Article Text

Abstract
Purpose The purpose of this pilot study was to demonstrate the applicability of time-resolved three-dimensional (3D) reconstructions from 3D digital subtraction angiography (DSA) rotational angiography (RA) datasets (four-dimensional (4D) DSA) to provide a more detailed display of the architecture of intracranial vascular malformations.
Methods The experimental reconstruction software was applied to the existing 3D DSA datasets obtained with Siemens Artis zee biplane neuroangiography equipment. We included 27 patients with clinical indications for 3DRA for preinterventional or preoperative evaluation of intracranial dural arteriovenous fistulas (dAVFs, n=8) or arteriovenous malformations (AVMs, n=19). A modified DSA acquisition protocol covering an extended rotation angle of the C-arm of 260° during a scan time of 12 s was used. 4D volumes were displayed with up to 30 frames/s in a transparent volume rendering (VRT) mode and time-resolved multiplanar reconstructions (MPRs). Arterial feeders, fistulous points, or the shunt zone within the AVM nidus and venous drainage patterns as well as associated aneurysms were assessed after definition of a standardized evaluation procedure by consensus of two reviewers in comparison with 2D DSA and conventional 3D reconstructions.
Results In all cases calculation of 4D reconstructions were technically feasible and evaluable. In two cases image quality was slightly compromised by movement artifacts. Compared with standard DSA projection images and 3D reconstructions, 4D VRTs and MPRs were rated significantly superior to define a proper projection and display of the shunt zone. In 12 out of 27 cases 4D reconstructions showed details of the angioarchitecture at the fistulous point or the nidus better than the other modalities and came close to the quality of superselective angiography. The efficacy of 3D and 4D applications was equal in the detection of pre- and intranidal aneurysms. The course of long arterial feeders and draining veins was difficult to assess on VRTs and MPRs. Especially for dAVFs, 2D DSA was clearly superior in identifying meningeal feeders. For detecting smaller vessels and for distinction between angiographic phases, 2D DSA is still considered to be superior to 4D imaging. Venous drainage was slightly better displayed in 4D reconstructions.
Conclusions Time-resolved 3DRA with 4D VRTs and MPRs is technically feasible and provides a detailed display of the angioarchitecture at the fistulous point or the nidus. Visualization of all angiographic features demands additional post-processing. Further standardization of evaluation tools and studies with blinded independent reviewers are necessary before the new technique can replace conventional neuroangiographic approaches.
- Arteriovenous Malformation
- Angiography
- Technique
- Vascular Malformation
Statistics from Altmetric.com
Introduction
High-resolution digital subtraction angiography (DSA) and three-dimensional (3D) rotational angiography (3DRA) are frequently used for angiographic evaluation of intracranial vascular malformations. However, details of the anatomy are frequently obscured by overlay of arteries and veins on projection images or by missing temporal information on static 3D reconstructions during a certain angiographic phase.1
Pre-therapeutic angiography of dural arteriovenous fistulas (dAVFs) or cerebral arteriovenous malformations (AVMs) frequently uses DSA series with high frame rates in multiple projections with the disadvantage of relatively high radiation doses.2 3D- and flat panel CT reconstructions are additionally used to provide more information about the site and extent of the shunt zone and to detect associated aneurysms.
In many instances these details are visualized by superselective angiography which is not part of a routine diagnostic angiogram and which has to be done in conjunction with embolization procedures, with the disadvantage of improper pre-therapeutic planning and rapid decision-making during the intervention.
The acquisition of 3DRA data within a certain scan time includes different angiographic phases and thus temporal information which can be used for calculation of time-resolved three-dimensional (4D) reconstructions. The main idea of 4D angiography is to provide multiple 3D volumes representing contrast dynamics at any point during scan time with the possibility to analyze the volumetric angiogram in multiple projections or multiplanar reconstructions (MPRs) in different phases with only one injection and acquisition.
The technical feasibility of 4D angiography has been reported in single cases or small case series.3–7 In particular, the 3D analysis of intracranial arteriovenous (AV) shunts could benefit from further dynamic information.4
Beyond findings like the presence of an AV shunt or associated aneurysms, we found it worthwhile to investigate whether 4D reconstructions provide more details about the transition zone between arteries and veins at the nidus or fistulous point as the main target of AVM or AVF treatment.
For detailed analysis of the microstructure a standardized approach for post-processing of 3D and 4D datasets was developed and compared between the two modalities and with diagnostic 2D DSA.
We rated the display of angioarchitectural features with the aim to find out whether 4D DSA alone is sufficient to determine arterial feeders and potential endovascular access routes, to distinguish associated pre- and intranidal aneurysms from vessel loops and venous pouches, and to assess venous drainage.
Like a recent study, which reported a potential reduction of radiation dose by replacing multiple 2D DSA series and 3D DSA by only one 4D run,4 it was also the purpose of our study to get first information about the feasibility in patients with pathological vasculature.
Dedicated analysis of effective patient dose was not part of this study. Referring to literature and experiences so far, an increase in dose of approximately 20% is expected compared with standard 3D DSA imaging. Considering the fact that during a conventional neurointervention 3D image acquisitions only add minor fraction of dose exposure, this increase is acceptable when weighed against the expected potential reduction in exposure from 2D acquisitions.
Methods
Patients
We included the data of 27 consecutive patients (20 men) of mean age 46 years (range 15–79 years) with clinical indications for 3DRA for pre-therapeutic evaluation of intracranial dAVF in 8 patients and an intracranial AVM in 19 patients. Patients' characteristics, clinical findings, and a brief description of the vascular malformations are provided in table 1.
Patient characteristics and type of cerebral malformation and short description of the procedure (ITN/superselective catheterization)
Methodology
2D, 3D, and 4D DSA images were obtained using a commercially available biplane angiographic system (Artis zee biplane; Siemens Healthcare GmbH, Erlangen, Germany). The experimental reconstruction software (Siemens Healthcare GmbH, Erlangen, Germany) for reconstructing time-resolved 3D images was applied to existing 3DRA (3D DSA) datasets.
Imaging acquisition
2D DSA images with a variable frame rate up to 4 frames/s were acquired in standard anteroposterior and lateral projections after hand injection of non-ionic contrast agent (Ultravist 240; Bayer-Schering, Berlin, Germany).
For 3DRA acquisition a modified protocol with an extended rotation angle of the C-arm of 260° during a scan time of 12 s with 30 frames/s was used. DSA images were obtained after a mask run and automatic injection of 21 mL of non-ionic contrast (Ultravist 300; Bayer-Schering) with a power injector at a flow rate of 3 mL/s. C-arm rotation was started with X-ray delay of 0.5 s after injection of the contrast agent.
Image reconstruction
3DRA data were transferred to a dedicated research workstation (syngo X Workplace, Siemens Healthcare GmbH, Erlangen, Germany) on which the 4D software prototype was installed. Digital subtraction was used for calculation of 3D and 4D volume rendering reconstructions (VRT) and multiplanar reconstructions (MPR) using the same algorithms and HU kernels (‘Unshaded’ for VRT and minimum intensity projection (MIP) MPRs).
The 4D DSA reconstructions were performed at the research workstation using a two-step process that has been reported in previous studies.3 ,4 A conventional 3D DSA volume was reconstructed by using a reconstruction algorithm as implemented in the product and the same reconstruction parameters used for standard 3D DSA scans described above. In a next step, the temporal information contained in the rotational projection sequence was encoded into the constraint volume for every projection image,3 ,4 resulting in a temporal volumetric representation of the contrast flow through the subject's vasculature at the frame rate of the rotational projection image acquisition (up to 30 frames/s).3 ,4 Time-resolved analysis of the whole volume or of cross-sectional views with slice thicknesses between 3 and 28 mm used VRT image representation with a pre-specified display in an unshaded mode. After reconstruction of the 3D and 4D volume, a proper ‘working projection’ for optimal display of the fistulous point or AVM nidus was selected to minimize overlay by adjacent vessels. MPRs with variable slice thickness parallel to the working projection further reduced complexity. Time-resolved or video analysis of 4D data helped to define the proper angiographic phase for optimal display of the AV shunt zone. Finally, we tried to follow arterial feeders and draining veins on VRTs or MPRs.
Figure 1 shows the evaluation procedure with an example of a 4D dataset of a patient with an AVM of the right temporal lobe.

(A) Time-resolved volume rendering reconstructions (anteroposterior projection) of an arteriovenous malformation (AVM) in the right posterior Sylvian fissure in the early arterial, later arterial, and venous phase with increasing filling of dilated draining veins. (B) Lateral view in the arterial phase demonstrates early venous drainage into superficial cerebral veins. Details of the angioarchitecture are not displayed in the standard projections. (C) Oblique caudo-cranial ‘working projection’ helps to select a proper angiographic phase to distinguish a middle cerebral artery branch as the main arterial feeder (red dotted line) from a parallel draining vein (blue dotted line). (D) A cut with variable slice thickness parallel to the working projection shows the terminal branches of the main feeding artery with several fistulas to the draining vein without overlay by adjacent vessels. (E) Slightly increased slice thickness includes the main arterial feeder and the proximal segment of the main draining vein. (F) In the later venous phase the two anterior and posterior (light blue line) draining veins can be separated from the fistulous nidus and the feeding arteries.
Image analysis
Feeding arteries, fistulous point or nidus, the presence of associated aneurysms, and the venous drainage pattern were determined by consensus of two experienced neuroradiologists who compared 4D DSA reconstructions with 3D volumes and 2D DSA projection images. The analysis was focused on the potential of 4D datasets to include all information derived from DSA and conventional 3D reconstructions. The angioarchitecture at the fistulous point or within the AVM nidus was the main target of our investigations to determine whether careful evaluation of 4D data could provide information similar to superselective angiography.
The quality of visualization of angioarchitectural findings was rated using the following categories:
+++, good visualization; ++, moderate, just adequate visualization; +, poor visualization. Further, a 4-point scale from 0 (not applicable) to 3 (good visualization) analogous to the above-mentioned rating was used to calculate the median of the vessels' visibility for each category. The non-parametric Mann-Whitney U test was applied for statistical analysis. A p value of <0.05 was considered to be statistically significant.
Further, the raters analyzed the images for special findings like pre- or intranidal aneurysms and impairment of venous drainage in AVM cases or reflux into cortical veins in patients with dAVF.
Results
Overall findings
In all selected cases calculation of 4D DSA datasets was technically feasible and evaluable. 4D DSA provided sufficient anatomical information in all patients. The image quality was slightly compromised in only two of the 27 cases imaged under local anesthesia. In comparison with DSA projection images, 3D and 4D reconstructions helped to define a proper projection of the shunt zone without overlay by adjacent vessels. Display of arterial feeders and draining veins was not rated to be significantly different among the three imaging modalities.
Concerning the shunt zone at the fistulous points of a dAVF or the nidus of an AVM, 4D reconstructions were rated superior to 2D DSA and 3D reconstruction. The difference was statistically significant (p<0.05).
Analysis of dAVFs
Due to incomplete display on VRT reconstructions and MPRs, the course of small meningeal feeders of dAVFs was difficult to determine on 3D and 4D datasets. 2D DSA was the best image modality for this purpose. 3D and 4D was not found to be advantageous in this regard (Figure 2).

(A–G) Comparison of different angiographic modalities in a patient with a posterior fossa dural arteriovenous fistula (dAVF) with cortical venous drainage. Meningeal feeder (yellow arrows), fistulous point (red arrow), and main draining vein are displayed. (A, C) Digital subtraction angiography (DSA) was superior to 3D and 4D applications to identify the feeding meningeal artery originating from the external occipital artery. (B, D, E) Volume rendering reconstructions and multiplanar reconstructions (MPRs) from 3D and 4D data could not demonstrate the whole course of the meningeal feeder. The display was dependent from the projection plane. (F) Superselective DSA demonstrates best the angioarchitecture at the fistulous point with the transition between the arterial network and the main draining vein prior to embolization. (G) MPRs from a 4D dataset came close to superselective angiography, with some limitations of the resolution within the arterial network.
However, the display of venous drainage benefited slightly from 4D analysis. In two out of eight dAVF cases, reflux into cortical veins was detected more easily on 4D reconstructions. In one of these cases 4D influenced the grading of the fistula. A cross-sectional view of time-resolved MPRs demonstrated the transition between arteries and veins at the fistulous points with sufficient quality to define the target for endovascular or surgical treatment. Due to less overlay by selection of the proper angiographic phase, 4D MPRs were found to be slightly superior to 3D reconstructions. Despite slight limitations due to an isotropic voxel size of ∼0.5 mm which appears not sufficient for visualizing smaller vessels and despite difficulties with window setting, thin 4D MPR slices came close to superselective angiograms (Figure 2) regarding diagnostic significance. In one out of eight patients 3D reconstructions were superior to 4D due to movement artifacts.
Analysis of AVMs
Regarding the distinction of the shunt zone within the nidus, the rating of 4D DSA in AVM cases was good in eight and moderate in nine of 19 cases. In one patient with a recent intranidal thrombosis, no AV shunt could be detected. Thus, visualization of the main feature of the nidal angioarchitecture was adequate or good in most of the patients. Despite multiple projections, comparative analysis of 2D DSA showed a higher number of seven poor visualizations of the nidus which decreased to three with the additional use of 3D reconstructions. In smaller and less complex AVMs in particular, visualization of the nidal angioarchitecture with 4D DSA was similar to superselective angiograms (Figure 3). In larger or more complex lesions with several feeders and draining veins it was more difficult to visualize the transition between arteries and veins (Figure 4). In three AVM cases it was also difficult to distinguish feeding arteries from draining veins in the area surrounding the nidus (Figure 4). 3D and 4D data were advantageous compared with DSA in identifying the course of arterial feeders. However, reconstructions showing the course of longer or tortuous feeders were time-consuming as additional effort for window setting was needed. In three of 19 patients with AVMs, pre- or intranidal aneurysms were detected. Compared with 2D DSA and VRTs from 3D datasets, cross-sectional MPRs through the nidus and the perinidal vessels were clearly superior. Volumetric time-resolved imaging only was not sufficient to separate associated aneurysms from overlaying structures (Figure 4). In two cases 3D and 4D reconstructions could clearly distinguish loops of feeding arteries from associated aneurysms.
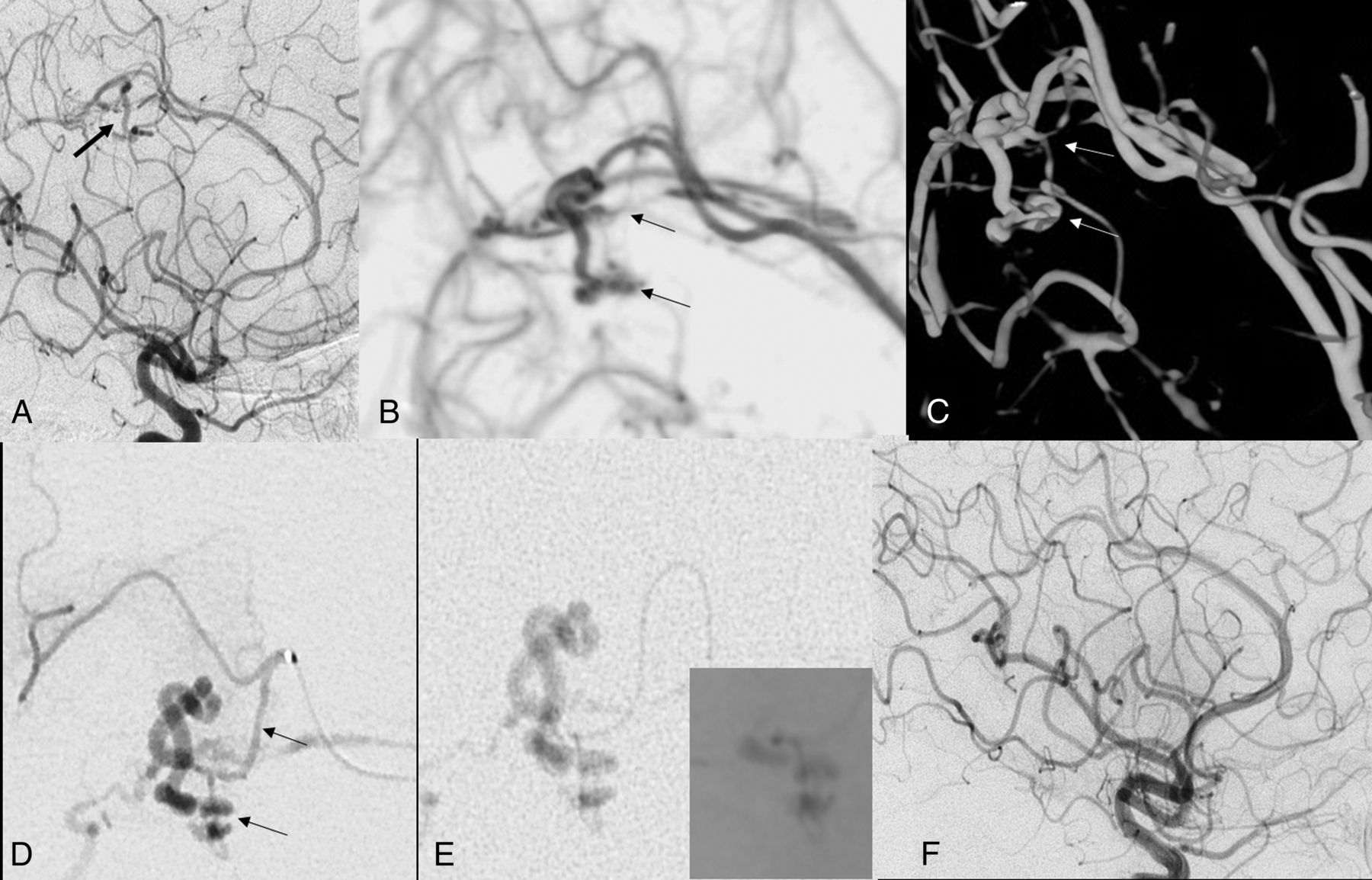
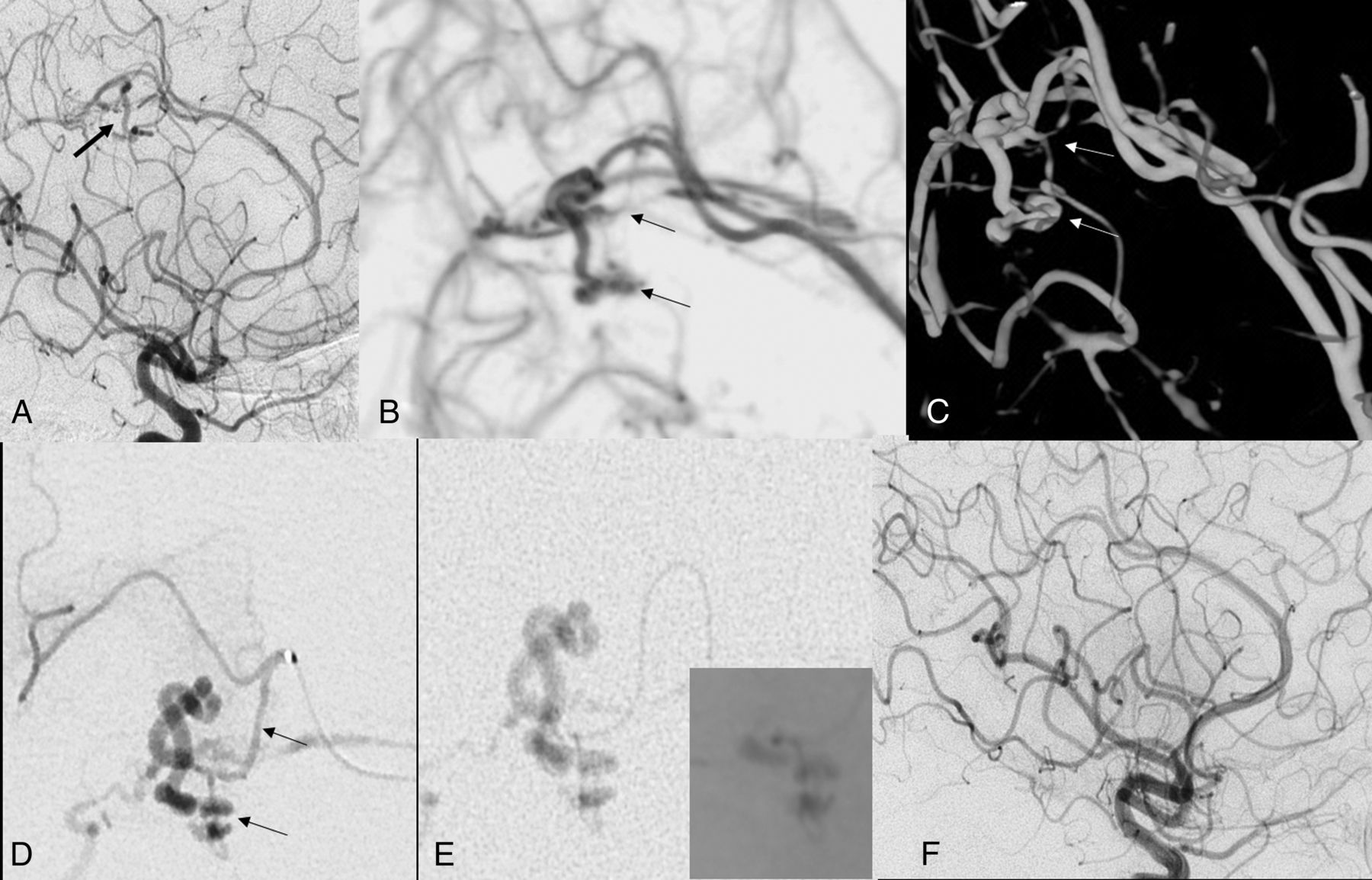
(A) Selective digital subtraction angiogram of a patient with intraventricular hemorrhage: proof of an arteriovenous shunt with early draining vein in the territory of the pericallosal artery (arrow). (B) A parasagittal cut of a 4D minimum intensity projection (MIP) reconstruction in the late arterial phase demonstrates the small feeding artery and the fistulous nidus (small arrows). An acute curve of the small feeding artery can be distinguished from a prenidal aneurysm (upper arrow). (C) Arterial feeder and fistulous point can also be shown on a volume rendering reconstruction (white arrows). (D) Superselective angiogram confirms the 4D findings (arrow). (E) Advancement of the microcatheter to the fistulous point and embolization with Onyx cast in the right lower quadrant. (F) Complete obliteration of the pial microfistula.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
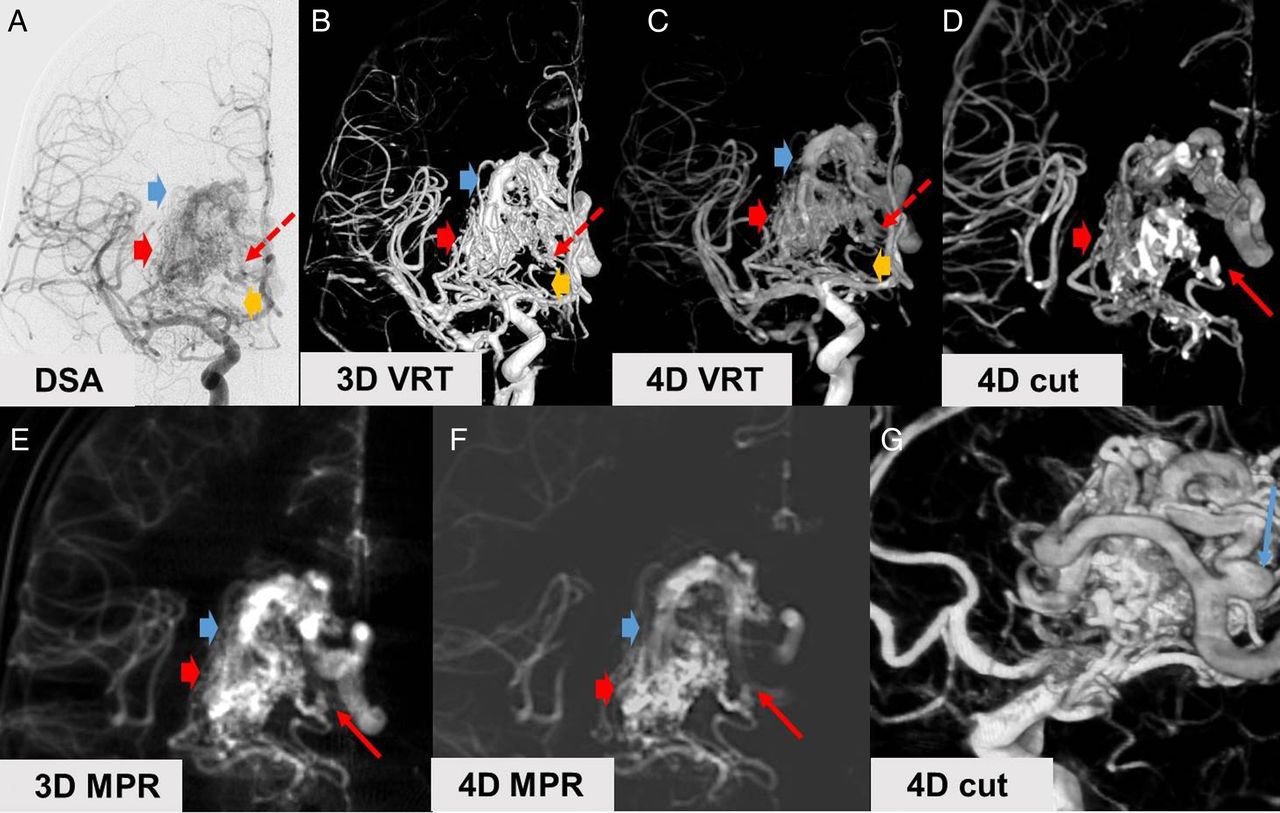
(A–G) Comparison of different angiographic modalities in a patient with a ruptured arteriovenous malformation (AVM) in the right basal ganglia. Arterial feeders from ascending anterior cerebral artery and middle cerebral artery perforators (yellow arrows), the shunt zone within the nidus (bright red arrows) and draining veins (bright blue arrows) can be distinguished on projection images, 3D and 4D volume rendering reconstructions (VRT) and multiplanar reconstructions (MPR). Note the small prenidal aneurysm (small red arrow) and varicose enlargement of one of the draining veins (small blue arrow). (A–C) Overlay of nidus, draining veins and associated aneurysm on digital subtraction angiography, 3D and 4D reconstructions of the whole volume. (D, E) Cuts from a 4D VRT and MPRs from a 3D dataset show the aneurysm more clearly. (F) The angioarchitecture of the nidus with multiple fistulous connections between arteries and draining veins converging to one of the main draining veins is best shown on 4D MPRs in earlier angiographic phases. (G) 4D also enhances the display of the veins in later phases of the angiogram.
The origin and course of draining veins was best visualized on 4D datasets. Venous aneurysms could be detected in three patients. We found two cases of venous stenosis. Impairment of venous drainage (probably due to thrombosis) in two patients with a recently ruptured AVM was best seen on DSA images.
Tables 2 and 3 show the results of the analysis of the microvascular findings with 2D, 3D, and 4D DSA in patients with dAVFs and AVMs. Additionally, the median for each category was calculated using a 4-point scale.
Analysis of microvascular findings between 2D DSA, 3D DSA and 4D DSA in patients with AVFs
Analysis of microvascular findings between 2D DSA, 3D DSA and 4D DSA in patients with AVMs
Discussion
In all cases calculation of 4D reconstructions was technically feasible and evaluable. Time-resolved 3D imaging provided equivalent or even more information than 2D DSA and 3D DSA scans in all patients. Our assessment of the diagnostic potential of 4D DSA reconstructions shows that visualization of the angioarchitecture at the fistulous points of dAVFs or at the shunt zone of an AVM nidus was at least equal to or superior to conventional angiographic imaging with DSA or 3DRA. Pre- and intranidal aneurysms could be detected reliably. 4D reconstructions were also valuable for the assessment of venous drainage. The superiority of 4D DSA could not be shown for small meningeal feeders of dAVF.
Our findings confirmed previous studies concerning the technical feasibility of 4D DSA, with the ability to create a series of time-resolved volumes of vasculature so that the passage of a contrast bolus may be viewed in 3D at any time and from any angle.3–7 In traditional 3D DSA, acquisitions overlap of vasculature can make it difficult to analyze details of the angioarchitecture of an AVM such as the nidus, associated aneurysms, venous stenosis, and drainage.4 Compared with time-resolved MR or CT angiography techniques, spatial resolution of 4D reconstructions is higher and allows viewing of an AVM from any angle at any time during its opacification.4 Previous authors have stated that, with the use of 4D DSA, the ability to view the relevant vasculature during the passage of the contrast agent in different angulations and at any time should result in less need to acquire multiple 2D series in both diagnostic and interventional procedures, thereby leading to reductions in both X-ray and contrast medium dose.2 ,4 The results of our assessment showed significantly better ratings of 4D visualization of the fistulous point or nidus. Because of the rapid filling and vascular overlap, 2D DSA is often suboptimal for evaluation of angioarchitectural features in AV shunts.4 Similarly, as static 3D reconstructions do not include any temporal information and comprise all vascular structures opacified during a certain acquisition phase, vascular structures that are adjacent to one another are often obscured by superimposition.4 The hypothesis that time-resolved 3D angiography could reduce 3D DSA and multiple 2D DSA image acquisitions to a single 4D acquisition4 is partially supported by our results.
Visualization of the micro-angioarchitecture at the level of AV shunts with 4D is superior as vessel loops could easily be distinguished from aneurysms and determination of the morphology, caliber, and number of fistulous connections is similar to superselective angiograms (Figure 3). We also found a trend towards better visualization of venous drainage on 4D reconstructions. The display of the origin and course of draining veins close to the nidus especially benefitted from temporal resolution.
For detecting smaller vessels such as meningeal feeders of dAVFs accessible for endovascular embolization, 2D DSA was superior to 4D imaging. With 4D reconstructions we experienced difficulties in following long arterial feeders or feeders of small caliber, and in distinguishing arteries from veins. 2D DSA provided valuable complementary time-resolved information in these cases and cannot be replaced by a single 4D dataset. However, 4D DSA may replace additional DSA series in oblique projections or with frame rates of >4 frames/s.
In our experience a detailed display of smaller vessels, the fistulous point or the angioma nidus was best with cross-sectional VRT views. Temporal resolution and restriction to cross-sectional views with variable slice thickness were the main tools used to avoid overlapping by adjacent vessels or overlapping of arteries and veins caused by using a dedicated injection protocol with 7 s bolus time. The shortcoming of overlapping angiographic phases is counterbalanced by the possibility to obtain multiple reconstructions and video analysis of hemodynamics.
Future studies with new protocols and omission of DSA series in multiple projections will show whether 4D DSA contributes to dose reduction in diagnostic neuroangiographic procedures of patients with intracranial vascular malformations. Better treatment planning after evaluation of 4D data may also result in fewer superselective catheterizations and DSA series during an intervention. First comparisons with superselective angiograms show a good agreement between 4D MPRs and superselective DSA projection images.
A prerequisite to avoid multiple or superselective angiograms has been a time-consuming analysis of a 4D dataset. With our process we tried to find a way towards a standardized approach to reduce complexity. Further prospective studies need to show that meticulous pre-interventional planning really reduces X-ray exposure before and during interventional procedures received from multiple DSA acquisitions. We also need to show that such detailed analysis provides a major contribution for better understanding of the angioarchitecture at the AV shunt zone, with the aim of increasing the safety and efficacy of AVM embolizations, surgery, or radiosurgical treatment.
Study limitations
Although time-resolved display of conventional 3DRA datasets was technically feasible in all cases, there is still some room for improvement of the new method.
The added clinical benefit provided by 4D DSA reconstructions for diagnosis and treatment planning, however, requires additional effort and experience for windowing of VRT representations and working out angioarchitectural details which demands a change of diagnostic habits. Instead of multiple 2D DSA views, we have to spend more time on the reconstruction and evaluation of a single dataset, similar to neurosurgical planning, with the assistance of navigation software. Standardization of window settings is necessary to facilitate the clinical use of 4D angiography. Making this easier for the user should certainly be an aim for future software versions.
Overlapping of arterial and venous phases has already been mentioned as one of the drawbacks of the new technique. In our study the time frame is limited by a maximal acquisition time of 12 s. A sharper and shorter bolus geometry was discussed but may result in a slightly inaccurate 3D representation of the vasculature. However, further analysis will help to define optimal injection protocols for small and large vessels and for fast and slow flow.
Patient movement and streak artifacts known in 2D DSA and 3D DSA have also been monitored in 4D DSA. As in 2D and 3D DSA, movement and streak artifacts can limit image quality. Regarding the display of smaller vessels such as perforators, the image impression can be noisier to some extent and smoothed in MPR/MIP reconstructions compared with 3D DSA reconstructions. In some cases, a misleading opacification of the jugular vein was obvious in the very early arterial phases which could potentially result in misinterpretation of a pathological venous contamination if no other imaging data are considered.
Further, we have to mention that the image analysis was performed with the consensus of both readers. Despite our efforts to get maximal information from all angiographic modalities, we might have been biased towards the new technology. At the current stage of development, independent reviewers need a profound understanding of intracranial AV shunts and would have to absolve a considerable learning curve to retrieve the information from 3D and even more complex 4D reconstructions.
Conclusion
4D DSA is a promising new tool to improve detailed angiographic analysis of the angioarchitecture of the shunt zone of intracranial dAVFs and AVMs. The method has the potential to improve pre-therapeutic planning and to avoid DSA series in multiple projections or superselective catheterization. Optimization of injection protocols, better standardization of time-consuming reconstructions, and studies with independent reviewers are needed for further evaluation of time-resolved 3D angiography.
Footnotes
Contributors SL: concept, design, data analysis and interpretation, manuscript writing and preparation. JB: concept, data interpretation, critical review of manuscript. SG and SK: concept, critical review of manuscript.
Disclaimer The experimental software presented in this paper is based on research and is not commercially available. Due to regulatory reasons its future availability cannot be guaranteed.
Competing interests JB: Consulting fee or honorarium: proctor for WEB, Sequent Medical and member of the scientific advisory board of Acandis. JB and SL: The project is part of a permanent scientific cooperation between Siemens and the Institute of Neuroradiology at the University Frankfurt, Germany, and travel expenses for presentation of the project are covered by Siemens. Our institution will receive an honorarium related to the publication of the study from Siemens. SG and SK: employees of Siemens Healthcare GmbH, BU Advanced Therapies, Forchheim, Germany.
Ethics approval Ethics approval was obtained from the local ethics committee of the University Hospital Frankfurt.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are included in the study.