Article Text

Abstract
Background The recanalization of cerebral aneurysms after endovascular embolization (coiling or stent-assisted coiling) has been a matter of concern.
Objective To systematically evaluate the predisposing factors for cerebral aneurysm recanalization using multidimensional analysis in a large patient cohort.
Methods In 238 patients with 283 aneurysms, patient baseline characteristics, aneurysm morphological characteristics, treatment-related factors, and changes in flow hemodynamics after endovascular treatment (coiling or stent-assisted coiling) were compared between the recanalization and non-recanalization groups. Multivariate logistic regression analysis was performed to determine independent risk factors correlated with recanalization.
Results 16 aneurysms treated by coiling recanalized, with a recurrence rate of 18.6%, and 24 recanalized in the lesions treated by stent-assisted coiling, with a recanalization rate of 12.2%. Large aneurysms (>10 mm, p=0.002) and a follow-up interval >1 year (p=0.027) were shown to be statistically significant between the recanalization and non-recanalization groups. For flow hemodynamic changes, three parameters (velocity on the neck plane, wall shear stress on the neck wall, and wall shear stress on the whole aneurysm) showed a relatively lower amplitude of decrease after endovascular treatment in the recanalization group. Interestingly, the velocity on the neck plane and wall shear stress on the neck wall may be elevated after treatment. Specifically, the reduction ratio (RR) of velocity on the neck plane showed significant difference between the groups in the multivariate analysis (p=0.013), and was considered an independent risk factor for recanalization.
Conclusions The aneurysm size, follow-up interval, and flow hemodynamic changes, especially the RR of velocity on the neck plane, have important roles in aneurysm recanalization.
- Aneurysm
- Blood Flow
Statistics from Altmetric.com
Introduction
Endovascular therapy is now the first-line treatment for the majority of cerebral aneurysms.1 However, aneurysm treatment after endovascular embolization has a higher frequency of recanalization than surgical clipping, ranging from 6.1% to 33.6%.2 Given the risk of recanalization, assessment of aneurysm recurrence is critical following endovascular treatment. Several risk factors have been proposed to explain aneurysm recurrence, including aneurysm morphological features, coil compaction and/or migration, and different types of endovascular embolization techniques.2 ,3 Studies using computational fluid dynamics (CFD) have also suggested that cerebral hemodynamics have a key role in aneurysm recurrence.4–6 However, these previous reports based on CFD were mainly performed in a relatively small number of specific cases (eg, <10 cases) or in a subset of patients, which challenges the representativeness of the hemodynamic findings.
Thus, the aim of our study was to systematically develop a comprehensive assessment of the predisposing factors for aneurysm recurrence. For 283 consecutive aneurysms treated with endovascular embolization (coiling or stent-assisted coiling) in our institution, we performed a multivariate analysis including patient baseline characteristics, aneurysm morphological characteristics, treatment-related factors, and changes in aneurysmal hemodynamics to determine the independent risk factors of recanalization. To our knowledge, this is the first multidimensional report with hemodynamic analysis in such a large patient cohort.
Patients and methods
Patient selection
This study was conducted with the approval of our institution, and the ethics committee of our hospital approved the study protocol. We retrospectively reviewed the clinical and radiologic data of patients who underwent endovascular embolization between January 2012 and December 2014. Patient data with available angiographic follow-up that was performed at least 3 months after the initial treatment were reviewed centrally by two experienced neuroradiologists, independent of the study, to determine whether the aneurysm had recanalized. The angiographic results of aneurysm embolization were quantified according to the Raymond–Roy classification system:7 class 1: complete obliteration, no filling of the aneurysm neck or dome; class 2: a residual neck, the persistence of any filling of the neck but not the dome; class 3: a residual aneurysm, any opacification of the aneurysm sac. At follow-up, an aneurysm was considered recanalized if any further filling of the aneurysm neck or sac was observed compared with the initial treatment findings.2 Patients with dissecting and fusiform aneurysms and those who had insufficient three-dimensional digital subtraction angiography data were excluded from this cohort. For the purpose of this study, a total of 238 patients (283 aneurysms) with available medical and angiographic data, who were treated by coiling or stent-assisted coiling, were included in our research. All data were acquired for diagnostic purposes and computation of hemodynamics, and informed consent was obtained from each study patient or their closest relatives.
Demographic and clinical data
The following data were extracted from case record forms: patient baseline characteristics, including patient age and gender, smoking, drinking, and hypertension; aneurysm morphological characteristics, including large aneurysm (>10 mm),8 ,9 wide-neck aneurysm (>4 mm),8 ,9 aneurysm status when receiving treatment (ruptured/unruptured), aneurysm locations, and aneurysm geometry (sidewall/bifurcation)—aneurysm locations were categorized as anterior circulation (anterior cerebral artery, middle cerebral artery, internal carotid artery) and posterior circulation (basilar artery, vertebral artery, posterior cerebral artery); treatment-related factors, including initial angiographic result after treatment, stent-assisted, type of packing density (≤24% or >24%),10 ,11 follow-up interval (≤1 year or >1 year); information about placement of the stent when the aneurysm was wide neck and/or the dome-to-neck ratio was <2; and the packing density, calculated as the ratio of coil volume and aneurysm volume multiplied by 100% (see online supplementary file).
supplementary file
Computational modeling and hemodynamic simulations
Patient-specific aneurysm morphologies were reconstructed from three-dimensional rotational angiography images. To calculate the hemodynamics of the aneurysms, we applied our previously developed computational modeling methods.12 A novel virtual stenting technique13 ,14 and a porous media method12 were used to simulate the in vivo Enterprise stent and coil mass, respectively. Hemodynamics parameters based on CFD were performed under pulsatile flow conditions using commercial software (ANSYS CFX 14.0; ANSYS, Inc, Canonsburg, Pennsylvania, USA). The computational results at the aneurysmal neck and the whole aneurysm were examined accurately. For observation of hemodynamic variables, we extracted the average flow velocity and average wall shear stress (WSS) at both pre- and post-endovascular embolization at peak systole. The hemodynamic reduction ratio (RR), defined as (pretreatment parameter−post-treatment parameter)/pretreatment parameter, was calculated for each patient-specific aneurysm. The following hemodynamic changes were examined: the RR of velocity on the neck plane and inside the aneurysm, and the RR of WSS on the neck wall and the whole aneurysm wall (see online supplementary file).
Statistical analysis
Analysis was performed with statistical software (SPSS V.19.0; IBM, Chicago, Illinois, USA). For continuous variables, the one-sample Kolmogorov–Smirnov test was used to test the normal distribution, followed by an independent-samples t-test for approximately normally distributed data. The Mann–Whitney U test was used to compare non-parametric data, while the χ2 test was used for categorical variables. Data are presented as frequencies (percentages) for categorical variables and mean±SD or median (IQR) for continuous variables. Risk factors with a p value <0.1 in univariate analysis were entered into a multivariate logistic regression analysis to assess the independent risk factors of recanalization. The OR with 95% CIs was calculated between the recanalization group and non-recanalization group. A two-tailed p value <0.05was considered statistically significant in the multivariate logistic regression.
Results
During the study period, 283 consecutive intracranial aneurysms (40 recanalization, 243 non-recanalization) treated by endovascular embolization (coiling or stent-assisted coiling) in our hospital were included in our study. Sixteen aneurysms treated by coiling recanalized, with a recurrence rate of 18.6%, and 24 recanalized in the lesions treated by stent-assisted coiling, with a recanalization rate of 12.2%. Univariate analysis of patient baseline characteristics, aneurysm morphological characteristics, treatment-related factors, and hemodynamic changes are shown in table 1. The results of multivariate logistic regression are presented in table 2.
Univariate analysis between recanalization and non-recanalization groups
Multivariate analysis between recanalization and non-recanalization groups
Patient baseline characteristics
There were 30% men in the recanalization group, and 27.2% men in the non-recanalization group. The mean patient age was 51.7 years in the recanalization group, and 53.6 years in the non-recanalization group. Univariate analysis showed no differences in any patient baseline characteristics between the two groups (table 1).
Aneurysm morphological characteristics
The mean aneurysm size was 10.1±6.1 mm in the recanalization group, with a mean neck width of 5.6±2.9 mm, and 6.8±4.3 mm in the non-recanalization group, with a mean neck width of 5.1±2.6 mm. Univariate analysis demonstrated a significantly higher proportion of large aneurysms in the recanalized group than in the non-recanalized group (16 (40%) vs 38 (15.6%), respectively; p<0.001, table 1). There was a non-significant trend towards recurrence of wide-neck aneurysms (p=0.075, table 1). Ten (25%) ruptured aneurysms were observed in the recanalization group, and 50 (20.6%) in the non-recanalization group, with no association with recanalization (p=0.526, table 1). There was also no association with recurrence for the factors of aneurysm location (anterior circulation, posterior circulation) and the type of aneurysm geometry (sidewall, bifurcation). For aneurysmal morphological characteristics, aneurysm size (>10 mm) was the only independent risk factor for recanalization (p<0.001, table 1; OR=4.63, 95% CI 1.76 to 12.2, p=0.002, table 2).
Treatment-related factors
No differences in the initial angiographic result were found between the recanalization and non-recanalization groups (p=0.114, table 1). A higher percentage of aneurysms treated only by coiling were seen in the recanalization group than in the non-recanalization group (40% vs 28.8%, respectively), though this was not significant (p=0.154, table 1). Lower packing density (23±7% vs 26±6%, respectively) and longer interval of follow-up (11.4±7.5 months vs 9.4±6.3 months, respectively) were seen in the recanalization group. However, there were no differences in the type of packing density (p=0.203, table 1), whereas the interval of follow-up >1 year remained significant in the multivariate logistic regression analysis (OR=2.51, 95% CI 1.11 to 5.66, p=0.027, table 2).
Hemodynamic changes
A lower amplitude reduction of the velocity on the neck plane was found in the recanalization group (figure 1A, C), resulting in a significantly lower median RR (19.5%) compared with the non-recanalization group (30.2%, p<0.001, table 1). By contrast, the RR of velocity inside the aneurysm was similar in the two groups. There were fewer streamlines inside the aneurysm caused by the inhibition of the stent and coils, indicating a marked decrease of velocity after treatment (figures 2D and 3D), and showing no difference, with a similar median value of RR in the recanalization and non-recanalization groups (71.7% vs 73.3%, respectively, p=0.869, table 1). As observed for changes of velocity on the neck plane, there was a lower amplitude reduction, or potentially an even larger amplitude increase of the WSS on the neck wall in the recanalization group (p<0.001, table 1). A larger area of elevated WSS may be seen on the circumference of the neck wall in the recanalization case (figure 2C). Additionally, a more marked decrease of WSS on the whole aneurysm wall between pre- and post-treatment can be observed in the non-recanalization case than in the recanalization one (figures 2C and 3C), which was also significantly different between the recanalization and non-recanalization groups (p=0.026, table 1). Of all the significant factors in univariate analysis, only the RR of velocity on the neck plane correlated significantly with recanalization in multivariate logistic regression analysis (p=0.013, table 2).
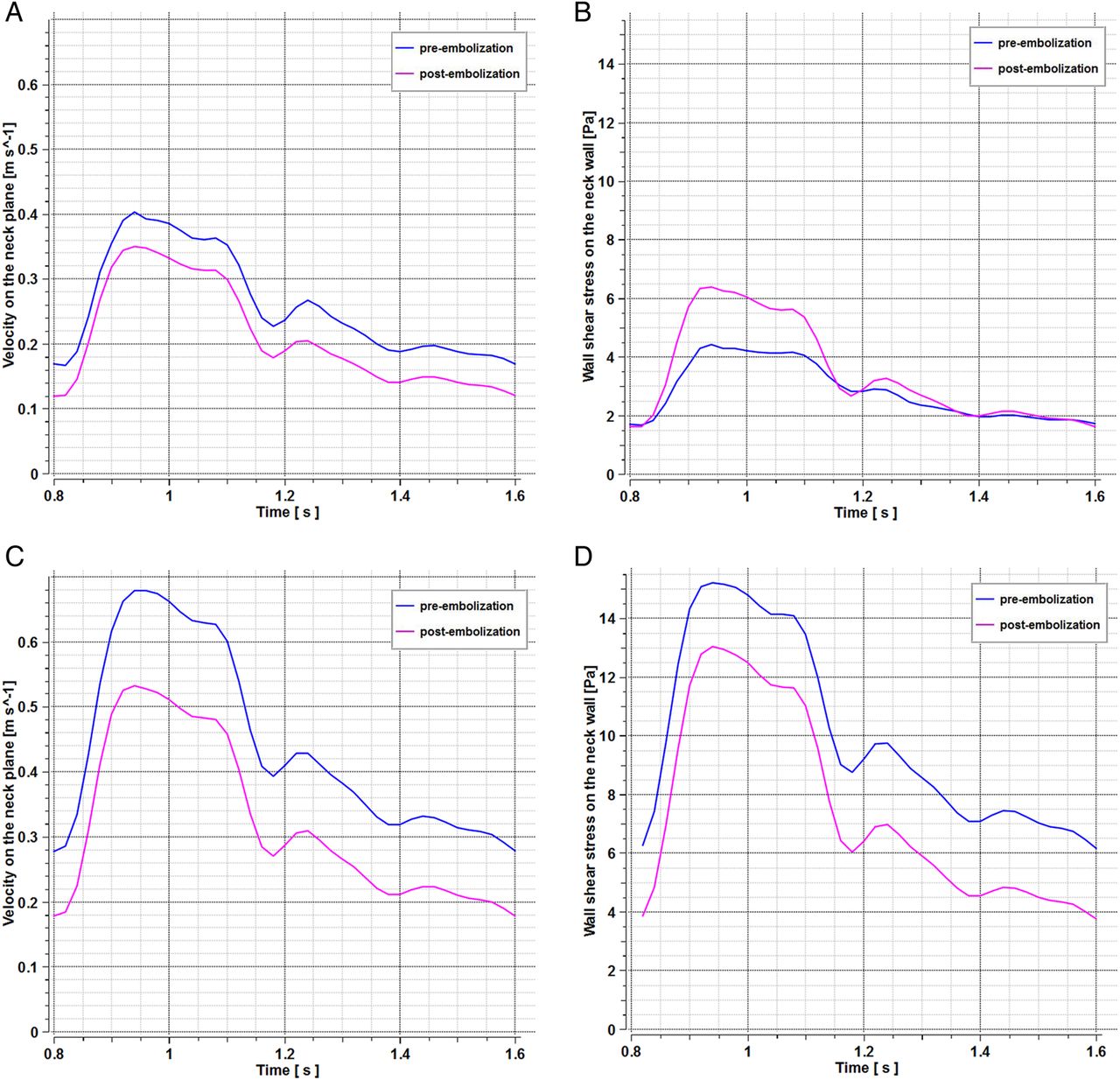
Representative velocity on the neck plane and wall shear stress (WSS) on the neck wall in a recanalization (A and B) and a non-recanalization (C and D) case. First column, velocity on the neck plane (A and C). Second column, WSS on the neck wall (B and D). After embolization, there was a lower amplitude reduction ratio of the velocity on the neck plane (A vs C) and obvious increases in WSS on the neck wall (B vs D) in the recanalization case.

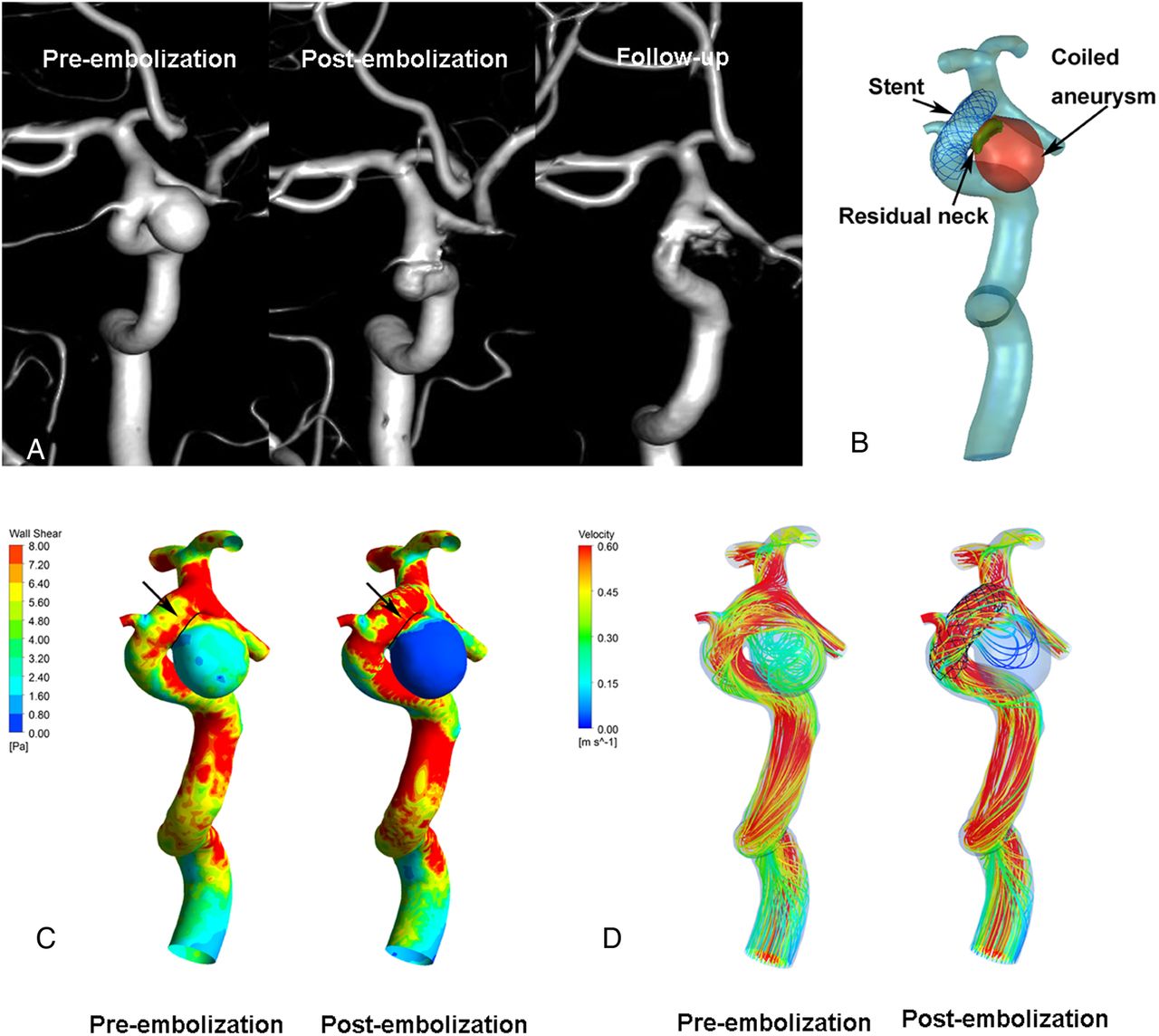
Illustrations of hemodynamics in a recanalized case, treated by stent-assisted coiling. (A) Angiographic images at pre-embolization (left), post-embolization (middle), and follow-up (right). (B) Reconstructed aneurysm model. (C) Wall shear stress (WSS) distribution at pre-embolization (left) and post-embolization (right). (D) Velocity streamlines at pre-embolization (left) and post-embolization (right). In illustration B, the green region (medium arrow) indicates the residual neck after endovascular treatment, the red region (large arrow) indicates the coiled aneurysm, and the stent (small arrow) was deployed. After embolization, the WSS on the whole aneurysm wall and the flow velocity inside the aneurysm were decreased (C and D). However, the WSS on the neck wall (circumference of the black lines) increased markedly (C, black arrows).

{kind=link}
{kind=link}
{kind=link}
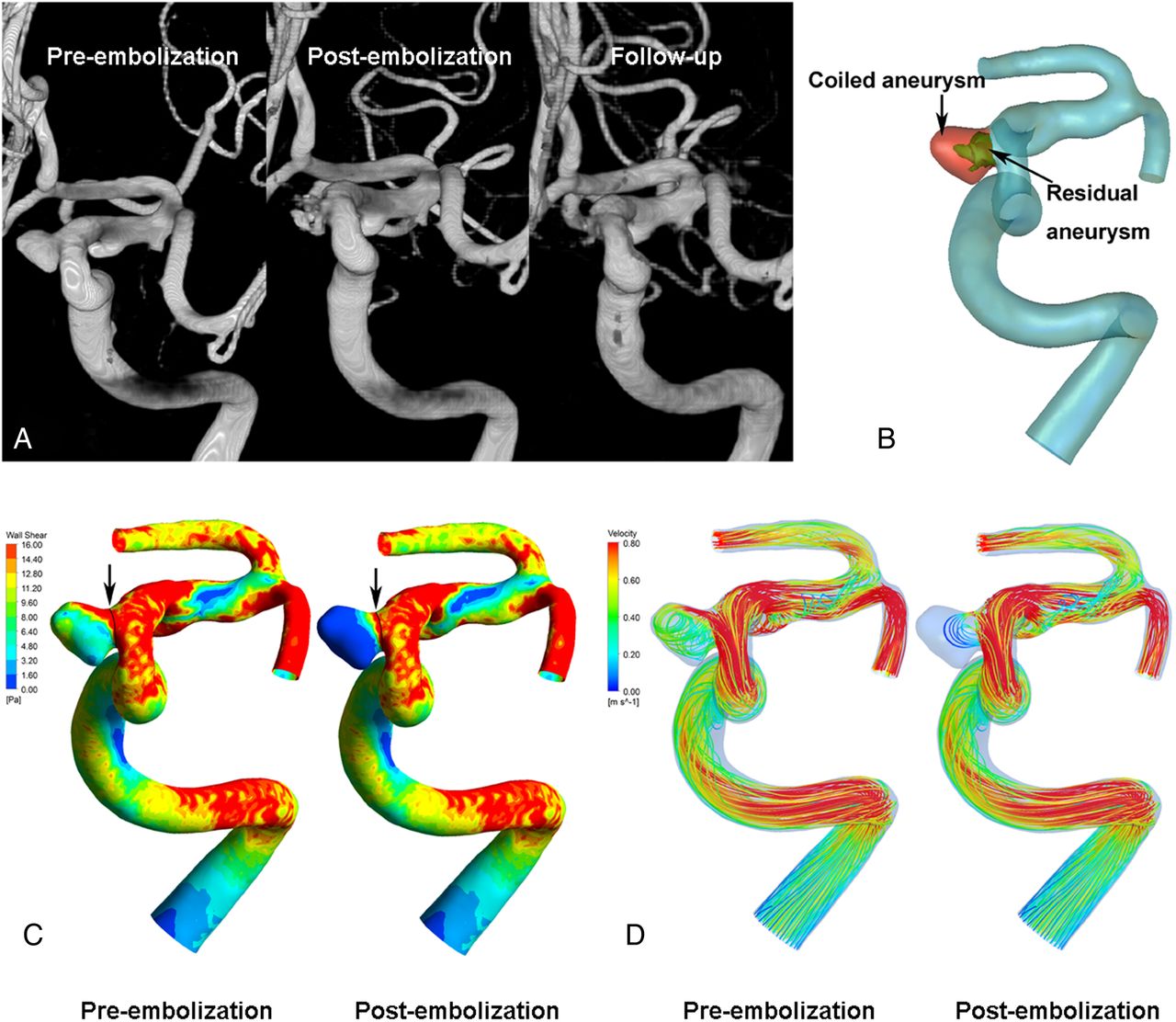
Illustrations of hemodynamics in a non-recanalized case, treated only by coiling. (A) Angiographic images at pre-embolization (left), post-embolization (middle), and follow-up (right). (B) Reconstructed aneurysm model. (C) Wall shear stress (WSS) distribution at pre-embolization (left) and post-embolization (right). (D) Velocity streamlines at pre-embolization (left) and post-embolization (right). In illustration B, the green region (large arrow) indicates the residual aneurysm after coil embolization, the red region (small arrow) indicates the coiled aneurysm. After embolization, the WSS on the whole aneurysm wall and the flow velocity inside the aneurysm were markedly decreased (C and D). In line with the changes of WSS on the whole aneurysm wall, the WSS on the neck wall (circumference of the black lines) decreased (C, black arrows).
Discussion
The durability of endovascular embolization (coiling or stent-assisted coiling) has been a major concern in the management of intracranial aneurysms. In this study, we performed an overall evaluation of the predisposing factors correlated with recanalization in a large series of patients. Our main findings were that aneurysm size (>10 mm), follow-up interval >1 year, and the RR of velocity on the neck plane were significant independent risk factors of aneurysm recurrence.
Aneurysm morphological characteristics
Aneurysm size was significantly associated with recanalization in our patients, as previously reported.2 ,15–17 What is more, we also found a 4.5-fold increase in the risk of recanalization with an aneurysm size >10 mm, similar to that reported in a systematic review and meta-analysis.17 It is possible that large aneurysms may be more susceptible to coil compaction/migration and/or coil loosening, attributed to the lower packing densities and resulting contrast filling within the aneurysmal neck or sac.11 ,18 The precise mechanisms leading to coil changes (coil compaction, coil migration, coil loosening) remain unclear. Possibly, larger aneurysms may experience complex flow patterns caused by pulsatile flow, resulting in coil changes.11 ,19 Based on the analysis of aneurysm morphological characteristics, we suggest that attention should be paid to large aneurysms after endovascular treatment. The use of flow-diversion embolization devices, which have a high metal surface area coverage of the parent artery vessel, thus achieving aneurysm occlusion by marked reduction of flow velocity and endoluminal reconstruction of the parent artery,20 ,21 may be a viable alternative for improving the treatment of large aneurysms.
Treatment-related factors
Of the treatment-related factors, follow-up interval >1 year was an independent risk factor for recanalization. In clinical practice, the first follow-up is routinely performed at 6 months as an index of occlusion,3 ,22 while there is high interpersonal variability for follow-up beyond 6 months, with no safe time interval recommended.22 ,23 Nguyen et al16 reported follow-up strategies of 6 months, 1 year, and then every year until 5 years for ruptured aneurysms, and 1 month, 3 months, and then 5 years from initial coiling for unruptured aneurysms. Choi et al24 also suggested a first follow-up at approximately 6 months, and then annually for ≥4 years. However, in a series of 59 patients with coil embolization of 65 aneurysms, Tailor et al25 reported that most occluded aneurysms at 6 months remained stable at the 2-year follow-up, which questioned the need for imaging follow-up beyond 6 months. In contrast, our data suggest that a 6-month follow-up after embolization was insufficient for monitoring all recanalization, and that a further 6 months of rigorous imaging follow-up was required. In support, in a series of 501 aneurysms, Raymond et al reported that majority of recurrence occurred at a mean of 12.31 months after embolization.15 Although repeated follow-ups lead to additional expense for patients, our findings imply that patients should reasonably receive follow-up at 1 year after the initial treatment, in case in early diagnosis recanalization was missed.
Hemodynamic changes
The role of hemodynamics in aneurysm recurrence is widely reported.4–6 Many hemodynamic parameters have been proposed as potential indicators of aneurysm recurrence, of which velocity and WSS are considered the most important. In the largest population combined with CFD thus far, the most interesting finding in our current study was that the RR of velocity on the neck plane after embolization was a significant predictor of recanalization when controlling for other factors.
Unlike previous reports, we used the RR of velocity as a normalized parameter to limit potential differences between individuals, which allowed more accurate comparisons to be made. A relatively low-amplitude RR of velocity on the neck plane was seen in the recanalization group. Of note, there were negative values for RR of velocity on the neck plane in most cases in the recanalization group, indicating elevated velocity after embolization. The higher residual velocity on the neck plane would have profound influence on later recurrence. One possibility is that the higher the residual velocity on the neck plane, the higher the impingement on the coils inside the aneurysm, which induces the compaction of the coils and leads to recurrence. Another possibility is that the relatively fast blood flow may impair local blood coagulation and prevent thrombosis formation in the aneurysms.26 Finally, the higher residual velocity may interfere with neointima formation of the aneurysmal orifice, which is considered essential for complete healing of the embolized aneurysms.27
WSS, defined as the tangential drag force per unit area of the endothelial surface,21 is thought to play a significant role in recanalization. By constructing only one computational model of a curved artery, Feng et al28 proposed that high local WSS leads to degeneration of the arterial wall, and thus results in aneurysmal growth. Several later studies also reported that higher WSS promoted aneurysmal recanalization.4 ,5 ,26 In contrast, Brinjikji et al found that aneurysm recurrence was related to a higher percentage of abnormally low WSS, which may induce apoptosis of aneurysm endothelial cells.29 In our study, a relatively low amplitude RR of WSS, or elevated WSS after embolization, was observed in the recanalization group, which may be associated with recanalization but was marginally significant in the multivariate analysis. The precise mechanisms underlying the biological relationship between WSS and recanalization need to be further determined.
Limitations
This study has some potential limitations. First, we used simplified CFD analyses, including rigid walls, Newtonian blood properties, and physiological but not patient-specific flow-boundary conditions; however, these parameters were previously reported to be useful for understanding flow hemodynamics in aneurysms.30 Similarly, our computational modeling of the stents and coils did not fully reflect the actual situation of endovascular treatment. Additionally, genetic factors and histopathological mechanisms are also important for aneurysm recanalization. The association between these aspects and aneurysm recurrence should be examined more comprehensively in future studies. Finally, a flow diverter was not included in our study because it was approved for operational use by the China Food and Drug Administration relatively late in comparison with other countries. In addition, this was a retrospective single-center study, and future prospective, large multicenter studies are required for detailed analysis of recanalization.
Conclusion
Using multidimensional analysis in a large patient cohort, we demonstrated that aneurysm size (>10 mm), follow-up interval >1 year, and RR of velocity on the neck plane were significant predisposing factors for aneurysm recurrence. These findings may be applied to clinical post-embolization management for the evaluation of recanalization.
References
Footnotes
QZ and LJ contributed equally.
Contributors QZ and LJ contributed to the preparation of the manuscript and data collection. KW and JL contributed to revision of the the manuscript. YZ, NP, YW, and SW contributed to data analysis and interpretation. HM and XY contributed to the experimental design and manuscript revision.
Funding This work was supported by National Key Research and Development Plan of China (grant number: 2016YFC1300800), the National Natural Science Foundation of China (grant numbers: 81471167, 81671139, 81571128, and 81220108007), the Special Research Project for Capital Health Development (grant number: 2014-1-1071), and National Institutes of Health (R01 NS091075).
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by the ethics committee of Beijing Tiantan Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors agree to share any data on request. Any data from this study are available by contacting the corresponding author.