most common clinical presentation of VADA was SAH, accounting for 75.9%.12 For ruptured VADA formed by the disruption of the internal elastic lamina13 ,14 with a high risk of rebleeding in the acute stage,2 ,15 internal trapping is generally the preferred treatment, as it is thought to be the most reliable endovascular method to prevent re-rupture.16 ,17 Although internal trapping has been widely used, it does have some drawbacks. First, obliteration of the parent vessel may cause lateral medullary or cerebellar infarction, even when the trapping is performed on the non-dominant side or after a negative result on a balloon occlusion test.18 The two main reasons for the development of ischemic symptoms are anatomy and hemodynamics. When the dissecting aneurysm is located distally to the posterior inferior cerebellar artery (PICA), this segment of the vertebral artery often has more perforating arteries than are found in the segment proximal to its origin,19 so that trapping tends to cause occlusion of the perforators. When the dissecting aneurysm is located proximally to the PICA, the PICA is supplied by the contralateral vertebral artery, potentially giving rise to a ‘dead space’ between the PICA and the site of occlusion with slow blood flow, which might cause occlusion of the perforators. Second, occlusion of the vertebral artery may increase blood flow and pressure in the contralateral vertebral artery, which may lead to enlargement of the contralateral vessels, even inducing rupture of pre-existing contralateral aneurysms.20 Lastly, early rebleeding is not uncommon.
The most important consideration in the treatment of VADA is weighing the risks of treatment with the risks of the natural history of these lesions. Ruptured VADA are known to have a poor natural history with high rates of rebleeding and mortality. In our unpublished study, we compared mortality rates among patients with ruptured VADA treated with deconstructive techniques and surgical clipping with a small group of patients managed conservatively and found that mortality rates in the conservative group were 50% compared with 20% in the treatment group. In the treatment of ruptured VADA, stent-assisted coiling is often thought to result in higher recanalization and mortality rates.21 However, with the advent of appropriate use of antiplatelet agents for VADA treatment, it is likely that outcomes for patients with ruptured VADA treated with stent-assisted coiling will improve, with higher rates of long-term angiographic occlusion and lower rebleeding rates. The current generation of stents has a much higher rate of metal coverage. An overlapping stent technique is feasible to decrease stent porosity.22 Recently, flow-diverting stents have also been adopted in the treatment of VADA.23 All these techniques improve the effect of diverting the inflow of the aneurysm and promote immediate thrombosis while also maintaining parent artery patency.
Fang et al compared internal trapping in 20 cases with stent-assisted coiling in 19 cases for the treatment of ruptured VADA. In the trapping group the immediate total occlusion rate was 80%, which improved to 88.9% during follow-up, compared with an immediate total occlusion rate of 47.4% in the stenting group that improved to 100% during follow-up. There was no difference in recurrence and rebleeding rates between the trapping and stenting groups.4 Sonmez et al performed a systematic review of endovascular treatment of VADA in 478 patients, and compared deconstructive and reconstructive techniques in the treatment of ruptured VADA. Patients treated with deconstructive techniques had higher rates of complete occlusion on immediate post-treatment angiography than those who underwent reconstructive techniques. However, the perioperative mortality rates were similar in the two groups.24 Our study found that internal trapping techniques resulted in higher postoperative immediate occlusion rates, but with no significant difference in long-term occlusion, good clinical outcome, recurrence, and perioperative mortality. The main obstacle to the use of stent-assisted coiling for the treatment of ruptured VADA is concern about the increased risk of hemorrhagic complications caused by perioperative antiplatelet medication. However, the relatively lower immediate total occlusion rate of stent-assisted coiling caused no obvious deterioration in perioperative rebleeding and mortality. Administering loading doses of dual antiplatelet drugs shortly before stenting has proved to be essential and safe.25
Unruptured vertebral artery dissections usually have a benign course,3 with conservative treatment such as anticoagulation and antiplatelet medication recommended as the first line of treatment. Kim et al26 followed up 191 patients with symptomatic intracranial unruptured vertebrobasilar artery dissection for a mean of 46 months. Clinical outcomes were favorable in all patients without ischemic symptoms, and in most patients with ischemic presentation. None of the VADA caused SAH. Kobayashi et al3 followed up 113 patients with unruptured VADA without ischemic symptoms at presentation for a mean of 3 years and found a 3% morbidity at follow-up, with two patients having clinical deterioration due to mass effect and one patient having ischemic stroke and hemorrhage. Five patients had enlargement of the aneurysm in this series. Therefore, when treating unruptured VADA it is necessary to measure the risks of treatment and the risks conferred by the natural history. Li et al27 reviewed 65 consecutive patients with unruptured VADA who underwent endovascular treatment, among whom patients who underwent internal trapping had more ischemia symptoms than those in the stent-assisted coiling group. In this study, good clinical outcome rates and recurrence rates were similar between the two groups. Owing to the absence of a standardized uniform assessment of complications and insufficient data, the perioperative morbidity was not analyzed. However, we can conclude that only those patients with enlarged aneurysms and those with progressive ischemia after medical management should be recommended for endovascular treatment, and that stent-assisted coiling might be the first choice.
PICA involvement was seen in 14.62% of VADA cases.12 When the PICA origin was involved neither internal trapping nor stent-assisted coiling could completely obliterate the dissected segment to preserve the blood flow to the PICA. Kim et al28 followed up 111 patients, among whom there was a 13% recurrence after endovascular treatment of VADA, and PICA involvement was the only independent risk factor for recurrence after endovascular treatment. In a ruptured VADA, recanalization is associated with a high rate of rebleeding. Thus for these types of lesions, bypass surgery should be considered.29 ,30 Vertebral artery (VA)-to-PICA stent placement plus coil embolization is also a reasonable option.31
To perform trapping for ruptured supra-PICA VADAs and to sacrifice the PICA in cases with other poor collateral circulation covering the PICA territory, one should consider bypass techniques, such as occipital artery–PICA anastomosis, to reduce the complication of symptomatic PICA territory infarction. In addition to ischemic complications of the PICA during endovascular procedures, the possibility of occluding the anterior or posterior spinal artery arising from the dissected segment should be considered. In our experience, severe ischemic complications such as quadriparesis or respiratory disturbance might occur if the anterior spinal artery originates only from the side of the dissected VA in patients with VA aneurysms located distal to the PICA. Therefore, for trapping vertebrobasilar VADAs, these factors should definitely be considered to reduce the poor ischemic complications.
Limitations
First, because decisions about treatment of VADA depend on multiple factors, these studies are limited by their non-comparative and non-randomized nature. Second, no validated, uniform classification system is available for VADA, the location of the lesion, the presence of collateral circulation, and the involvement of branch vessels, which all affect the feasibility of treatments. Patient selection and publication bias could not be avoided. Third, because there is no uniform assessment of complications and the data were incomplete, perioperative morbidity was not analyzed.
Last, but not least, since no patients were treated with flow diverters in the stent-assisted coiling groups among all these eight studies, subgroup analysis for a flow diverter group could not be performed. Flow diverters have been developed to treat intracranial aneurysms. These endovascular devices are placed within the parent artery rather than the aneurysm sac. They alter the hemodynamics at the aneurysm/parent vessel interface, resulting in gradual thrombosis of the aneurysm over time. Subsequent inflammatory response, healing, and endothelial growth shrink the aneurysm and reconstruct the parent artery lumen while preserving perforators and side branches in most cases. Although flow diverters have already allowed treatment of previously untreatable wide neck and giant aneurysms, risks remain, including in-stent thrombosis, perianeurysmal edema, distant and delayed hemorrhages, and perforator occlusions. This newly developed technique need to be improved and has not yet been widely used. Possibly because of this, none of the eight studies included these patients. However, because flow diverters have expanded the therapeutic options for treatment of cerebral aneurysms, further research is expected.
Conclusions
For ruptured VADA both internal trapping and stent-assisted coiling are technically feasible, with high rates of good long-term neurologic outcomes and low recurrence and mortality rates. Overlapping stents and appropriate use of antiplatelets may decrease the risk of rebleeding and recurrence. For unruptured VADA, conservative treatment is recommended. For patients with enlarged aneurysms and those with progressive ischemia after medical management, both internal trapping and stent-assisted coiling are good choices. When the PICA origin is involved in a ruptured VADA, bypass surgery or VA-to-PICA stent placement plus coil embolization should be considered.
References
Footnotes
JG, GL, HZ, and RW contributed equally.
Contributors All authors participated in drafting the article and revising it critically for important intellectual content. All authors made substantial contributions to the conception and design, acquisition of the data, and analysis and interpretation of the data.
Funding This work was supported by National Natural Science Foundation of China (81301061).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors are willing to share spreadsheets from their data extraction on request.