Article Text

Abstract
Objective To determine the safety and effectiveness of a new low-profile, laser-cut, closed-cell stent system in the treatment of complex intracranial aneurysms.
Methods A total number of 43 patients with complex intracranial aneurysms were treated using 60 Acandis Acclino stent systems (follow-up 2012–2016; mean 11 months). 36 patients presented with wide-necked intracranial aneurysms, dissecting aneurysms were seen in 7 patients. 39 patients received stent-assisted coiling. We analyzed demographic data and follow-up results.
Results Sixty stents were successfully deployed. In one paraophthalmic internal carotid artery aneurysm the stent could not be placed. Thirty-three wide necked aneurysms were treated by single or multiple stent-assisted coiling. Complete occlusion was achieved in 31 of those cases (94% Raymond−Roy occlusion classification, RROC 1). Two patients showed stable residual aneurysmal filling (RROC 3). In three wide-necked aneurysms, sole stenting was the preferred treatment. For dual stent-assisted procedures the kissing-Y stenting technique was successfully performed in 11 aneurysms. In all dissecting aneurysms constructive therapy with stenting and preservation of the affected parent artery was achieved. Additional subsequent coil embolization was intentionally planned and successfully performed in 6 of the 7 dissecting aneurysms. The overall directly procedure-related complication rate was 7%, including one death.
Conclusions Endovascular treatment of complex intracranial aneurysms using Acclino stents is a feasible and safe procedure with low complication rates. Even severe cases can be treated among others using the kissing-Y stenting technique, with good mid-term results.
- Aneurysm
- Stent
- Intervention
- Angiography
Statistics from Altmetric.com
Introduction
Endovascular treatment with sole coiling of wide-necked, complex bifurcation and giant aneurysms is often limited or even not feasible. The stent-assisted coiling technique clearly reduces the recurrence rate.1 Since the first description of this technique in 1997,2 several flexible self-expanding intracranial stents have been introduced and clinically used for the treatment of previously uncoilable intracranial aneurysms.3–7 Low-profile self-expandable stents such as LVIS Jr (MicroVention, Tustin, California), LEO baby (Balt, Montmorency, France), and Acclino (Acandis, Pforzheim, Germany) broadened the range of endovascular treatable aneurysms as their design enables deployment in small distal arteries and delivery through 0.0165 inch microcatheters. Acclino stents received a CE mark for use in the European Union in June 2012. They are the second generation of closed-cell Acandis stents and are the followers of the first generation of Acandis Neuro Closed stents. The Acclino flex stents were introduced in 2014 and replaced the previous Acandis stent generation. Two recent studies have described the initial clinical experience with Acclino stents in the treatment of intracranial aneurysms in small cohorts.8 ,9
In our retrospective study, we want to present our results of both later generations of Acclino stents, which were used for single, double (including kissing-Y stenting technique), and multiple stent-assisted coiling. We analyzed the technical feasibility and safety in clinical practice and evaluated the mid-term results in 43 patients with complex intracranial aneurysms.
Patients and methods
Patients
In a retrospective review, we identified 43 patients with various intracranial aneurysms treated electively with stent-assisted endovascular techniques by using at least one Acclino stent between June 2012 and October 2015 with a follow-up until April 2016. The clinical data were obtained from the patient's medical files. Written informed consent was obtained from all patients. Approval was obtained from the local hospital's institutional review board.
Antiplatelet regimen
Premedication for all procedures included 100 mg acetylsalicylic acid (ASA) and 75 mg clopidogrel daily for at least 10 days before the intervention. A multiplate function test was performed before the procedure to ensure a sufficient response to clopidogrel and ASA. The measured values had to be below the reference standards. During the intervention, heparin was administered intra-arterially with close monitoring of the activated clotting time, keeping it between 200 and 350 s. ASA 100 mg daily for at least 1 year and clopidogrel 75 mg daily for at least 6 weeks were prescribed after the intervention.
Interventional procedure
All patients underwent the intervention under general anesthesia. The angiographic examination was performed on a biplane angiographic system (Axiom Artis BA biplane, Siemens, Erlangen, Germany). A 5F or 6F Envoy guiding catheter (Codman & Shartleff, Raynham, Massachusetts, USA) was positioned in the internal carotid artery (ICA) for aneurysms of the anterior circulation or in one vertebral artery (VA) for aneurysms of the posterior circulation, respectively. We used the Acandis Acclino 1.9 microcatheter set or in cases of the new Acandis Acclino flex stents, the NeuroSlider 17 microcatheter. A middle marker on the stents' transport wire should be positioned at the aneurysm neck. For cases of kissing-Y stenting, two microcatheters were advanced coaxially through the guiding catheter to the aneurysm site, using different microguidewires. When the microcatheters were positioned correctly, the guidewires were withdrawn. The stents were sequentially deployed side by side through the microcatheters. The microcatheter used for stent deployment subsequently was navigated through the stent interstices in the aneurysmal sac. Then, detachable coils were delivered within the aneurysm.
Follow-up
Postprocedural angiograms were obtained immediately after coiling of the aneurysm. All patients underwent postinterventional cranial CT directly after the intervention. The patients' first follow-up was performed at 3–6 months, usually by both DSA and MRI with 3D time-of-flight and contrast-enhanced MR angiography. The second follow-up was carried out 1 year later. Postinterventional angiograms and follow-up MR angiography and DSA were reviewed and evaluated based on the Raymond−Roy Occlusion Classification (RROC)10 by two experienced interventional neuroradiologists (senior author >35 years’ experience) in consensus.
Acandis Acclino stents
We used two different types of Acclino stents, the 1.9 F stent system and the newer Acclino flex stent system. The stents are self-expandable nitinol microstents with a closed-cell design. The stent system features three radio-opaque markers at the proximal and the distal end of the stent, indicating correct position and expansion of the stent. The three transport wire markers allow increased visibility and a safe and precise placement of the stent. The distal end of the transport wire has a highly flexible atraumatic soft tip. The Acclino flex stent system is the third generation of closed-cell stents of Acandis. The new optimized asymmetric cell design ensures an improved vessel wall apposition even in tortuous vessels. Both later generations of stents are available with 3.5 mm and 4.5 mm diameters, each of them with five different stent lengths (15 mm, 20 mm, 25 mm, 30 mm, 35 mm), allowing a broad range of vessel sizes from 1.5 mm to 4 mm to be treated. Since 2015, the Acclino flex stent system is also offered in 6.5 mm diameter with four different stent lengths (20 mm, 25 mm, 30 mm, 35 mm), allowing vessels up to 6.0 mm in diameter to be treated. The 1.9F stent is compatible with any 0.0165″ microcatheter, the Acclino flex stent is deliverable through a microcatheter of 0.0165″–0.017″ internal diameter, and the new Acclino flex stent with a 6.5 mm diameter is compatible with any 0.021″ microcatheter. Sequential coil embolization of the aneurysm can often be performed without changing the microcatheter after stent deployment. The stents are retrievable and repositionable if an adjustment of the stent is necessary, even if the stent was deployed between 50% and 90% of its total length.
Results
Forty-three aneurysms in 43 patients were treated with 60 Acclino stents between June 2012 and April 2016. Four patients with subarachnoid hemorrhage received sole partial coiling of the aneurysm dome in the acute phase. In these cases, dense packing of the aneurysmal sac was not always sufficiently achieved. Therefore, additional stent-assisted coiling was performed a few weeks later. In an emergency coiling of a ruptured anterior communicating artery (AcomA) aneurysm, coil protrusion into the parent artery followed by periprocedural thromboembolism was initially managed by administration of tirofiban. Subsequently, an Acclino stent was deployed to protect the parent vessel and to avoid further thromboembolism. The 24 months’ follow-up showed complete aneurysmal occlusion. Thirty-six of 43 aneurysms were complex wide-necked aneurysms, the other seven were dissecting aneurysms. Sixteen patients were treated with two or more stents. Eleven of these patients with a complex bifurcating aneurysm were treated with the kissing-Y stenting technique.7 The aneurysm distribution was as follows: 14 at AcomA, being the most common aneurysm location, 8 at basilar artery (BA), 7 at the intracranial ICA, 5 at the middle cerebral artery (MCA), 5 at distal VA segments, 2 at the anterior cerebral artery (ACA), 1 at the posterior inferior cerebellar artery, and 1 at the posterior cerebral artery (PCA). The mean aneurysm size was 7.7×5.8 mm (range 2–17 mm).
In six patients intracranial stent therapy was necessary owing to aneurysmal regrowth and one patient was previously insufficiently clipped. In one case, periprocedural thromboembolism during aneurysmal coiling was managed by stent placement, preserving the parent arteries. Sixty stent deliveries were technically feasible without any difficulties. In one paraophthalmic ICA aneurysm the stent could not be placed appropriately and safely. In this case a different stent was successfully used.
Initially, we used the second-generation stents in 26 patients. Since the introduction of the Acclino flex system in 2014, we have used the new system in a consecutive series of 16 patients. In one patient both stent systems were used. Table 1 gives information about the stents and vessel diameters.
Stent diameter in relation to mean vessel diameter
The mean follow-up time was 11 months. We report no stent migration or fracture during the follow-up. In three of the 36 wide-necked aneurysms we performed no coiling or incomplete coiling, due to vessels arising out of the aneurysmal sac. For this reason, we excluded those three aneurysms from the statistical assessment using the RROC. For the remaining 33 wide-necked aneurysms, complete occlusion in postprocedural angiograms was achieved in 30 (91% RROC 1) cases. We observed no neck remnants (RROC 2). Three patients had residual aneurysm filling (9% RROC 3). Follow-up demonstrated complete aneurysmal occlusion in 31 patients (94% RROC 1). One residual aneurysm was completely occluded on follow-up (RROC 1). Two patients showed stable residual aneurysmal filling (RROC 3) without clinical significance.
In the subgroup of the 11 wide-necked aneurysms, treated using the kissing-Y technique, one BA/superior cerebellar artery aneurysm was treated by sole stenting because the superior cerebellar artery rose out of the aneurysmal fundus. Seventeen months’ follow-up showed stable aneurysm size. In the aneurysms treated by stent-assisted coiling with the kissing-Y technique 9 of 10 showed immediately complete occlusion (90% RROC 1).
Follow-up of two wide-necked aneurysms treated without, or with incomplete, coiling to avoid infarction in the supplied vascular territory showed stable aneurysm size at 17 and 6 months, respectively.
The aim of endovascular treatment in all seven dissecting aneurysms was constructive therapy. The primary goal of the procedure was to protect the parent vessel with stents. Subsequent coil embolization was performed in six of the seven aneurysms. Deconstructive therapy was not necessary in any case.
Complications
In our series one patient harboring a saccular aneurysm died. The patient presented initially with a wide-necked AcomA aneurysm. Aneurysm rupture occurred during stent deployment of a third-generation Acandis stent followed by subarachnoid hemorrhage. In one patient treated with kissing-Y stent-assisted coiling using two Acclino 1.9F stent systems, postoperative cranial CT showed infarction in both the anterior and posterior circulation, presumably owing to cardiac embolism; atrial fibrillation was in the medical history. Nevertheless infarction due to embolisms caused by the guiding catheter in the aortic arch should be considered for differential diagnosis. For a dissecting aneurysm of the PCA, stent-assisted coiling, using a second-generation Acandis stent, was the preferred planned treatment. Stent deployment was feasible without any technical complications. However, the P2 segment was obliterated at the end of the procedure. In one case of kissing-Y stent-assisted coiling using two Acclino flex stents, a slight intimal hyperplasia (<50%) without any clinical significance was noted at 6 months’ follow-up.
Illustrative cases
Case 1
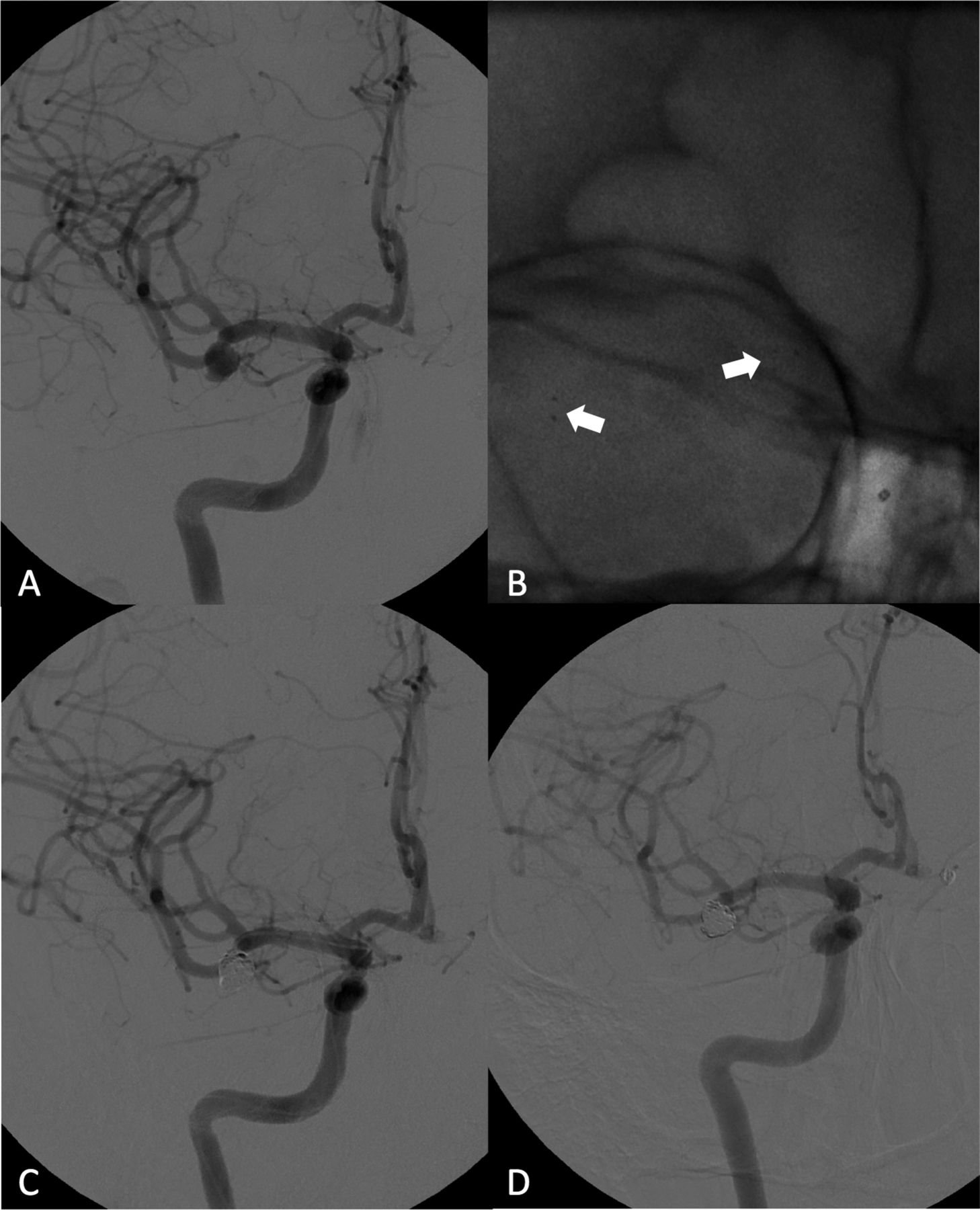
A middle-aged patient presented at our department with three intracranial aneurysms found incidentally on MRI. The patient had a family history of ruptured aneurysms. The patient refused neurosurgical clipping and preferred endovascular treatment. DSA showed a complex wide-necked aneurysm of the right MCA—bifurcation with one M2 branch directly originating out of the aneurysm sac (figure 1A). The MCA aneurysm measured 7×5 mm and was treated by stent-assisted coiling. Initially, a self-expanding 3.5×25 mm Acclino stent was deployed from the above-mentioned M2 branch into the M1 segment (figure 1B). Subsequent coil embolization led to complete occlusion of the aneurysm with preservation of all peripheral MCA branches (figure 1C). No peri- or postinterventional complications occurred and the patient did well after treatment. The 4- and 16-month angiographic follow-up showed complete occlusion of the aneurysm (RROC 1) (figure 1D).
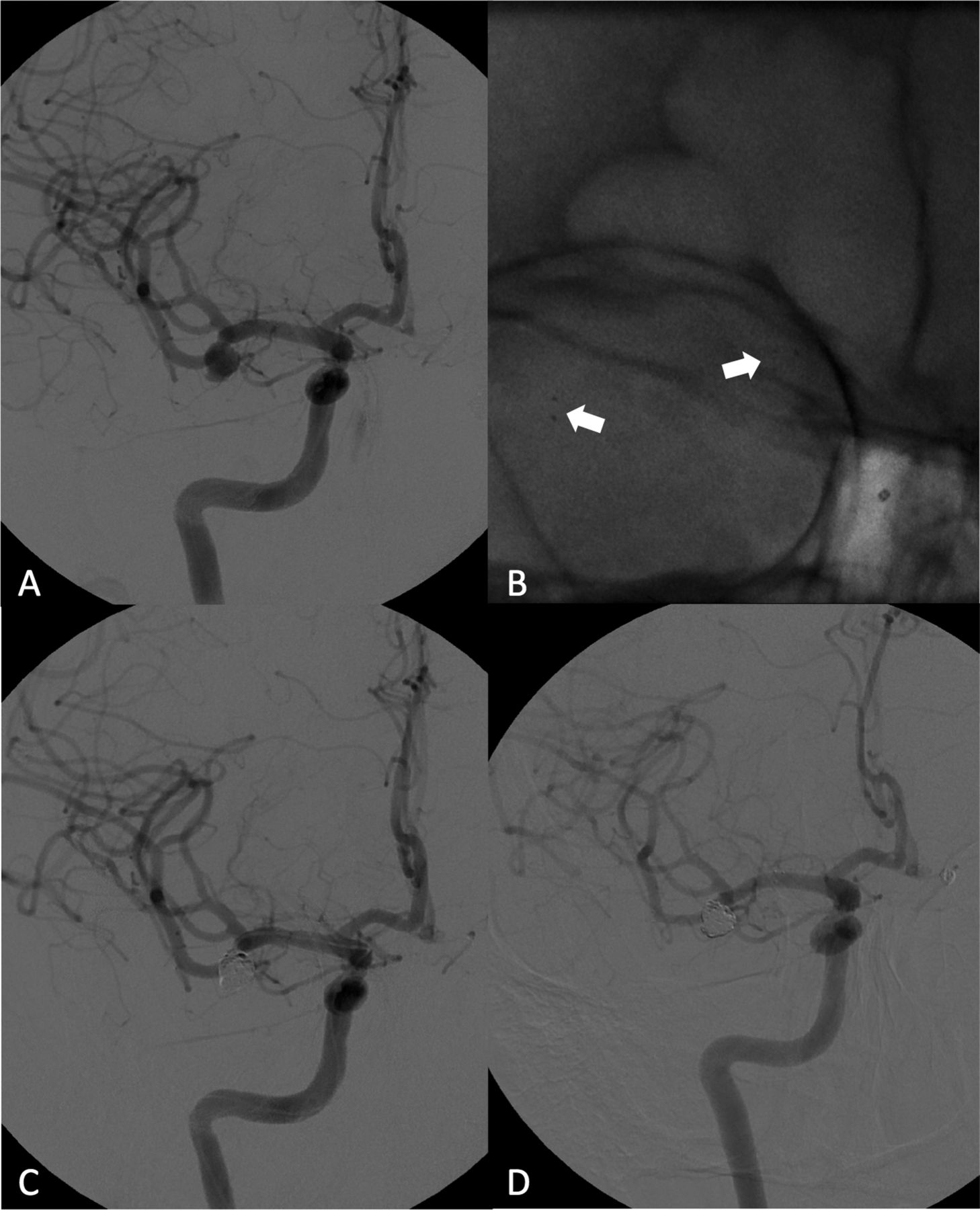
DSA in frontal projection, right internal carotid artery (ICA) injection, showing (A) a dysplastic wide-necked middle cerebral artery bifurcation aneurysm. A non-subtracted image in working projection after stent deployment (M1−M2). Arrows indicate the proximal and distal stent markers (B). Immediate postprocedural (C) and 16 months’ follow-up DSA (D) in frontal view, right ICA injection, showing complete occlusion of the aneurysm with the preserved M2 branch.
Case 2
An elderly patient presented at our department with a partially calcified and thrombosed giant 25×23 mm incidental aneurysm of the right ICA/PCA (figure 2A). The non-thrombosed part of the wide-necked aneurysm measured 17×13 mm on DSA (figure 2B). The right embryonic PCA originated directly at the basis of the aneurysmal sac. There was no supply from the BA to the right PCA. Initially, two Acclino flex stents were simultaneously inserted using the kissing-Y technique (figure 2C–E). One 3.5×25 mm stent was deployed from the embryonic PCA to the supraophthalmic ICA and another 4.5×30 mm stent was deployed from the proximal M1 segment to the supraophthalmic ICA. The two stents were placed side by side in the distal ICA. DSA showed successful bridging of the aneurysm basis with protection of the PCA. Subsequent coil embolization led to complete occlusion of the aneurysm. Postinterventional CT was unremarkable. A 6-month angiographic follow-up showed no recurrence or reperfusion (RROC 1), with a fully preserved and patent right PCA (figure 2F). The patient was completely asymptomatic.

Cranial CT scan showing a partially calcified giant internal carotid artery (ICA) aneurysm (A). DSA in lateral projection, right ICA injection (B), showing the non-calcified part of the giant aneurysm. DSA in roadmap technique (C) and non-subtracted image (D), both in lateral projection, demonstrating the deployment of two Acclino flex stents in kissing-Y stenting technique into the parent arteries (M1—ICA and posterior cerebral artery (PCA)—ICA). Non-subtracted angiographic run (E) after successful deployment of the stents. Arrows indicate the markers of the two stents. (F) DSA 6 months’ follow-up in lateral projection, right ICA injection, showing complete occlusion of the aneurysm (Raymond−Roy Occlusion Classification, RROC1) with a fully preserved PCA.
Case 3
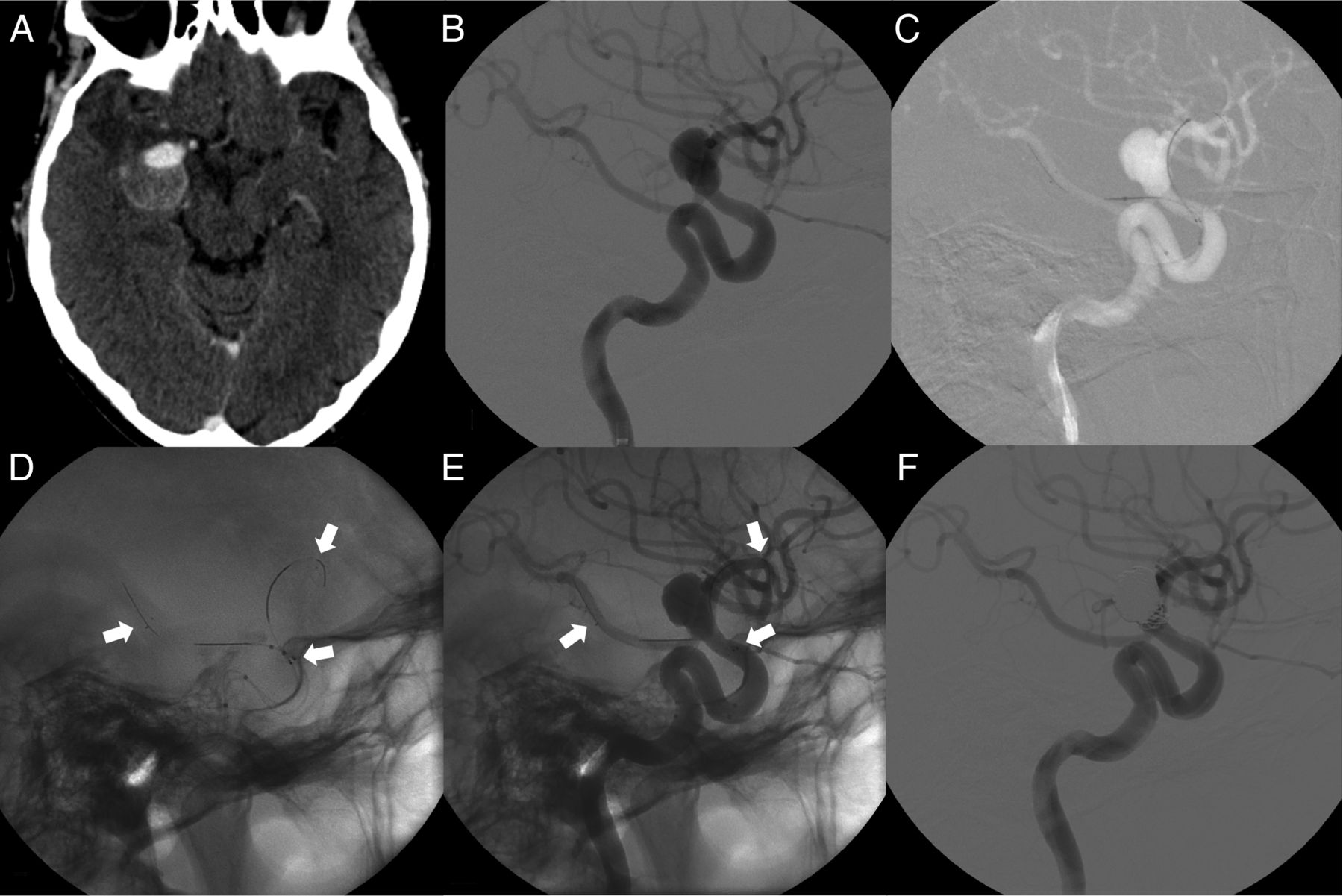
A middle-aged patient presented with an incidentally found 14×14 mm aneurysm at the fusion of the VAs to the BA (figure 3A, B). The patient had a severe headache. Initially, a Neuroslider 17 microcatheter was inserted into each VA and the two microcatheters were placed with both tips in the distal part of the BA. In a second step, two Acclino flex stents (each 4.5×35 mm) were simultaneously inserted and deployed from the middle part of the BA to the aneurysm sac (figure 3C). Using the same microcatheters, another two Acclino flex stents (each 4.5×30 mm) were inserted. Both were telescopically deployed within the previously implanted stents overlapping in the aneurysm sac. Each of the secondarily implanted stents was placed from the aneurysm sac to both V4 segments, respectively (figure 3D). After successful deployment of the four stents, subsequent coil embolization was performed (figure 3E). Postinterventional CT showed no signs of intracranial bleeding or stroke. A 6-month follow-up was unchanged without any recurrence or reperfusion. All four stents were patent (figure 3F).

{kind=link}
{kind=link}
{kind=link}
Cranial CT scan showing (A) a partially calcified giant basilar artery (BA) aneurysm. DSA left anterior oblique view, right vertebral artery (VA) injection, (B) demonstrating a 14×14 mm BA aneurysm at the fusion of the VA. Non-subtracted images obtained during placement of the two distal stents side by side in the BA (C) and during placement of the two proximal stents into each VA (D). Non-subtracted image during coil embolization with microcatheterization through the stent struts (E). Arrows indicate the markers of the distal stents, arrowheads the markers of the proximal stents. DSA in working projection (F) demonstrating successful stent-assisted coiling of the BA aneurysm.
Discussion
The Acclino stents are self-expandable, laser-cut stents with a closed-cell design. They belong to a new generation of highly flexible intracranial stents deliverable through microcatheters with an internal diameter of 0.0165 inches. The Acclino stents are resheathable and repositionable, even if released up to 90% of their total length, allowing precise positioning. This feature is an advantage over Enterprise and LVIS Jr stents, which are retrievable only up to 70–80% of their length.11 ,12 We report no problems in resheathing the stent when not fully deployed.
In our study, we used two different Acclino stents—the second generation of Acandis stents and the third generation, the Acclino flex stents. The second-generation Acandis stents were replaced by the Acclino flex stent. The Acclino flex stent has an asymmetric cell design, facilitating improved vessel wall apposition and conformability in tortuous vessels. Experienced neurointerventionalists reported improved feasibility with better navigation in small distal tortuous vessels due to its reduced axial rigidity. Nevertheless, the visibility of the markers was degraded, especially under fluoroscopy. Meticulous subgroup analysis with a dedicated description of the differences between the two Acclino stent systems is beyond the scope of this work. However, the second generation of Acandis stents is recommended for deployment in arteries with a lumen diameter of between 2 and 4 mm. The Acclino flex stents are available in three different sizes. They are labeled for a broad range of parent artery vessel diameters of between 1.5 mm and 6.5 mm, allowing treatment of complex aneurysms, even very small distal cerebral arteries. The same range of parent vessel sizes applies to the Leo/Leo baby stent, whereas the LVIS Jr stent is intended for arteries with a lumen diameter of between 2 and 3.5 mm.13 ,14
We had no problems in navigating the Acandis microcatheter for coiling through the stent interstices, even through double-layered stents as in a kissing-Y stenting technique. Hence, it was not necessary to trap the coiling microcatheter in the aneurysm sac during stent deployment.
In our study, the Acclino stents were successfully deployed and placed correctly in all but one case. The Acclino stents were used for single or multiple stent treatment (including the kissing-Y stenting technique) of complex intracranial aneurysms where sole coiling did not lead to a complete aneurysm occlusion or was even not feasible. We report one case of a giant complex aneurysm at the fusion of the VAs to the BA with successful telescopic stent implantation of four Acclino stents.
The aim of our study was to present our mid-term experience in stent-assisted endovascular techniques using a new self-expanding microstent.
However, there are several other treatment options for complex intracranial aneurysms.
Balloon-assisted coiling, flow diversion, and intrasaccular flow disruption are alternative commonly used endovascular techniques. Chalouhi et al15 found that balloon-assisted coiling requires higher rates of re-treatment and has lower rates of complete aneurysm obliteration than stent-assisted coiling. The safety and efficacy of flow diverters and flow disrupters for the treatment of complex intracranial aneurysms have already been investigated in several studies with encouraging aneurysm occlusion rates.16–18 The large number of recently developed endovascular treatment options is creating a couple of new challenges for the interventional neuroradiologist. At least, neurosurgical clipping is still an effective treatment for selected intracranial aneurysms.
In our study, we demonstrated that the use of Acclino stents for stent-assisted endovascular techniques of complex intracranial aneurysms leads to a very high mid-term occlusion rate.
Aydin et al13 recently reported an immediate occlusion rate for Leo baby stents of 75% and 85% on follow-up. The immediate occlusion rate using LVIS Jr stents was 73% in a prospective study published in 2014.19 Poncyljusz et al20 reported a RROC 1 of 82% in their LVIS series. Similar results were published by Fiorella et al,21 with a complete occlusion rate of 75%. In our study, stent-assisted coil embolization of wide-necked intracranial aneurysms using the Acclino stents showed a complete occlusion rate of 94%.
A comparison of the different study populations showed that our study population had a similar aneurysmal distribution (65.1% anterior circulation; 34.9% posterior circulation) to the study populations of Möhlenbruch et al (LVIS Jr: 68.2% anterior circulation; 31.8% posterior circulation) and Fiorella et al (LVIS: 69% anterior circulation; 31% posterior circulation).19 ,21 In the study group of Aydin et al,13 aneurysms treated with the Leo baby stent were much more often located at the anterior circulation (90%). The mean aneurysm size of 7.7 mm×5.8 mm is similar to the sizes of the aneurysms treated using the LVIS and LVIS Jr stents, of 7.2 mm21 and 8.9 mm,20 respectively.
Acclino stents are characterized by a low thrombogenicity. Their laser-cut, electropolished surface promises a low rate of thromboembolic complications.22 Nevertheless, we performed stent-assisted endovascular techniques only if a good response to clopidogrel and ASA with values below the reference standards was ensured in the multiplate function test before all endovascular procedures. Kono et al23 reported that even triple antiplatelet therapy may not prevent thromboembolic events and highlighted the importance of a platelet function evaluation before employment of intracranial stents. We report only one case of procedural embolism managed with the administration of tirofiban. Postinterventional CT showed infarctions in the right anterior circulation and in the left posterior inferior cerebellar artery territory, presumably due to cardiac embolism. There was no further case of thromboembolism. One case of coiling-related thromboembolism was managed by stent placement, thus preserving the affected parent arteries. Aydin et al13 found a periprocedural or delayed thromboembolic event rate for the Leo baby stent of 7.5%. Behme et al14 reported asymptomatic thrombus formation in 2 of 34 cases treated with the LVIS Jr device (5.9%). This rate was comparable to the rates of periprocedural symptomatic thromboembolism—1.4% for the Neuroform and 8.7% for the Enterprise stent—noted by Kadkhodayan et al.24
Despite its retrospective design, the initial experience and results with the Acclino stents in our cohort of patients are promising. However, these findings have to be confirmed in future prospective studies.
Conclusion
Our results indicate that stent-assisted endovascular techniques with Acclino stents are a feasible treatment for complex intracranial aneurysms. Even in challenging complex bifurcation aneurysms we achieved good treatment results using the kissing-Y stenting technique.
References
Footnotes
FB and DG contributed equally.
Contributors FB: conceptualized the study; drafted the initial manuscript and revised it critically; and approved the final manuscript as submitted. DG: designed the study, analyzed and interpreted data for the work, drafted the manuscript; critically revised the manuscript; and approved the final manuscript as submitted. DM, MS-H: acquired, analyzed, and interpreted data for the work; critically revised the manuscript; and approved the final manuscript as submitted. BG: acquired data for the work; revised the manuscript; and approved the final manuscript as submitted. KM: acquired, analyzed, and interpreted data for the work; designed the study; drafted the manuscript; and approved the final manuscript as submitted. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Ethics approval Approval was obtained from our local hospital's institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors agree to share data on request.