Article Text

Abstract
Background and purpose Thrombus composition has been postulated to affect the success of endovascular therapy. Calcified clots are composed of large amounts of calcium phosphate which influences their mechanical properties and may serve as a model for testing this hypothesis. The aim of this study was to evaluate the recanalization and complication rates of calcified thromboemboli in patients with acute ischemic stroke who underwent thrombectomy.
Material and methods A retrospective analysis was performed of all calcified intracranial thromboemboli in patients suffering an acute ischemic stroke, referred for endovascular therapy at two centers between January 2013 and July 2016.
Results Eight patients with a calcified intracranial clot underwent stent retriever thrombectomy (five women; mean age 80 years). Mean clot attenuation was 305 HU (range 150–640 HU). Successful reperfusion defined, as Thrombolysis in Cerebral Infarction grade 2b–3 was achieved in only one patient (12.5%). Two periprocedural adverse events occurred: one peripheral vessel perforation which was coiled and one inadvertent stent retriever detachment due to fracture of the stent retriever wire.
Conclusion Stent retriever thrombectomy of calcified thromboemboli seems less effective than with other types of clots. Different mechanical properties of calcified clots may render them stiffer and less accessible for stent retrievers. When faced with a calcified intracranial thromboembolus in clinical practice, a more contained approach may be warranted in view of low recanalization rates, and the potential for periprocedural adverse events.
- aneurysm
- angiography
- fistula
- intervention
- stroke
Statistics from Altmetric.com
Introduction
Five randomized controlled trials (RCTs) have proven mechanical thrombectomy to be a safe and effective treatment for large vessel occlusion in patients with acute ischemic stroke.1–5 Using different study protocols, varying inclusion criteria, and distinct endovascular techniques, the recanalization rates ranged from 59% in Multicenter Randomized Clinical trial of Endovascular treatment for Acute ischemic stroke in the Netherlands (MR CLEAN) to 88% in Solitaire With the Intention For Thrombectomy as Primary Endovascular Treatment (SWIFT PRIME). It is not yet clear to what extent patient specific factors may influence the success of endovascular therapy, and there is still some debate about the most appropriate technique. Hentschel et al have shown higher recanalization rates using stent retrievers (97.0%) compared with non-stent retriever thrombectomy (79.8%).6 Some studies have shown higher success rates with proximal balloon occlusion compared with interventions without proximal protection. However, little research has focused on the characteristics of the thromboembolus itself, and its potential effect on the success of recanalization.
Based on histological analysis of thrombi retrieved from 36 acute stroke patients, artheriogenic emboli with a core rich in red blood cells (56.9%±12.2%) and peripherally located platelets, and cardiogenic emboli with fibrin as the predominant component (39.5%±13.5%), may be distinguished.7 Rarely, calcified thromboemboli causing a large vessel occlusion are encountered. The composition implies different mechanical properties, which may influence the success of recanalization.
The aim of this study was to evaluate the recanalization rates, thrombus device interaction, complications, and patient outcome following mechanical thrombectomy using stent retrievers of calcified thromboemboli in the setting of acute ischemic stroke.
Materials and methods
Patients
We retrospectively reviewed all patients with acute ischemic stroke who underwent endovascular therapy between January 2013 and July 2016, at two centers experienced in mechanical thrombectomy. Inclusion criteria were: acute ischemic stroke with a calcified intracranial thrombus seen on non-contrast CT, treated with stent retriever thrombectomy, age >18 years, and National Institutes of Health Stroke Scale (NIHSS) score >2. Cases were reviewed by two board certified neuroradiologists. Patients investigated with MRI instead of CT were excluded. Differentiation between calcified clots and an underlying stenosis is challenging and may not always be definite. We selected only those patients with sudden onset of neurological symptoms without pre-existing transient neurological attacks. Furthermore, cross sectional and angiographic imaging ruled out local vessel irregularity at the occlusion site. On CT, a calcified clot with a ovoid shape within the vessel lumen without segmental vessel wall calcification had to be illustrated.
The radiological examinations were retrieved from the Picture Archiving and Communicating System (PACS; R11.4.1, 2009; Philips, Best, Netherlands; Sectra, Linkoping, Sweden). The location and size of the embolus were registered on 1 mm non-contrast CT images in the axial plane.8 Thrombus attenuation was quantitatively assessed in Hounsfield units (HU) by drawing a small circular region of interest approximately 1–2 mm in diameter on the embolus. The same measurement was performed on the corresponding vessel segment on the contralateral side. The interventional report was consulted to find out the material used, type of anesthesia, and periprocedural complications. Arterial patency after the endovascular procedure was classified using the modified Thrombolysis in Cerebral Infarction (TICI) score. Clinical data were obtained from the stroke registry, which listed all relevant clinical information, including initial NIHSS score, time of symptom onset, time of presentation, time of groin puncture, application of intravenous tissue plasminogen activator (IV rtPA), symptomatic hemorrhage, and modified Rankin Scale (mRS) score at 3 months.
Intervention
Selective intra-arterial digital subtraction angiography (DSA) was performed on a biplane, high resolution angiographic system (Axiom Artis zee; Siemens, Erlangen, Germany; Allura Clarity; Philips, Best, Holland) using Iopamiro 300 (Iopamidol, Bracco, Switzerland) as the contrast agent. Based on the clinical status and compliance of the patient, the intervention was performed under either general anesthesia or conscious sedation.
An 8 Fr sheath (Terumo, Terumo Medical, Tokyo, Japan) was inserted into the common femoral artery to secure the access. Selective angiography of the occluded territory was performed with a 5 Fr-JB3 catheter (Cook Medical, Bloomington, Indiana, USA). For stable support, a guiding catheter was advanced as distally as possible to the internal carotid artery. A microcatheter was navigated over the microwire to the distal end of the thromboembolus. The microwire was removed and the position of the microcatheter tip distal to the thrombus was confirmed with contrast. The stent retriever (SR) was delivered through the microcatheter and fully deployed across the clot by completely withdrawing the microcatheter. When a distal access catheter was used, it was advanced over the push wire of the deployed SR to the proximal end of the clot. The SR was slightly pulled back until partially re-sheathed within the distal tip of the distal access catheter and both were then withdrawn together through the guiding catheter while maintaining constant suction by manual syringe aspiration. Successful recanalization was defined as TICI 2b–3 on the last angiogram.
Results
A total of 1022 patients with acute ischemic stroke underwent endovascular therapy at two centers within the study period, and 639 had an available non-contrast CT. In 8 (1.3%) with a non-contrast CT, a calcified intracranial embolus was identified, and SR thrombectomy was performed (five women, three men; mean age 80 years, range 68–100 years).
Due to clinical history and presentation, as well as angiographic appearance, all events were classified as acute thromboembolic events rather than underlying intracranial stenosis. The characteristics of these patients are shown in table 1. The mean NIHSS score on admission was 13.5 (IQR 10.25–16.75). The calcified clot was found in the middle cerebral artery in 75%: M1 segment (n=4) or M2 segment (n=2) and carotid T (n=2). No patient had multiple clots. Mean embolus attenuation was 305 HU (range 150–640 HU), with an average diameter of 3 mm (range 2–4 mm). In five patients a carotid atherosclerotic plaque was found on the ipsilateral site of the intracranial occlusion and was the presumed embolic source. One patient had undergone a transcatheter aortic valve implantation (TAVI) prior to acute presentation of a focal neurological deficit. In the remaining two patients, the presumed embolic source was undetermined. Two patients (25%) received IV tPA. In two patients the procedure was done under conscious sedation and in six under general anesthesia. An SR was used in all patients: a Capture LP 3×15 mm (Medtronic, Minneapolis, Minnesota, USA) in four patients, a Solitaire FR 4×20 mm (Covidien/ev3 Inc, Irvine, California, USA) in two patients, and a Solitaire 6×30 mm in two patients. The average number of SR passes was 2.9 (range 1–5). A distal access catheter was used in all except one patient. Successful recanalization (TICI 2b–3) was achieved in only one patient (12.5%) (patient No 7). The mean time interval from symptom onset to groin puncture, and the mean time from door to groin puncture were 265±95 and 126±66 min, respectively (Table 3). One patient was referred from an outside hospital and time of onset was unknown.
Baseline characteristics
In one patient (No 1) with a clot in the right M1 segment, inadvertent detachment of a Capture Mindframe LP 3×15 mm due to fracture of the SR wire occurred during device recovery. The device was left in the M1 segment without any bypass effect and no attempts were made to remove the device. In another patient with an M1 occlusion (patient No 5), a Capture Mindframe LP 3×15 mm was deployed across the thrombus. During device recovery, sudden loss of resistance occurred, and a control run demonstrated active contrast extravasation from a distal M2 branch which was immediately occluded with two coils. The post-interventional CT scan revealed extensive subarachnoid hemorrhage and contrast in the Sylvian fissure (figure 1).

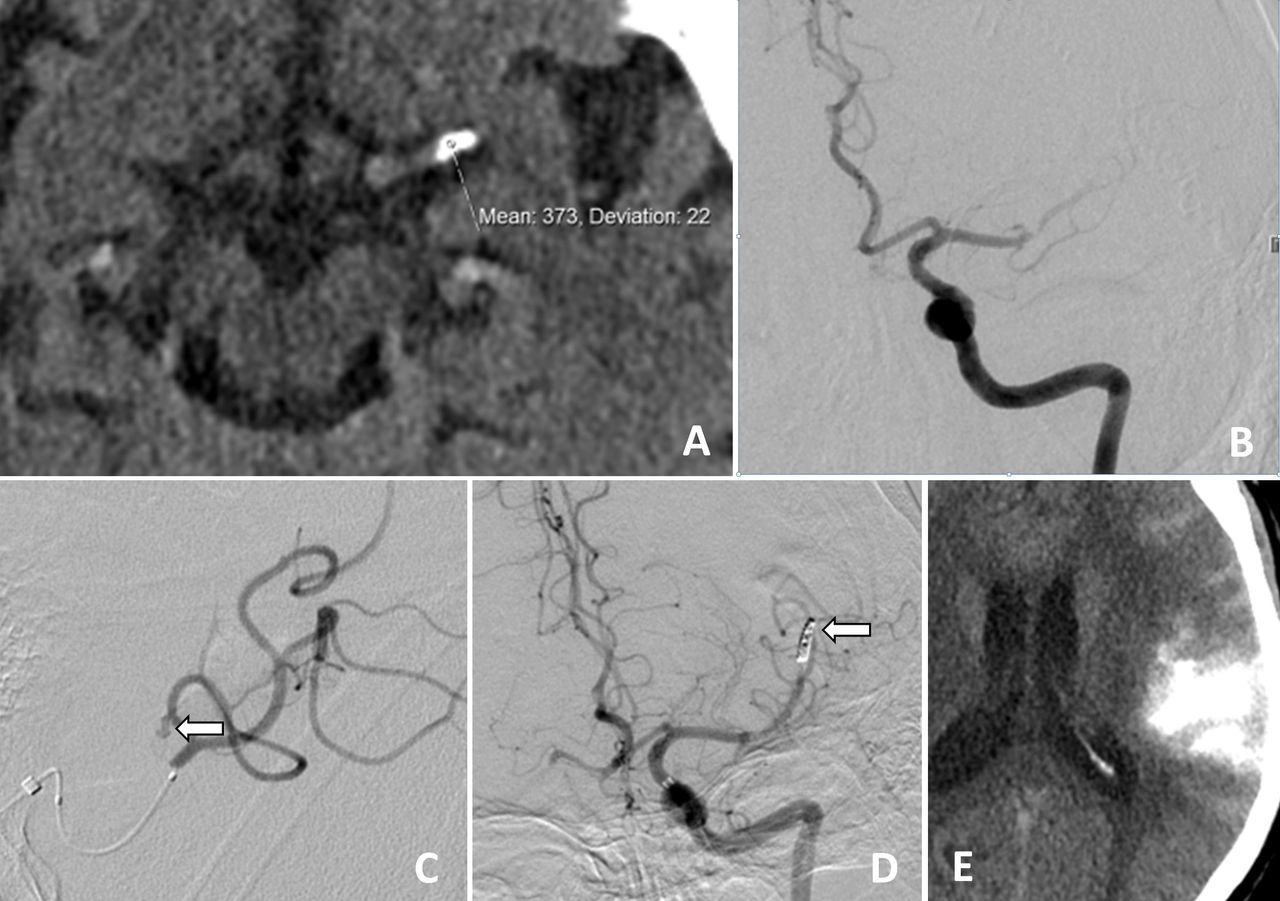
Elderly patient (No 5) presenting with right sided hemiparesis (National Institutes of Health Stroke Scale score on admission of 12). (A) Non-contrast CT demonstrates a calcified clot in the left M1 segment. (B) Corresponding baseline DSA image in the anteroposterior projection shows near occlusion of the distal segment of the M1 segment. (C) DSA after recovery of the Capture LP demonstrates active contrast extravasation from a distal M2 branch (arrow). (D) After coil occlusion of the branch, no active bleeding is visible. (E) Non-contrast CT after intervention demonstrates large contrast extravasation in the sulci of the frontal operculum. Thrombolysis in Cerebral Infarction 0; modified Rankin Scale score of 6.

{kind=link}
{kind=link}
Elderly patient (No 8) presenting with left sided hemiparesis (National Institutes of Health Stroke Scale score on admission of 16). (A) Non-contrast CT demonstrates a calcified clot in the right internal carotid artery terminus. (B) Corresponding baseline DSA in the lateral projection shows the thrombus just above the origin of the posterior cerebral artery, with some residual flow in the anterior cerebral artery (ACA) territory. (C, D) Control DSA in the anteroposterior and lateral projection after thrombectomy with a Solitaire 6 × 30 mm. The thrombus has been pushed into the origin of the M1 segment. Restoration of blood flow in the ACA territory. Thrombolysis in Cerebral Infarction 1; modified Rankin Scale score of 6.
Good outcome at 3 months (mRS 0–2) was observed in only one patient (12.5%) (patient No 7). Five patients (62.5%) died (mRS 6) during the 3 month follow-up period (Figure 2), one patient (12.5%) was severely disabled (mRS 5), and one patient was lost to follow-up.
Three additional patients with a calcified intracranial clot seen on non-contrast CT who had not been submitted to endovascular therapy were not included for further analysis. In two patients (patient Nos 10 and 11), no mechanical thrombectomy was performed based on a multidisciplinary decision, taking into account imaging parameters, including a small infarct volume and good collaterals. In one patient (No 9) who had a calcified thrombus in an M2 branch and a downstream occlusion at the level of the carotid bifurcation, the procedure was stopped because of tortuous anatomy and inaccessibility of the intracranial circulation.
Discussion
Several clinical and imaging parameters, such as NIHSS score, time from symptom onset, size of ischemic core, collaterals, and diffusion weighted imaging/perfusion weighted imaging mismatch play a role in decision making in patients with acute ischemic stroke. To date, very little attention has been paid to the features of the thromboemboli themselves. Based on composition, determined by histological analysis, three different types of emboli may be distinguished. Artheriogenic thrombi show abundant red blood cells in the center and peripherally located platelets covered in fibrin, cardiogenic thrombi have clusters of platelets scattered within a fibrin-rich clot, and calcified thrombi contain large amounts of calcium phosphate.7 9 The three thrombus types may be similar in size, location, and angiographic appearance, but still lead to different recanalization rates, which is most likely due to their distinct mechanical properties. Clots composed predominantly of red blood cells usually show a hyperdense signal on non-contract CT and blooming artifacts on susceptibility weighted imaging, whereas thrombi with abundant fibrin show no artifacts on susceptibility weighted imaging.10 However, the composition of thrombi may vary, and current imaging techniques cannot always reliably distinguish between all of them. Calcified clots have a unique feature, which may be appreciated on non-invasive imaging. This group offers a model to seek to answer a principal question: is recanalization and the success rate of SR thrombectomy dependent on thrombus composition?
As shown in an animal study by Yuki et al, fibrin-rich clots yielded significantly lower recanalization rates (37.5%) and required more recanalization attempts than erythrocyte-rich clots (100%) using the Merci device.11 The authors attributed this significant difference to distinct histopathological composition. In a study in 34 patients suffering acute ischemic stroke (AIS) of the anterior circulation, thrombi rich in white blood cells showed lower recanalization rates, a longer intervention time, and a less favorable outcome.12 As stated by Kaesmacher, periprocedural thrombus fragmentation is more likely to occur with higher neutrophil levels in the thrombus.13 In a study by Jagani, there was no relationship between clot density and revascularization success or stroke etiology.14 Chueh et al investigated the mechanical properties of thromboemboli and concluded that calcified specimens were stiffer than arteriogenic and cardiogenic emboli, which may have an influence on recanalization.15
The incidence of calcified thrombi identified on CT is comparatively low. From our records, only 1.3% of all patients with acute vessel occlusion with available non-contrast CT undergoing endovascular therapy with a SR fell into this group.
A good recanalization result in our study was achieved in only one patient undergoing thrombectomy (12.5%), which is substantially lower than the numbers published in large RCTs, which ranged from 59% in MR CLEAN to 88% in SWIFT PRIME.1 4 This also applies to good clinical outcome at 3 months (mRS 0–2), which was observed in only one patient (12.5%) in our study population, in clear contrast with the numbers reported in the literature. Furthermore, the mortality rate of 62.5% and the complication rate in our study were considerably higher than those reported in earlier studies (table 2). The low recanalization rates and poor outcome may not be attributed to thrombus composition alone. Other factors such as generalized atherosclerosis, cardiac disease, and the older age compared with the large RCT should be considered. Although no general statement may be based on this small case series, and the incidence of calcified emboli in the randomized trials is not known, this comparison shows a striking difference between calcified thrombi and an unselected clot types in the general population of patients undergoing endovascular treatment (EVT).
Comparison of reperfusion, clinical outcome, and mortality in large randomized controlled trials and in our study
Baseline characteristics and treatment variables of all patients undergoing an endovascular procedure*
In our study, an SR was used in all patients. The principle of stent retriever thrombectomy is the compression and entrapment of thrombus material within the stent struts before withdrawal. While this seems a reasonable approach, and has been verified in in vitro studies on soft and elastic thromoemboli, it is questionable whether calcified thrombi, which pose higher resistance to deformation, may be effectively retrieved with this technique. Constant radial force of the SR on the clot is required during retrieval in order to retain the material within the stent struts. Alternative techniques such as intra-arterial rtPA, primary aspiration, and intracranial stenting should be considered when faced with this thrombus type, but this issue was not addressed in our study.
Since the first description of calcified intracranial emboli in 1981 by Yock, only 48 cases had been reported in the literature up to 2014.16 Recently, Walker et al reported on 22 patients with calcified cerebral emboli seen at their institution between 2001 and 2013, where the most frequent presumed sources of embolic material were calcified aortic stenosis (36%), carotid atherosclerotic plaque (30%), and mitral annular calcification (11%).17 As described by Walker and in several case reports, most embolic events occur spontaneously without any inciting event, a finding that was also observed in our series.17 However, two events (25%) occurred after an intra-arterial procedure (aortic valve implant, n=1; renal artery stenting, n=1).
In fact, with increasing numbers of patients undergoing minimally invasive heart valve interventions, especially in the setting of aortic valve stenosis, the number of calcified intracranial thromboemboli may be underestimated and may rise in the future. A recent meta-analysis in patients undergoing TAVI using a transapical or transfemoral approach reported a 30 day stroke incidence of 4%, and had the strongest independent association with a high early and late mortality.18 19 As reported by Tay et al, most cerebrovascular events in patients undergoing TAVI occur within 24 hours (11 of 23, 48%).20 This seems to indicate that the native aortic valve is the source of emboli which may show abundant calcification. Intraoperative transcranial ultrasound monitoring of the middle cerebral artery in patients undergoing TAVI revealed that embolic events peak during valvuloplasty and valve placement.21 22
The limitations of our case series include the small number of patients with a rare type of embolus, the retrospective nature of our review, and the lack of a control group. It would be interesting to evaluate the efficacy of different thrombectomy devices in calcified clots in an in vitro model.
Conclusion
Calcified clots represent a rare type of intracranial thrombi seen in patients with ischemic stroke which, according to our results, show lower recanalization rates than those for non-calcified thromboemboli after SR thrombectomy. A more contained approach may be warranted in view of the rather low recanalization success and the risk of periprocedural complications. SRs are the mainstay of endovascular therapy for acute ischemic stroke but their success
with calcified thrombi which show different mechanical properties has not been validated.
Acknowledgments
We thank Susan Kaplan for proof reading.
References
Footnotes
Contributors Study concept and design: TD, EP, and JG. Acquisition, analysis, or interpretation of the data: TD, EP, AC, FZ, LR, SJ, UF, PM, and JG. Drafting of the manuscript: TD, JG. Critical revision of the manuscript for important intellectual content: TD, EP, AC, FZ, LR, PM, SJ, UF, PM, and JG. Study supervision: AC, UF, and JG.
Competing interests UF: Swiss National Science Foundation (SNSF) research grants, Global PI SWIFT DIRECT trial, and consultant for Medtronic. JG: Global PI of STAR and SWIFT DIRECT (Medtronic), consultancy; CEC member of the Promise Study (Penumbra), consultancy; and Swiss National Science Foundation (SNSF) grants for MRI in stroke.
Ethics approval The study was approved by the local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.