Article Text

Abstract
Background Sacral dural arteriovenous fistulas (DAVFs) are rare vascular abnormalities of the spine characterised by slowly progressive symptoms that can mimic different myelopathy disorders.
Object To report our single Institution experience with sacral DAVFs.
Methods We retrospectively reviewed the clinical records of patients admitted from 1 January 2006 to 31 December 2016 with a diagnosis of sacral DAVFs, treated by endovascular embolisation or surgical clipping. Clinical presentation, imaging characteristics, treatment results and follow-up were analysed.
Results We identify 13 patients with sacral DAVFs supplied by lateral sacral arteries. Clinical presentation was characterised by different degrees of motor weakness and sphincter disturbances. In all patients, spinal MRI showed spinal cord hyperintensities with enhancement and prominent perimedullary vessels. Selective internal iliac angiography was mandatory to identify the exact location of the fistula. A complete embolisation was achieved in eight patients performing a single endovascular embolisation and in three patients performing a single surgical disconnection: two patients required combined procedures. Follow-up imaging showed a complete resolution of the spinal cord hyperintensities in 81% of patients and a reduction of the intramedullary enhancement in 91%. Gait improvement was observed in 73% of patients, while remaining stable in 27%. Sphincter disturbances improved in 36% of patients and remained stable in 64%.
Conclusion Awareness of sacral location of DAVFs is critical because standard spinal angiography will not identify sacral supplies, unless internal iliac arteries are properly examined. In our experience, the endovascular treatment show results comparable to surgery when the fistula point is correctly disconnected.
- spine
- lumbosacral
- subdural
- fistula
Statistics from Altmetric.com
Introduction
Spinal dural arteriovenous fistulas (DAVFs) are the most frequent vascular abnormalities of the spine, accounting for approximately 70% of all vascular spinal lesions.1 The arteriovenous (AV) shunt between the radiculo-meningeal artery and the radicular vein is usually located inside the dura mater at the dorsal surface of the dural root sleeve in the intervertebral foramen, where the two vessels run parallel.2 The resultant arterialisation of the radicular vein and of the valveless perimedullary venous plexus leads to a reduced venous outflow in the radiculo-meningeal artery and to a progressive spinal cord edema. At presentation, the symptoms are often subtle and nonspecific, thus the following clinical course is often slowly progressive, causing a high rate of missed or delayed diagnosis.3 Furthermore, the sacral location of the dural fistula is more rare and can be undetected if common iliac and sacral lateral arteries are not properly investigated during selective angiography performed for a precise suspicion of sacral DAVF.
In this article, we report our single Institution experience from 2006 to 2016 of 13 sacral DAVFs supplied by lateral sacral artery (LSA), treated with endovascular embolisation or surgical clipping alone or in combination.
Methods
Chart review
We retrospectively reviewed the clinical records of patients admitted to our Institution from 2006 to 2016 with a diagnosis of sacral spinal DAVFs with the aim of evaluating the clinical presentation, the diagnostic imaging, the type of treatment and outcome.
Clinical presentation
For each patient the clinical presentation was evaluated in terms of symptoms (motor weakness and sphincter disturbances) and in terms of time between the onset of the symptoms and the definitive diagnosis. Clinical features of patients were adjusted to the Aminoff and Logue scores (ALS)4 before and after the procedure and according to last follow-up visit.
Diagnostic imaging
We investigated the imaging characteristics of spine magnetic resonance (MR) imaging and spinal angiography. All spine MR examinations were performed on a 1.5T Avanto MR imaging system (Siemens, Erlangen, Germany). The examinations included sagittal T1-weighted spin echo, sagittal T2-weighted fast spin echo, axial gradient echo and post-gadolinium sagittal T1-weighted sequences. A biplane flat-panel detector angiographic suite (AXIOM Artis Zee Biplane angio suite equipped with DynaCT; Siemens Medical Solutions, Erlangen, Germany) was utilised for both diagnostic and interventional procedures. The angiographic diagnostic protocol included catheterisation of all intercostal and lumbar arteries, thyrocervical, costocervical and vertebral arteries, and both iliac arteries. In addition, as standard practice, a cone-beam volume CT (CBCT) examination with the same flat panel was performed, in order to obtain pseudo-angio CT images to precisely define the angio-architecture of the AV shunt.5 More specifically, projection images were acquired with a 30×40 cm flat panel detector, with a resolution of 616×480 pixels. Image acquisition covered 100° left anterior oblique to 100° right anterior oblique in a screw axis rotation of the C-arm with the x-ray tube moving under the patient. Total acquisition time was 8 s for 397 projection images, 90Kv by using the 360mGy/frame dose mode and angulation step of 0.50°/frame. The CBCT was acquired during selective arterial catheterisation of the feeding artery to the sacral DAVF, with a manual injection of 20% diluted contrast (Iopamiro 300 mg, Bracco, Milan, Italy). The injection was accurately timed throughout the whole 8 s acquisition time, using a 20 ml syringe.
Treatment
Patients underwent endovascular embolisation or surgical clipping following an interdisciplinary discussion of each case. Endovascular treatment was performed as a first-choice therapy, under general anaesthesia and systemic heparinisation, monitored with activated clotting time. In order to reach the fistula point, as previously documented in the diagnostic DSA, a 6Fr Special catheter (Cordis Neurovascular, Miami Lakes, FL, USA) was placed by a right femoral approach into the internal iliac artery and a glue-compatible over-the-wire microcatheter Marathon (Covidien Irvine, CA, USA) was negotiated, over an Hybrid 12/14 guidewire (Balt, Montmorency, France) into the lateral sacral artery. Subsequently a mixture of diluted N-butyl-cyanoacrylate (Glubran Gem, Lucca, Italy) and ethiodised oil (Lipiodol, Guerbet, Paris, France), with a concentration of 20%–30% depending on the AV shunt haemodynamic, was slowly injected, under a blank roadmap, in order to occlude the fistula point and the proximal segment of the draining vein. At the end of the procedure, the microcatheter was gently removed and DSA injection from both the internal iliac artery was performed in order to confirm the complete occlusion of the tributary vessels of the fistula. In addition, the pedicle supplying the anterior spinal artery was always checked. Surgical treatment was considered as an alternative in case of unfavourable vascular anatomy of the arterial feeders, in a setting not suitable for selective catheterisation, and consisting of focal haemilaminectomy and microsurgical intradural interruption of the draining vein, close to the fistula point, by clipping. The treatment success and the procedural complications were evaluated for each patient.
Follow-up
Immediate post-operative spine MRI was performed in all cases, and used as baseline imaging for the following FU. The patient underwent both clinical and spine MR examinations at 3, 6 and 12 months after the treatment and, when it was possible, once each year thereafter. The primary component of interest was the clinical outcome, investigated at the follow-up medical visit, according to the Aminoff and Logue score. The secondary components of interest were resolution of T2 hyperintensity/swelling of the spinal cord and decrease of intramedullary enhancement, observed at follow-up MRI. Data are presented using descriptive statistics, including percentages and counts for categorical data and means for continuous data.
Ethics
The Ethical Committee of the Institute approved the study. The requirement for written informed consent from all patients was waived by the IRB according to national policies for observational studies.
Results
Chart review
We identified 13 patients, four females and nine males, with sacral DAVFs out of 93 patients with spinal DAVFs. The age ranged from 48 to 78 years, with a mean age of 64 years. Patient data are summarised in table 1.
Clinical data, treatment and follow-up in patients with sacral DAVFs
Clinical presentation
At admission, all patients had an association of motor weakness and sphincter disturbances (ALS: G5 1/13, G4 3/13, G3 8/13; M3 9/13, M2 3/13, M1 1/13). Before admission to our Institution, two patients were erroneously treated for inflammatory myelitis and one for herniated disc elsewhere, without resolution of the symptoms. Data collected from the past medical histories demonstrated a mean of 1.4 (range 1–3) digital subtraction angiography (DSA) attempts to achieve diagnosis. The mean time from symptoms onset to definitive DSA diagnosis was 14 months (range 6–24 months).
Diagnostic imaging
In all cases, pre-operative spine MRI showed extensive hyperintensity/swelling of the spinal cord from the thoracic segment to the conus, associated with intramedullary enhancement and prominent perimedullary vessels on post-contrast images (figure 1AB–A’B’, 2A–B). Precise location of the sacral fistula was identified in all patients performing a spinal angiography, by selective injections of both internal iliac arteries to demonstrate the vascular supplies to the shunt from the lateral sacral arteries (figures 1C–D and 2C). In 7/13 (53%) cases, diagnostic DSA was performed under general anaesthesia, in order to minimise motion artefacts in uncooperative patients and to provide adequate visualisation of slow-flow AV shunts. The fistula was located between L5-S1 in six patients, S1-S2 in four and S2-S3 in three (table 1). The CBCT images detailed the AV-shunt and showed the presence of the arterialised dilated filum terminale draining vein (FTV) in all of the cases (figure 1G–G’ and 2D–E).

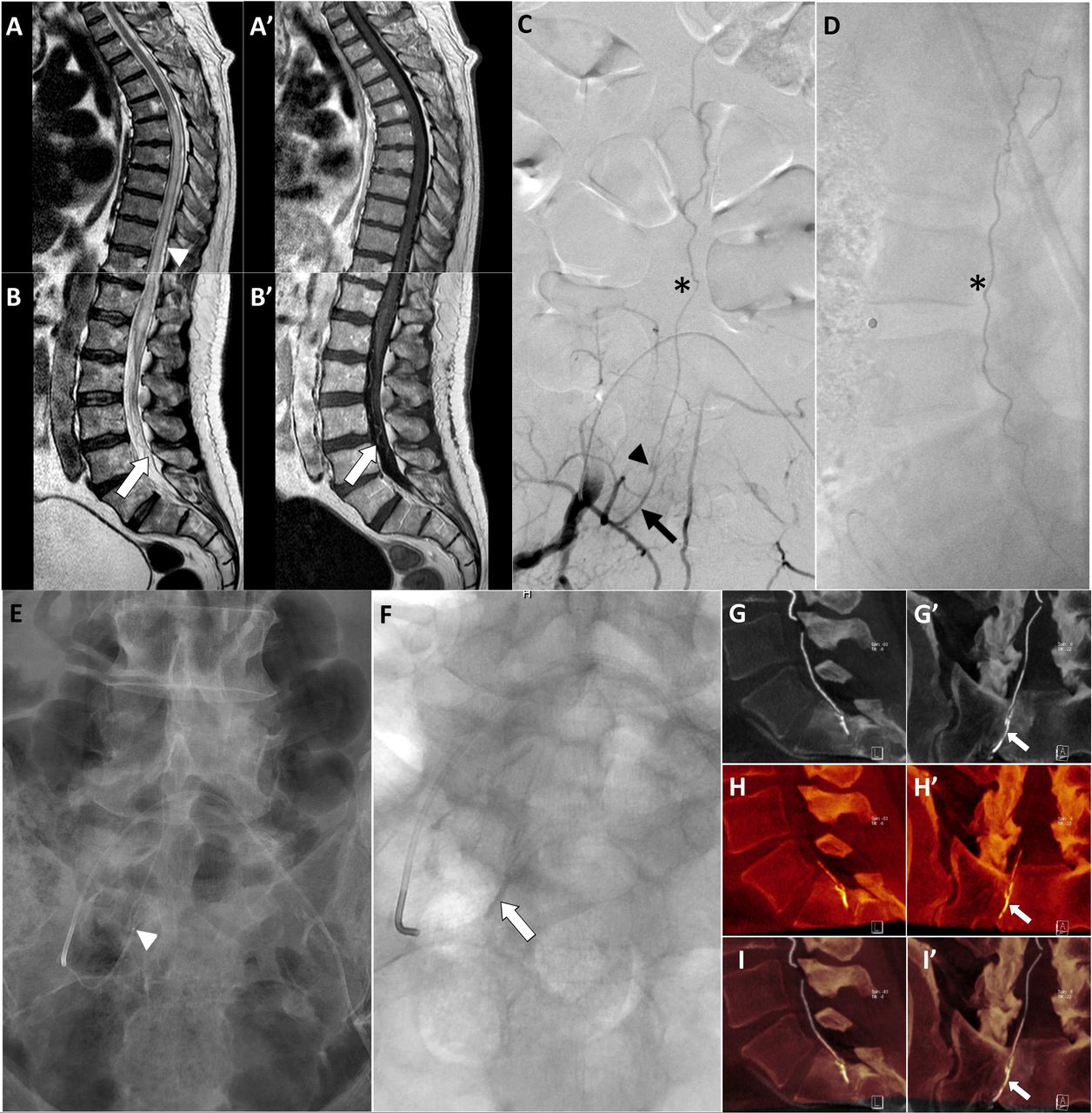
Patient 1: Sagittal T2-wi MR (A–B) and sagittal contrast-enhanced (CE) T1-wi MR (A’–B’) show spinal cord swelling with abnormal contrast enhancement of the conus and dilated pathological perimedullary vessels (white arrowhead): the white arrow point to the dilated filum terminalis vein. Right hypogastric artery selective DSA in antero-posterior (C) and lateral (D) projections demonstrates a sacral DAVF supplied by the LSA (black arrow), the fistulous point (black arrowhead) and the dilated FTV (black asterisk). Unsubtracted DSA image (E) shows the microcatheter negotiated into the LSA, with the tip (white arrowhead) close to the fistulous point. Post-endovascular treatment native DSA image (F) exhibits the glue cast (white arrow) across the AV shunt. Fusion imaging (I–I’) between sagittal and coronal maximum-intensity-projection (MIP) images from pre-treatment CE-CBCT (G–G’) with the MIP CBCT images after embolisation5 (H–H’) show the distribution of the glue (white arrow in H') along the feeding artery (white arrow in G') from the right S1 foramen to the draining vein, across the fistulous point (white arrow in I’).
{kind=link}
{kind=link}
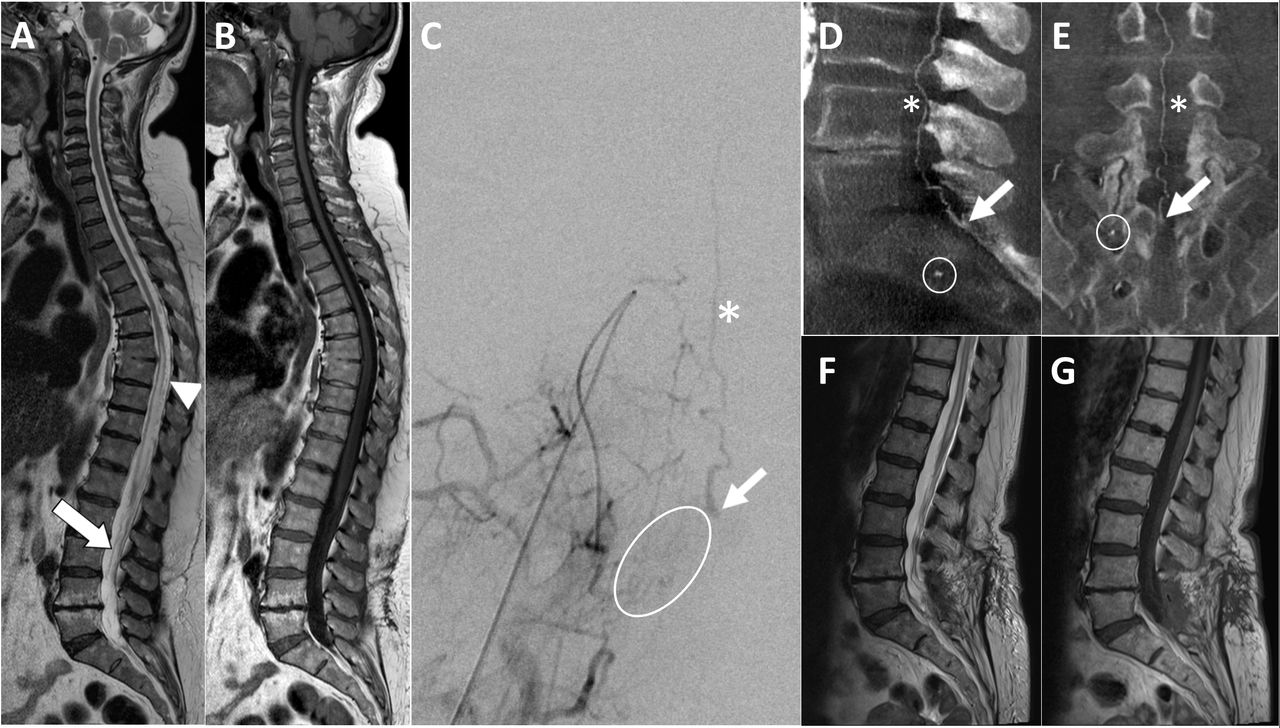
Patient 6: Sagittal T2-wi MR (A) and sagittal CE T1-wi MR (B) show extensive swelling of the spinal cord from the thoracic segment to the conus, associated with intramedullary enhancement and prominent perimedullary vessels (white arrowhead): the white arrow point to the dilated filum terminalis vein. Right hypogastric artery selective DSA (C) demonstrates a sacral DAVF supplied by multiple small arteries (white circle) arising from the LSA, in a setting not suitable for endovascular embolisation. The white arrow indicates the fistulous point, the white asterisk the dilated FTV. Sagittal (D) and coronal (E) MIP images from CE-CBCT show the feeding artery from the right S1 foramen (white circle), the fistulous point (white arrow) and the FTV (white asterisk). Sagittal T2-wi MR (F) and sagittal CE T1-wi MR (G) performed 3 months after surgical treatment show a reduction of the spinal cord swelling and a complete resolution of the intramedullary enhancement: pathological perimedullary vessels are no more visible.
Treatment
Regarding procedural results, a complete cure was achieved performing a single endovascular embolisation (figure 1E–F, H–H’ and I–I’) in 8/13 patients (62%) and a single surgical disconnection in 3/13 (23%). In one patient, two surgical attempts prior to a conclusive endovascular embolisation were performed, due to unsuccessful identification of the draining vein during dural exposure. One patient underwent an incomplete endovascular attempt and only subsequent surgery scored a complete occlusion of the fistula shunt (table 1). We faced very few complications, none of them permanent. In one case a cerebrospinal fluid leak after surgical clipping that resolved spontaneously in 1 week, and in one case a temporary paraplegia after embolisation, which resolved in few days after high corticosteroids therapy, interpreted as a possible contrast-induced neurotoxicity. No major or permanent complications were observed during post-operative hospitalisation.
Follow-up
In all cases, at the immediate post-treatment spine MRI, spinal cord hyperintensities on T2-weighted images and the intramedullary enhancement on post-contrast images remained unchanged, even in the paraplegic patient. Prominent perimedullary vessels were still visible after the treatment only in one patient who underwent an immediate DSA control, which confirmed the absence of any residual arterovenous shunt.
In our series, the mean follow-up time was 31 months (range 6–57 months). Two patients died of unrelated causes (patient 3 for acute respiratory failure, patient 7 for acute myocardial infarction) before the first post-operative visit and therefore were lost to follow-up. At latest follow-up, spinal MRI showed a complete resolution of the spinal cord hyperintensities on T2-weighted images in 9/11 (81%) patients and a decrease of the intramedullary enhancement on post-contrast images in 10/11 (91%) patients (figure 2F–G). At clinical examination the gait improved in 8/11 (73%) patients, while remained stable in 3/11 (27%). Sphincter disturbances improved in 4/11 (36%) patients and remained stable in 7/11 (64%) patients. The ALS at diagnosis and at follow-up, respectively, are reported in table 1.
Discussion
Spinal DAVFs are a rare cause of progressive myelopathy, with an annual incidence of 5–10 cases per million.6 Among these, a sacral location of the fistula occurs in only 5%–10% of cases in the largest series reported in the literature.7 In our series, we observe a higher frequency of sacral DAVFs (14%) when compared with data already published in the literature. This is probably because our Institution is one of the major referral centres for cerebral and spinal vascular disease in Italy. As a tertiary centre, the Department’s activity is characterised by the recruitment and investigation of rare and undiagnosed vascular diseases, usually referred for a second opinion from other hospitals. In addition, the knowledge of sacral DAVFs haemodynamic among physicians is generally limited, causing delays in referral and misdiagnosis, therefore the frequency of the disease could even be higher than those reported in literature. The pathogenesis of spinal DAVFs remains unclear but the middle-age onset suggests an acquired condition. Sacral DAVFs usually presents the same symptoms as thoracic DAVFs, which are the most common location. In fact, independently from the exact artery and vein involved, the arterialisation of the valveless perimedullary venous plexus and the subsequent venous hypertension affects the spinal cord in a gravity-aided caudo-cranial direction.
The clinical presentation is a combination of motor weakness, sensory disturbances and sphincter dysfunctions,8 as confirmed in our series. These clinical symptoms may be shared by various myelopathy disorders including anterior spinal artery infarction, myelitis, spinal cord neoplasms as well as degenerative disc disease.4 In several series and case reports, patients had undergone some other kind of surgical treatment before the identification of the sacral DAVFs,9 similarly to our patients 2, 7 and 10 (table 1). Furthermore, symptoms are slowly progressive, causing a high rate of delayed diagnosis and consequently late treatment. In our series, the mean time from the symptoms' onset to diagnosis was 14 months, highly comparable to those reported in other series.10 Awareness of this rare location of DAVFs by physicians is crucial, in order to achieve a prompt diagnosis and treatment of the AV shunt, preventing further disabling symptoms.
Aside from the nonspecific clinical presentation, the initial diagnosis of sacral DAVF is often complicated by a lack of specific imaging findings.11 The MR features at presentation (spinal cord swelling, increased signal on T2-weighted studies and intramedullary enhancement) may vary among patients and are highly non-specific.12 13 The most specific sign of venous hypertensive myelopathy on MR studies is the presence of prominent perimedullary vessels. Even if literature quotes this finding in fewer than half of the patients with spinal DAVF,14 in our series we were able to identify the prominent perimedullary vessels in every MR study. Retrospectively, we also recognised in every case the prominent FTV draining of the fistula, as a curvilinear hypointense vessel running into the dural sac between the cauda roots, well visible on T2 sagittal MRI. However, though a correct interpretation of the imaging studies is essential to a proper and early diagnosis, a radiologic picture based on MRI alone is not enough.
Once a preliminary suspect of spinal DAVF is made, a definitive identification of the AV shunt requires an angiographic evaluation.15 In our series, only the selective catheterisation of the internal iliac arteries permitted to show the sacral DAVFs, fed by branches of the LSA.16 Interestingly, data collected from the past medical histories demonstrated a mean of 1.4 (range 1–3) DSA attempts to achieve diagnosis. DSA series of patients 2, 3, 7 and 11, acquired in other hospitals, showed how the selective catheterisation of the internal iliac arteries was not performed at the time of the diagnostic procedure: patients 7 and 11 underwent only selective injection of the common iliac arteries, not adequate to opacify the sacral DAVF. The visualisation of the sacral AV shunt at the dorsal surface of the dural root sleeve in the intervertebral foramen can go undetected if the internal iliac arteries are not selectively injected at the time of spinal angiography. Some important arteries supplying the sacral spinal cord segments, such as the ilio-lumbalis and lateral sacral arteries, arise from the posterior trunk of the internal iliac artery. From the ilio-lumbalis artery arise ascending branches, which run along the lumbar nerves ending into the spinal canal. The LSA lies lateral to the anterior sacral foramina, and usually splits into superior and inferior branches, sending branches into the sacral canal, supplying radicular and spinal arteries. Notably in all spinal angiograms, we observe a dilated FTV. The FTV is continuous with the anterior spinal vein, which runs above, and it is the only longitudinal collector seen below the L2 region. Any AV shunt draining towards the spinal cord must drain through the FTV. Accordingly, it is reasonable to propose that an engorged and tortuous intradural FTV may indicate the existence of a sacral DAVF17 18 in case of spine MR myelopathy. Additionally, angiography remains the only way to correctly identify the anterior spinal artery and the artery of Adamkiewicz in order to avoid major complications at treatment.
The optimal management strategy to cure sacral AV fistulas remains controversial thus far. The most important aspect is that therapy must be performed immediately after the diagnosis. Treatments of sacral DAVF consist of permanent occlusion of the AV shunt by clipping or gluing using a liquid embolic agent. Surgical disconnection has been described as the therapeutic treatment of choice.19 Microsurgical interruption by target laminectomy, dura opening and bipolar coagulation or clipping of the pathologic draining vein is a straightforward procedure, with a near-total success rate.20 Although surgery is an effective therapy, interventional techniques are rapidly improving, thus, at present, they represent a viable alternative with reliable outcomes. The goal of endovascular therapy is occlusion of the arterial feeder, the fistulous communication and the proximal venous outflow, similar to surgery. First endovascular experiences, several years ago, with polyvinyl alcohol (PVA) particles were disappointing with a much higher delayed failure when compared withsurgery.21 Nowadays PVA particles are rarely utilised, while the use of N-butyl-cyanoacrylate (n-BCA) glue is preferred. In fact, the n-BCA when it reaches the nidus of the dural fistula and penetrates into the venous side, leads to a durable occlusion of the fistula. Recent reports of n-BCA embolisation notify a permanent occlusion of the fistula in 85% of patients,22 a result comparable to the 90% occlusion rate for the endovascular procedures in our series. There are few papers23 24 regarding the use of Onyx (EV3, Irvine, Ca, USA) or PHILL (Microvention, Inc California, USA) for the treatment of spinal DAVFs. Onyx and PHILL are liquid polymers commonly used when an increased penetration is needed to reach and obliterate the fistulous point. In the case of sacral DAVFs, when the vascular anatomy is favourable and the catheter can be safely placed close to the fistulous point, an increased penetration is not needed and n-BCA is an effective treatment option. When the vascular anatomy is not favourable, for example in the presence of multiple small feeders, and the catheter cannot be safely placed close to the fistulous point, liquid polymers are risky to use because they may not reach the target or produce a temporary and incomplete occlusion of the proximal draining vein, due to a laminar precipitation of the embolic agent from the peripheral part of the lumen. In this scenario, surgery should be preferred rather than endovascular therapy. In addition, long-term outcome for spinal DAVFs treated with Onyx or PHILL are not yet available in the literature. In our opinion, the sacral DAVFs differ from other spinal fistulas as the arterialised vein runs along the nerve root for a long tract before reaching the spinal cord, making it safer to inject n-BCA, with a decreased risk of causing any vascular injury to the spinal cord due to inadvertent spreading of the embolic agent into the normal perimedullary venous plexus. As best practice, we recommend, at the end of the embolisation, to examine the arteries below and above to the fistula origin, including the contralateral, to rule out anastomotic pathway or vascular recruitment.
In our series, there seems to be no differences in the outcome of patients treated by endovascular embolisation or surgery, even though a comparative analysis between the surgical and the endovascular groups was not possible due to the limited number of patients. Regardless of treatment modalities, an increased chance of neurological improvement is associated with mild pre-treatment deficit or shorter duration of symptoms. In our series, we noted a slight improvement of motor symptoms in the majority of patients, whereas sphincter disturbances remained stable. This finding may be the result of a very early involvement of the conus medullaris due to the sacral location of the fistula.
From 1972 to date, less than 50 cases of vascular lesions of the spine arising from the internal iliac arteries has been reported in the literature25 .Among them, excluding epidural, direct and post-traumatic fistulas and arteriovenous malformation, we identified only 15 cases of sacral DAVFs arising from the LSA9 16 18 25–32 (table 2).
Literature on sacral DAVFs
Up to date, to our knowledge, our report represents the largest single Institution case series ever published on sacral DAVFs.
Conclusion
Sacral DAVFs represent a small subgroup of a rare and usually misdiagnosed disease. Awareness of a possible sacral location of DAVFs is critical because standard spinal angiography will not identify DAVFs with sacral supply unless the internal iliac arteries are carefully examined at the time of angiography. Our experience documented that in the presence of a long arterialised vein, that is almost always visible into the dural sac at sagittal T2 MRI, the endovascular treatment is safe and effective, even if surgery may still be required in the presence of a very small and diffuse network of arteries feeding the fistula.
References
Footnotes
Contributors All authors made substantial contributions to the conception or design of the work: or the acquisition, analysis, or interpretation of data for the work; drafted the work or revised it critically for important intellectual content; and provided final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Patient consent Obtained.
Ethics approval IRCCS Foundation Neurological Institute ’C. Besta' Ethical Committee.
Provenance and peer review Not commissioned; externally peer reviewed.