Article Text

Abstract
Background Optical coherence tomography (OCT) is a high resolution intravascular imaging method that allows visualization of flow diverter struts and the vessel wall. In this study, malapposition of the flow diverter that continues into the neck of the aneurysm, named communicating malapposition (CM), was investigated as a potential factor for delayed aneurysm healing.
Methods 40 New Zealand White rabbits underwent elastase induced aneurysm creation, and were subsequently assigned to one of four treatment groups based on flow diverter type and administration of antiplatelet therapy. All animals underwent post device deployment balloon angioplasty and subsequent OCT to assess device/vessel apposition. The incidence of CM seen on OCT was assessed with a binary scoring system: 0–CM present; 1–CM absent. At 30 days, DSA was acquired to assess aneurysm healing. Aneurysm healing on terminal DSA was measured using a previously developed 5 point scale, with a score of 3 or 4 considered a positive outcome.
Results All animals were grouped into a single cohort for analysis as no difference in the rate of CM or healing was seen in the four treatment groups. Significant interaction between the absence of CM and a positive outcome was confirmed by Fisher exact test (P=0.0034). Angioplasty was shown to treat 33% of the cases of CM seen at implant, and these treated cases overwhelmingly had a positive outcome (P<0.001).
Conclusion The use of OCT to assess CM of flow diverters has been shown to be predictive of the 30 day healing rate of an animal model of aneurysms.
- aneurysm
- device
- flow diverter
Statistics from Altmetric.com
Introduction
Over the past decade, flow diverter technology has emerged as a valuable endovascular tool for treating brain aneurysms. Despite this increase in use, confounding results from studies have shown both high occlusion rates (75–95%) and positive clinical outcome,1 2 and other studies have shown much lower rates of aneurysm occlusion (of approximately 60%) at standard follow-up time points.3 The precise mechanisms behind delayed aneurysm healing remain elusive. We seek to identify and understand potential indicators of delayed aneurysm occlusion through imaging. Currently, optical coherence tomography (OCT) is used in cardiology to examine strut–to-vessel wall apposition. Recent studies on cardiovascular stenting have shown that poor stent strut apposition can lead to delayed endothelial growth.4 5 Other studies have looked at the presence of malapposition of flow diverters in histologically sectioned samples,6 but techniques to interrogate in vivo malapposition could provide insight on aneurysm healing. Due to the spatial resolution that approaches the cellular level (10 µm) and rapid temporal resolution, OCT in cerebrovascular applications is gaining interest.7–10
Malapposition can occur at any point along the length of the stent. The focus of this work is on malapposition at the level of the aneurysm neck. We introduce the term ‘communicating malapposition’ (CM)—that is, malapposition in the parent artery proximal to the aneurysm and continues into the neck of the aneurysm, effectively creating a much larger neck area. We hypothesize that OCT imaging acquired after flow diverter placement allows for visualization of potential CM, and that this CM is a predictor of poor aneurysm occlusion rates at 30 days. Additionally, we investigated the impact of post-deployment balloon angioplasty on CM.
Methods
All animal research activities were approved by the institutional animal care and use committee. Forty New Zealand White rabbits (sex: either; weighing 3.0–4.0 kg) underwent elastase induced aneurysm creation of the right common carotid artery, as previously described.11 After a minimum of 21 days post aneurysm creation, all aneurysms were screened for size uniformity by either non-invasive DSA12 or non-invasive contrast enhanced VasoCT.13 The animals were assigned to one of four groups (n=10/group): group 1, implant with the pipeline embolization device (PED; Medtronic Neurovascular, Irvine, California, USA); group 2, implant with the PED and use of dual antiplatelet therapy (DAPT); group 3, implant with the PED with Shield technology (sPED, Medtronic Neurovascular); and group 4, implant with the sPED and use of DAPT. The DAPT regimen consisted of oral administration of aspirin (10 mg/kg/day) and clopidogrel (10 mg/kg/day) beginning at least 5 days prior to implant, and continued for the duration of the study. P2Y12 reaction units were obtained using the Verify Now system (Accriva Diagnostics, San Diego, California, USA). All subjects with DAPT had therapeutic P2Y12 reaction units (69±29) compared with 235±46 in rabbits not premedicated with DAPT.
All procedures were performed under general anesthesia and with a strict aseptic technique. Prior to all surgical or imaging procedures, the animals were pre-anesthetized by subcuticular injection of atropine (0.01 mg/kg) and given an intramuscular dose of buprenorphine (0.03 mg/kg) for pain management. Anesthesia was induced by intramuscular injection of ketamine (35 mg/kg) and xylazine (5 mg/kg), and maintained with mechanical ventilation of 1–3% isoflurane. The physiologic status of the animal was assessed using continuous monitoring of respiration rate, heart rate, oxygen saturation level, end-tidal CO2 level, and temperature. For reversal of anesthesia, intravenous yohimbine (0.2 mg/kg) was used. Analgesics were administered twice per day for 48 hours following surgery.
Once anesthetized, the right femoral artery was exposed through a 2 cm incision. A 6 F introducer sheath was inserted over a guidewire and through an arteriotomy of the femoral artery. A Navien-072 guide catheter was positioned in the brachiocephalic trunk and DSA as well as three-dimensional rotational angiography were acquired for the measurements of the subclavian artery and to determine the required device size as per the proximal vessel diameter. The designated flow diverter was deployed under fluoroscopic guidance and implanted such that the entire aneurysm neck was covered. After the device was deployed, OCT imaging (Dragonfly Catheter; St Jude Medical, Westford, Massachusetts, USA) was performed using the ‘Hi-res’ protocol on the ILUMIEN OPTIS system (St Jude Medical). Under this protocol, 540 images were taken along the parent artery and across the neck of the aneurysm. In the case of a common origin of the left common carotid artery, and the brachiocephalic artery, the Navien was advanced such that the tip was distal to the origin of the left common carotid artery. In order to remove blood from the artery during OCT imaging, iodine contrast (Omnipaque 240; GE Healthcare, Malborough, Massachusetts, USA) was injected at a continuous rate of 4–5 mL/s for 3–5 s. After OCT imaging, balloon angioplasty of the entire length of the device (beginning distally) was performed using a HyperGlide balloon (4×10 mm; Medtronic Neurovascular) in all cases. Following angioplasty, OCT was repeated. Finally, VasoCT was acquired. Thirty days after device implant, animals were re-anesthetized and catheter DSA was performed to assess the rate of aneurysm occlusion on a previously described 5 point scale.14
The primary outcome of this study was the rate of positive aneurysm healing, a score of 3 or 4, as a function of the existence of CM (figure 1), on a binary scale of 0 CM present, 1 CM absent. CM was primarily measured on OCT after balloon angioplasty, while the rate of CM seen on pre-angioplasty OCT was also assessed to compare the effect of angioplasty. A Fisher’s exact was used to show significance, and R was used for all statistical calculations. CM diagnosis using DSA and OCT was reported by two raters, and agreement was assessed using Cohen’s weighted kappa (κ) scores. κ was calculated for both pre and post balloon angioplasty as pre and post balloon angioplasty observations were independent. An overall weighted κ was calculated, accounting for all observations made.

(A) Optical coherence tomography (OCT) image of the aneurysm neck, showing no communicating malapposition. (B) OCT image of the aneurysm neck showing communicating malapposition (arrows).
Results
The baseline characteristics of each aneurysm were compared across groups, and no differences were found (table 1). Furthermore, the use of DAPT compared with no DAPT showed no impact on the rate of aneurysm occlusion (50% and 55%, respectively) or on the prevalence of CM (45% and 40%, respectively). This allowed for all 40 animals to be grouped for modeling CM effect on the rate of aneurysm occlusion.
Baseline characteristics as a function of group assignment
Overall, the rate of positive aneurysm healing at 30 days was seen in 53% of the animals (n=21), with no CM seen in 81% of those cases (n=17). Representative images from a CM negative and a CM positive case can be seen in figure 2. Fisher’s exact test confirmed the association between lack of CM and aneurysm healing (P=0.0034) (table 2). Furthermore, when malapposition presented along the parent artery distal to the aneurysm neck was compared with the rate of positive outcome, no association was found (P=0.776).
Contingency table of communicating malapposition versus occlusion status

(A, D) Post-implant DSA. (B, E) Post-angioplasty optical coherence tomography (OCT) depicting device apposition at the neck of the aneurysm. A communicating malapposition (CM) is present in (E) (arrow) but not in (B). (C, F) Thirty day follow-up DSA. The aneurysm that had CM shows patency of the aneurysm, while the aneurysm without CM is completely occluded.
CM observed before balloon angioplasty
In all cases, balloon angioplasty was performed after the flow diverter was implanted, but after an initial OCT sequence had been acquired. This allowed for identification of cases in which the CM was treated—that is, CM was seen on OCT pre balloon angioplasty, but not on OCT after balloon angioplasty (figure 3). Of the 24 cases where CM was seen prior to balloon angioplasty, eight showed positive treatment of the CM (33%), and of those in whom CM was effectively corrected, seven had a positive 30 day aneurysm occlusion rate (88%). This positive treatment outcome was confirmed with a Fisher exact test (P=0.0078) (table 3).
Contingency table of treated communicating malapposition versus occlusion status
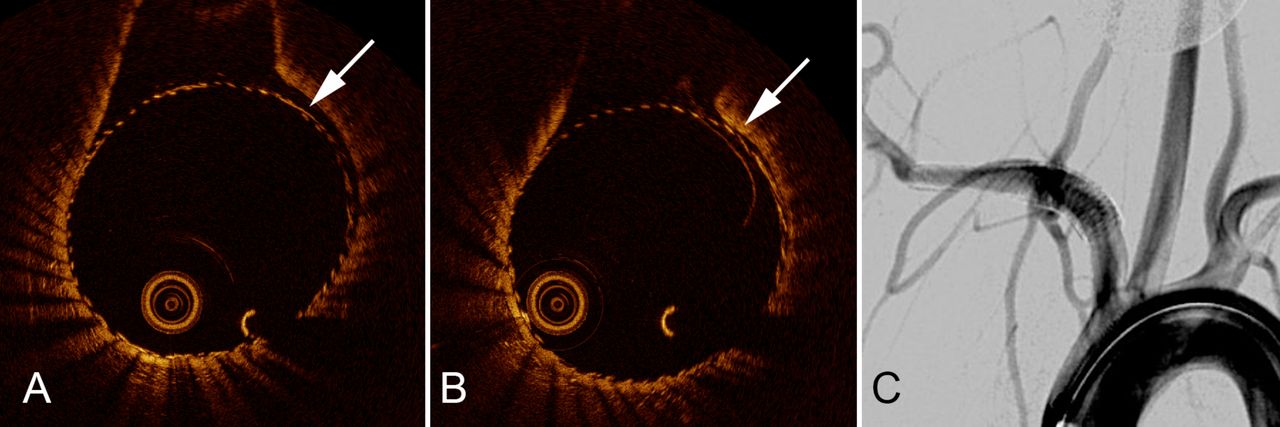
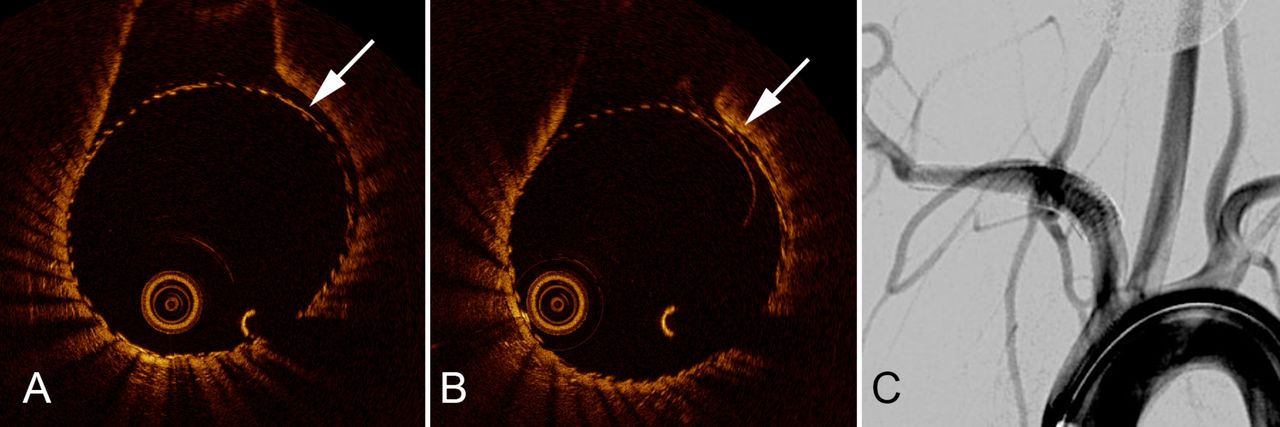
(A) Optical coherence tomography (OCT) image of communicating malapposition (CM) in the parent vessel before balloon angioplasty (arrow). (B) OCT image from the same device after balloon angioplasty, showing correction of the CM (arrow). At the 30 day follow-up, the animal showed good aneurysm healing on angiography (C).
No CM observed before angioplasty
When a subgroup analysis was performed on the set of animals that showed no CM before angioplasty was performed, it was observed that 1 of the 16 (6%) had CM caused by balloon angioplasty (figure 4), and in this case the outcome was poor (P>0.05).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
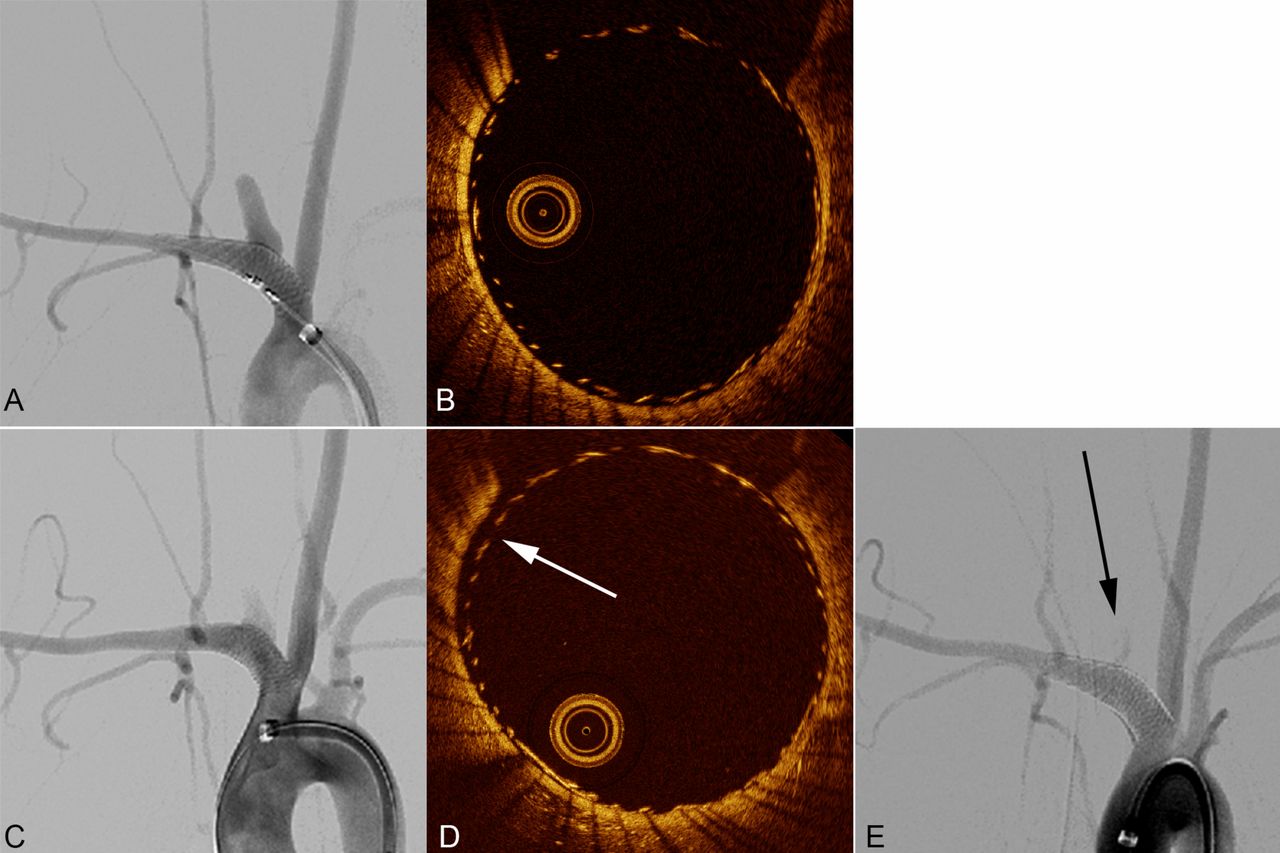
DSA showing frontal projection (A) and optical coherence tomography (OCT) (B) immediately following device implant. Apposition at the neck of the aneurysm was good (B) with no communicating malapposition (CM) diagnosed. Following balloon angioplasty (C, DSA frontal projection), OCT shows appearance of CM (D, arrow). After 30 days, the aneurysm dome continues to fill with contrast (E, arrow).
DSA, OCT, and VasoCT in the diagnosis of CM
Two expert reviewers (each with more than 10 years of experience with diagnostic angiography) blind to the OCT results and 30 day aneurysm occlusion scores rated the presence of CM on DSA images. The inter-rater reliability for diagnosis of CM using DSA was poor (κ=0.32). For both raters, cases that they scored positive for CM were equally likely to have CM present or absent on OCT. DSA interpretation of CM led to unreliable prediction of 30 day dichotomized occlusion score (P=1).
Two raters (<1 year of experience with OCT imaging) blind to the 30 day occlusion scores had substantial agreement in diagnosing the presence of CM (κ=0.75). Taken independently, each rater’s diagnosis of CM as present was significantly predictive of early aneurysm non-occlusion (rater 1, P=0.0034; rater 2, P=0.0037).
VasoCT reconstructed images were reviewed for detection of CM. Although respiratory motion artifacts were absent, as the data were acquired under breath hold, the proximity of the aneurysm model to the heart induced significant pulsation artifacts. The partial volume averaging of this motion in the reconstructed images could not be used for reliable detection of CM.
Discussion
It was recently shown that a malapposition scoring system applied to post explant histological samples correlated well with occlusion rates.6 In this study, we presented a high resolution, intravascular imaging approach to assess malapposition of flow diverters using OCT in vivo. The lack of CM on OCT was shown to have a high predictive value for the rate of early aneurysm occlusion outcome at 30 days. Furthermore, the presence of CM correlates with poor rates of aneurysm occlusion, meaning that the use of OCT for prediction of outcome shows both high sensitivity and specificity. Recently, Periera et al have shown that the DSA based measurement of the mean aneurysm flow amplitude change as the result of flow diverter implantation can be used to predict aneurysm thrombosis at 12 months.15 Perhaps these complementary approaches, when coupled, could offer very high confidence for predicting aneurysm occlusion in response to flow diversion.
Balloon angioplasty is one of the techniques used to treat malapposition of flow diverters when flow irregularities are seen on DSA. In the subgroup of rabbits with CM present on post implant OCT, we have shown that balloon angioplasty can improve the apposition of the flow diverter, and that this improvement in CM results in much higher rates of positive angiographic outcome. In the subgroup of rabbits with no CM prior to balloon angioplasty, for the most part, balloon angioplasty had no effect; however, there was one case in which CM was caused by the balloon angioplasty and in this case the aneurysm had a poor occlusion rate at endpoint. Although not statistically significant, this does raise the concern that ubiquitous balloon angioplasty may have a deleterious effect on the apposition of a well apposed flow diverter. This further reinforces the need for intraluminal imaging in the cerebrovascular space. From this study, the treatment of CM may be an important factor in the overall healing rate of aneurysms, but without direct evidence of CM, balloon angioplasty was shown to be potentially detrimental.
Our study that used current, state-of-the-art flat panel angiography reinforces prior data showing the inability to diagnose CM using conventional DSA.6 This is likely due to the projection nature of DSA that cannot always capture eccentric CM as well as CM that occurs at the limit of spatial resolution of DSA. VasoCT can potentially address these limitations13; however, due to the location of the aneurysm in this model, pulsatile motion of the implant rendered interpretation of the data unreliable. High resolution OCT imaging did reveal CM where the extent of the malapposition from the vessel wall was only slightly larger than the stent struts, which may be at the detection limit of VasoCT.
Our study only examined the impact of CM on early aneurysm occlusion. It is possible that at longer follow-up durations, these aneurysms would progress to complete or near complete occlusion. Therefore, it should not be interpreted that CM leads to treatment failure. However, CM does appear in this model to increase the latency period during which the aneurysm is not adequately treated.
Conclusion
Malapposition of flow diverters at the level of the neck of the aneurysm may play a role in delayed aneurysm healing. OCT is a useful diagnostic tool to image malapposition of aneurysms treated by flow diversion, and more development is needed to build a dedicated, neurovascular OCT system for clinical use. Balloon angioplasty may help to improve malapposition, but judicious use of this technique guided by high resolution intravascular imaging may improve outcomes.
References
Footnotes
Contributors Study design: MM, JMW, MJG, and ASP. Data acquisition: MM, JC, FC, ETL, RMK, OWB, and TT. Literature research: MM, MJG, and ASP. Data analysis and interpretation: RMK, MM, JC, MJG, and ASP. Manuscript preparation: RMK, OWB, ETL, and MJG. Revision of manuscript for important intellectual content: ASP. Approval of final version of the manuscript: all authors.
Funding This work was supported by Medtronic Neurovascular. The content is solely the responsibility of the authors, and does not represent the official views of Medtronic.
Competing interests JC has received educational scholarships from Medtronic Neurovascular and Microvention/Terumo. JMW is employed by Medtronic Neurovascular. MJG has been a consultant on a fee-per-hour basis for Codman Neurovascular, InNeuroCo, Medtronic Neurovascular, and Stryker Neurovascular; holds stock in InNeuroCo; and has received research support from the National Institutes of Health (NIH), Anaconda, Codman Neurovascular, Gentuity, InNeuroCo, Microvention, Medtronic Neurovascular, MIVI Neurosciences, Neuravi, Philips Healthcare, InNeuroCo, Rapid Medical, R92M, Stryker Neurovascular, The Stroke Project, and the Wyss Institute. ASP has been a consultant on a fee-per-hour basis for Medtronic Neurovascular and Stryker Neurovascular; and has received research grants from Medtronic Neurovascular and Stryker Neurovascular.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data queries for raw data (images, etc) can be made to the corresponding author.
Presented at This paper was presented previously at the 14th Annual Meeting of the SNIS, Colorado Springs, Colorado, USA, on 26–28 July 2017 and at the WFITN, Budapest, Hungary, on 16–19 October 2017.