Article Text

Abstract
Background and purpose The aim of the study was to evaluate whether leukoaraiosis severity is associated with outcome in acute stroke patients undergoing mechanical thrombectomy with stent-retriever devices.
Methods In this retrospective multicenter study, we evaluated 251 acute stroke patients (pretreatment National Institutes of Health Stroke Scale score ≥8) treated with stent-retriever devices. Leukoaraiosis severity was graded as 0–2 (absent-to-moderate) versus 3–4 (severe) according to the van Swieten scale. The main clinical outcome was the proportion of good functional outcome, defined as a modified Rankin Scale of 0–2 at 90 days.
Results Significantly fewer patients in the severe LA group than in the absent-to-moderate LA group achieved a good functional outcome (18.4% vs 50.2%, P<0.001). In multivariable analysis, severe leukoaraiosis was a significant negative predictor of good functional outcome at 90 days (OR, 0.27; 95% CI 0.10–0.77; P=0.014).
Conclusions The severity of leukoaraiosis is independently associated with 90-day functional outcome in acute stroke patients undergoing mechanical thrombectomy with stent-retriever devices.
- stroke
- thrombectomy
- leukoaraiosis
Statistics from Altmetric.com
Introduction
Mechanical thrombectomy (MT) using stent-retriever devices has become the standard of care for acute ischemic stroke (AIS) caused by a large-artery occlusion (LAO) in the anterior circulation.1 However, only approximately 40% of these patients achieve good functional outcome in the real world.2 3 The identification of patients most likely to benefit from MT is important for increasing the overall proportion of patients with a satisfactory prognosis after MT. Elucidating factors that influence outcome may be the first and foremost step. Among the different parameters, neuroimaging markers play a central role in selecting MT treatment patients, especially those outside the conventional therapeutic time window.4 5
Leukoaraiosis (LA), a common neuroimaging feature of cerebral small vessel disease, appears as abnormal hypointensities on CT and hyperintensities on T2-weighted or fluid-attenuated inversion recovery (FLAIR) magnetic resonance images. A meta-analysis demonstrated that LA presence and severity were associated with symptomatic intracranial hemorrhage (sICH) and poor stroke outcome after thrombolysis.6 In addition, moderate or severe LA increases the risk of hemorrhagic transformation following thrombectomy with Merci devices.7 In a recent single-center study with a small cohort size of thrombectomy patients using stent-retriever devices, there was no association of LA severity with functional outcome or intracranial hemorrhage risk.8 However, there is a paucity of data from the multicenter analysis with a large cohort, especially in the Chinese populaition.
Thus, the aim of the present study was to investigate the association of severe LA with AIS outcome in a relatively large multicenter cohort of MT-treated patients with stent-retriever devices in the Chinese population. We hypothesized that LA severity might be associated with functional outcome after MT with stent-retriever devices.
Methods
Participants
This was a multicenter retrospective study involving six well-established stroke centers in China. We extracted all consecutive patients between January 2014 and September 2017 according to the following criteria: were diagnosed with AIS; had an LAO in the anterior circulation, confirmed by computed tomographic angiography/magnetic resonance angiography/digital subtraction angiography; age ≥18 years; pretreatment National Institutes of Health Stroke Scale (NIHSS) score ≥8; premorbid modified Rankin Scale (mRS) score <2; and undertaking MT with stent-retriever devices (Solitaire, Covidien, Irvine, CA, USA). We excluded patients whose pre-therapeutic CT scans were unavailable. This study was approved by the ethics committee of each participating center, and patient consent was waived because of its retrospective nature. Details of the treatment approaches and periprocedure management in routine practice are illustrated in the online-only supplementary file 1.
Supplementary file 1
Data collection
Data including demographics, medical history, laboratory measures, stroke severity, imaging characteristics, procedural factors, outcome measures, and safety aspects were recorded. Details of the data elements are shown in table 1. All angiography, CT, and MRI images were sent to the core laboratory in Jinling Hospital, and were evaluated in a blind manner by two physicians/interventionists (YG and SZ), with advice of a third experienced physician/interventionist (WZ) in case of disagreement. LA was assessed using the van Swieten scale (VSS; see online-only supplementary file).9 In the present study, we separately assessed the LA severity in each hemisphere, and considered the nonischemic hemisphere score as the final grade after unblinding. Collateral circulation before thrombectomy was evaluated from the angiograms by the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology scale,10 and good collateral circulation was defined as values≥2. The degree of recanalization was measured using the modified Thrombolysis in Cerebral Infarction score on final post-thrombectomy angiogram,11 with successful recanalization defined as a score of 2b or 3.
Demographics and baseline characteristics stratified by leukoaraiosis severity
Study outcomes
The main clinical outcome was the proportion of good functional outcome, defined as an mRS score of 0–2 at 90 days. The secondary clinical outcomes included futile recanalization (FR), mortality at 90 days, symptomatic intracranial hemorrhage (sICH) within 72 hours, and shifts in disability levels over the entire range of mRS scores at 90 days. FR was defined as successful recanalization without good functional outcome at 90 days. sICH was assessed according to the Heidelberg Bleeding Classification (details are provided in the online-only supplementary file).12
Statistical analysis
Continuous variables were presented as mean ±SD deviation or as median IQR. Categorical variables were presented as percentages. LA severity was defined as absent-to-moderate LA (VSS<3) or severe LA (VSS≥3).13 Systolic blood pressure (SBP) was dichotomized into ≤140 mmHg and >140 mmHg, and NIHSS scores were categorized into 8–15, 16–20, and >20. Continuous variables were analyzed with the Student t-test or Mann–Whitney U test according to their normality of distribution. Categorical variables were analyzed with χ2 or Fisher exact tests. Backward-stepping binary logistic regression analysis was performed to analyze the association of LA severity with 90-day functional outcome, FR, or mortality at 90 days. Variables with P<0.05 on univariate analysis were entered into multivariable analysis (considering age, sex, smoking, drinking, coronary artery disease, atrial fibrillation, hypertension, diabetes mellitus, previous ischemic stroke, baseline SBP, baseline NIHSS score, stroke cause, collateral grade, degree of recanalization, symptoms onset to recanalization time, receiving intravenous alteplase, and LA severity). A multivariable ordinal logistic regression analysis was used for the shift analysis with adjustment for the same covariates that were used in the aforementioned binary logistic regression analysis with modified Rankin Scale scores as a dichotomized outcome variable. Data analyses were performed using statistical software (SPSS 22.0; IBM, Armonk, NY, USA).
Results
Baseline characteristics
We identified a total of 294 AIS patients with anterior circulation LAO treated with stent-retriever devices. Of these, 40 patients with an NIHSS score of <8 were excluded. Among the remaining 254 patients, baseline CT scans were not available in three patients, with a final total of 251 patients eventually enrolled into this study. Baseline characteristics of these patients according to LA severity are listed in table 1.
Study outcomes
Only 18.4% of patients with severe LA achieved a good 90-day functional outcome, compared with 50.2% of patients with absent-to-moderate LA (P<0.001). In 192 patients with successful recanalization, the prevalence of FR in patients with severe LA was higher than that in patients with absent-to-moderate LA (75.9% vs 39.3%, respectively; P<0.001).
Mortality was reported in 60 patients (23.9%). Causes of death were stroke-related (49), cardiac-related (four), pulmonary diseases (four), systemic bleeding (two), and undetermined (one). There was a higher mortality rate in the severe LA cohort compared with the absent-to-moderate LA cohort (50% vs 19.2%, respectively; P<0.001; table 2). The rate of sICH was similar between patients with severe LA and those with absent-to-moderate LA (13.2% vs 9.9%, respectively; P=0.539; table 2).
Outcome according to leukoaraiosis severity
Independent predictors for outcomes
Significant variables in the univariate comparisons were entered into the multivariable model (details are provided in Table in the online-only supplementary file). Severe LA was inversely associated with good functional outcome at 90 days after adjusting for age, baseline SBP, baseline NIHSS score, stroke cause, collateral grade, and degree of recanalization (OR , 0.27; 95% CI 0.10–0.77; P=0.014; table 3). Furthermore, severe LA was a significant independent risk factor for FR after multivariable adjustment for age, baseline SBP, baseline NIHSS score, stroke cause, and collateral grade (OR, 3.59; 95% CI, 1.24–10.43; P=0.019; table 3). In addition, there was a significant association of LA severity with mortality at 90 days after adjusting for confounding factors including age, baseline SBP, baseline NIHSS score, history of coronary heart diseases, collateral grade, and degree of recanalization (OR, 2.58; 95% CI 1.01–6.58; P=0.048; table 3). The associations of leukoaraiosis with outcomes remained when leukoaraiosis severity, baseline NIHSS score, and systolic blood pressure were entered as ordinal or continuous variables in all models (not shown).
Multivariable analyses between severe leukoaraiosis and good 90-day functional outcome, FR, or mortality at 90-days
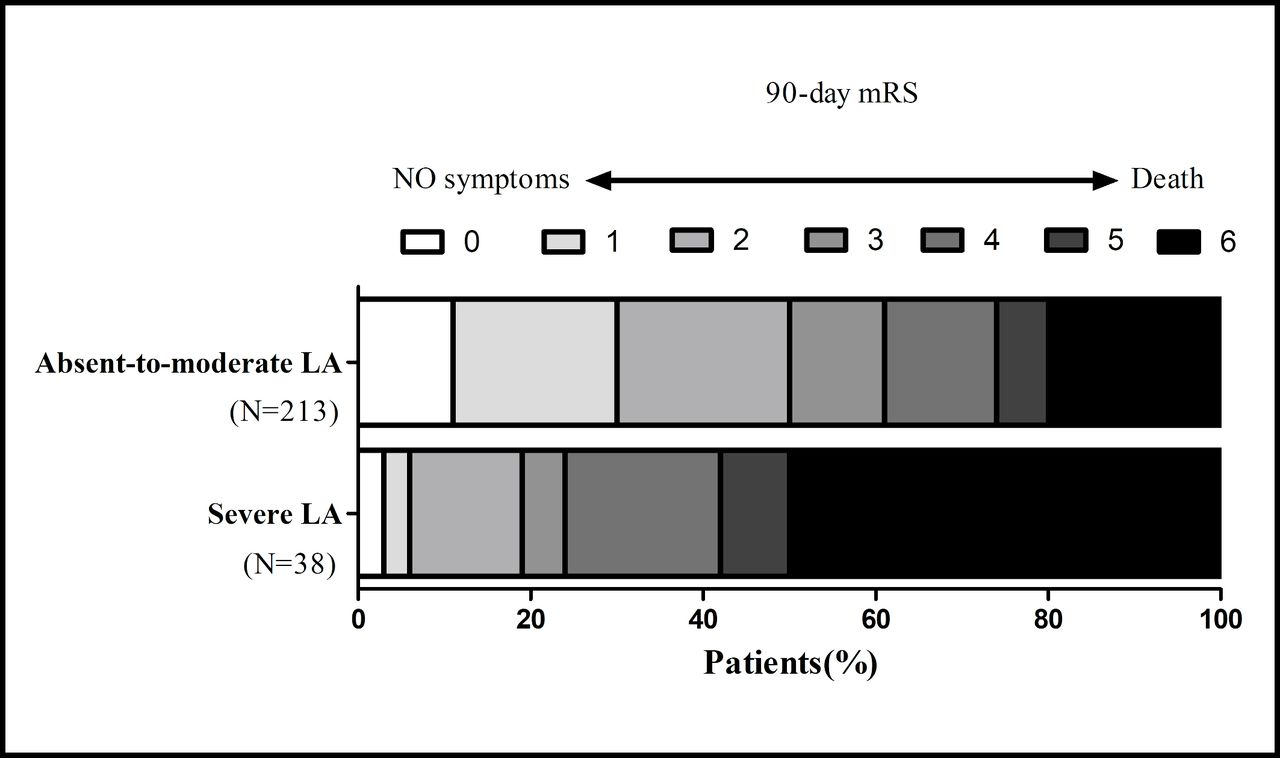
The shift analysis demonstrated that there was a significant difference between patients with and without severe LA in the overall distribution of the 90 day mRS scores (common OR, 2.54; 95% CI 1.22–5.31; P=0.013; figure 1).
{kind=link}
Distribution of modified Rankin Scale (mRS) scores at 90 days according to leukoaraiosis (LA) severity. There was a significant difference between patients with and without severe LA in the overall distribution of mRS scores after adjusting for age, baseline systolic blood pressure, baseline National Institutes of Health Stroke Scale score, stroke cause, collateral grade, and degree of recanalization in a multivariable ordinal regression analysis (common OR, 2.54; 95% CI 1.22–5.31; P=0.013).
Discussion
This multicenter study shows that severe LA predicts a diminished chance of a good functional outcome after MT using stent-retriever devices for AIS. In addition, severe LA is an independent risk factor for FR and mortality at 90 days in multivariable analysis. However, no association was found between severe LA and sICH in univariate analysis.
In the present study, only 18.4% of the patients with severe LA achieved a good functional outcome after MT with stent-retriever devices. Our data is consistent with a previous study in 129 patients with AIS undergoing endovascular therapy, including 37 patients treated with stent-retriever devices, showing a good functional outcome rate of 14% in the presence of severe LA (VSS≥3), and establishing LA severity as an independent predictor of poor 90-day outcome.14 However, in contrast to our study, a recent analysis of 56 AIS patients found no significant association of LA burden on FLAIR images with AIS outcomes after MT using stent-retriever devices.8 These findings may relate to differences in the characteristics of the study populations, as we excluded patients with minor stroke (NIHSS <8), in whom the benefits of mechanical thrombectomy are uncertain. Further, the role of LA in minor stroke patients remains unclear. For example, Onteddu et al15 reported that severe LA (VSS≥3) in minor ischemic stroke patients (NIHSS ≤5) was an independent predictor of a worse functional outcome, while Zerna16 found no association of LA burden on MRI with disability at 90 days (mRS score 2–6) in transient ischemic attack or minor stroke (NIHSS ≤3) patients in multivariable analysis. Further studies are required to determine the specific contribution of LA to functional outcome after minor ischemic stroke, especially in patients receiving MT. In addition, the study by Atchaneeyasakul et al8 included 56 cases with FLAIR images from 136 consecutive AIS patients receiving MT, which may have created a potential bias and was likely underpowered to detect clinical differences.
The mechanisms by which LA affects poststroke outcome remain poorly understood. There is evidence that LA is associated with microcirculatory disturbances,17 18 and thus may have a detrimental effect on cerebral collateral circulation,19 and be related to larger infarct cores13 or infarct growth20 after ischemic stroke. In addition, LA is associated with increased platelet activation21 and hypercoagulability.22 Activated platelets and fibrinogen may occlude capillary and noncapillary sectors, contributing to focal ‘no-reflow’ (loss of microvascular patency),23 an important factor associated with FR. In the present study, we found severe LA was a significant predictor for FR. Our data confirm the results of a previous study, reporting that moderate-to-severe LA (VSS≥2) was independently associated with FR in AIS treated by MT.24 Moreover, LA may be relevant for neurorehabilitation after stroke. White matter integrity, a well established component of stroke functional recovery,25 26 may be impaired in individuals with a higher LA load.27 On the other hand, LA is also a robust predictor of cognitive dysfunction after ischemic stroke,28 29 which may impair the capacity of patients to learn and implement the treatment programs in rehabilitation.
Consistent with the study by Atchaneeyasakul et al,8 we found that LA severity was not associated with sICH. However, Shi et al7 reported contrasting findings, whereby moderate or severe LA (on FLAIR images) in the deep white matter was correlated with intracranial hemorrhage in AIS patients treated with Meric devices. The Meric device may be associated with a higher rate of intracranial hemorrhage,30 which may account for these differing results. Therefore, our results suggest that severe LA may not be a contraindication for MT with stent-retriever devices, as the complication of sICH is likely unrelated to LA severity.
The major limitation of the present study is the retrospective design, which may lead to information and selection bias. Another possible limitation is the use of VSS to assess the extent of LA on CT, which is less accurate than volumetry using MRI (although this may be less applicable in clinical practice). CT is still widely used to evaluate stroke patients, and VSS is broadly approved as a visual rating tool. Finally, the protocol criteria for MT may vary between different centers and periods based on the development of clinical evidence or guidelines. The strength of our study includes the multicenter analysis with a relatively large sample size, blinded imaging assessment, and systematic ascertainment of clinical patient characteristics.
Conclusions
This multicenter study showed that severe LA may be a relevant risk factor for poststroke outcome after MT using a stent-retriever device. Our data may be used cautiously by clinicians to better evaluate the expected prognosis of MT in patients with LA. These results need confirmation in larger prospective analyses.
References
Footnotes
YG and WZ contributed equally.
Contributors YG, YW, WZ: study design, primary manuscript writing, tables, and figure. YG, WZ, SZ: data acquisition and image analysis. BS, XS, SL, YB, ZL, DZ: data acquisition. WZ, XL: critical revision and final approval of the manuscript.
Funding This work was partly supported by National Natural Science Foundation of China grant number 81530038 and 81501193, Natural Science Foundation of Jiangsu Province grant number BE2016748, and National Key Research and Development Program grant number 2017YFC1307901.
Competing interests None declared.
Patient consent Not required.
Ethics approval Ethics committee of each participating center.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional material is published online only.