Article Text

Abstract
Background and purpose Hemorrhagic transformation (HT) is a complication that may cause neurological deterioration in patients with acute ischemic stroke. Various radiological subtypes of HT can be distinguished. Their influence on functional outcome is currently unclear. The purpose of this study was to assess the associations between HT subtypes and functional outcome in acute ischemic stroke patients with proven large vessel occlusion included in the MR CLEAN trial (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic stroke in The Netherlands).
Methods All patients with follow-up imaging were included. HT was classified on follow-up CT scans according to the European Cooperative Acute Stroke Study II classification. Functional outcome was assessed using the modified Rankin Scale (mRS) 90 days after stroke onset. Ordinal logistic regression analysis with adjustment for potential confounders was used to determine the association of HT subtypes with functional outcome.
Results Of 478 patients, 222 had HT. Of these, 76 (16%) patients were classified as hemorrhagic infarction type 1, 71 (15%) as hemorrhagic infarction type 2, 36 (8%) as parenchymal hematoma type 1, and 39 (8%) as parenchymal hematoma type 2. Hemorrhagic infarction type 2 (adjusted common OR (acOR) 0.54, 95% CI: 0.32 to 0.89) and parenchymal hematoma type 2 (acOR 0.37, 95% CI 0.17 to 0.78) were significantly associated with a worse functional outcome. Hemorrhagic infarction type 1 and parenchymal hematoma type 1 were not significantly associated, although their point estimates pointed in the direction of worse outcome.
Conclusion This study suggests that parenchymal hematoma type 2 is relevant for functional outcome after an acute ischemic stroke, and smaller HTs might also influence long term functional outcome.
Trail registration number ISRCTN10888758.
- hemorrhage
- stroke
- thrombectomy
- thrombolysis
- complication
Statistics from Altmetric.com
Introduction
Hemorrhagic transformation (HT) manifests as natural progression of acute ischemic stroke (AIS) or a complication of thrombolytic treatment1 2 and can cause neurological deterioration.1 With the recent introduction of endovascular treatment (EVT) as standard of care in AIS, the effect of HT on outcome has gained increased interest.3–7 Based on the radiological appearance, HT is categorized as hemorrhagic infarction (HI) or parenchymal hematoma (PH).8 Both types have been subdivided into small and large subtypes (suffixes 1 and 2, respectively). Some hemorrhages cause acute neurological deterioration and are classified as symptomatic intracranial hemorrhage (sICH). No significant differences in the incidence of sICH between patients treated with and without EVT have been observed.3–7 The incidence of HT in these patients has not been reported. In most sICHs the underlying hemorrhages are large.8 9 Therefore, it has been suggested that the patient’s well being is not influenced by the small hemorrhage subtypes, HI1, HI2, and PH1.10 Some studies even suggest that HI is associated with better functional outcome than patients without HI because it is a sign of early revascularization.11 12 However, as some patients with HI show acute neurological deterioration, the impact of HI on functional outcome might be underestimated.13 Even though, most patients with HI do not show acute neurological deterioration, it could still have a negative impact on long term functional outcome.14
The main purpose of this study was to determine the incidence of HT and assess the association between subtypes of HT and functional outcome, approximately 90 days after stroke onset in the MR CLEAN trial population (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic stroke in The Netherlands).3
Methods
MR CLEAN was a prospective, multicenter, randomized clinical trial that assessed the efficacy and safety of EVT compared with usual treatment in patients with AIS in The Netherlands. Patients with a proximal intracranial large vessel occlusion of the anterior circulation who could be treated within 6 hours after symptom onset were included in MR CLEAN. The MR CLEAN design and outcomes have been previously presented in detail.3 15
A central medical ethics committee and the research boards of all participating centers accepted the MR CLEAN trial. Written informed consent was obtained from all patients or their legal representative.
In this post hoc analysis, all patients with follow-up imaging were eligible for inclusion. HT was classified according to the European Cooperative Acute Stroke Study II (ECASS II) classification.8 Hemorrhagic infarction 1 (HI1) was defined as small petechiae along the margins of the infarct; hemorrhagic infarction 2 (HI2) as confluent petechiae within the infarcted area but no space occupying effect; parenchymal hematoma 1 (PH1) as blood clots in 30% or less of the infarcted area with some slight space occupying effect; and parenchymal hematoma 2 (PH2) as blood clots in more than 30% of the infarcted area with substantial space occupying effect.8 HT was identified by two experienced observers from the core imaging committee. Patients with any ICH and neurological deterioration (increase of 4 points on the National Institute of Health Stroke Scale (NIHSS)) were classified as sICH.3
Follow-up imaging acquired at approximately 5 days was examined to reduce the chance of contrast staining being classified as HT. When 5 day follow-up imaging was not available, 24 hour follow-up imaging was used for classification of HT. HI rates at 24 hour and 5 day follow-up imaging were compared to detect possible overestimation of HI due to contrast staining. Functional outcome was defined according to the modified Rankin Scale (mRS) assessed at 90 days (±14 days) after AIS onset. The mRS is a score to assess functional outcome and ranges from 0 to 6, where 0 indicates ‘no symptoms’ and 6 ‘death’.
Statistical analysis
HT was divided in four groups; HI1, HI2, PH1, and PH2.8 The effect of HI1, HI2, PH1, and PH2 on functional outcome, with no HT as the reference level, was assessed using multivariable ordinal logistic regression analysis. Functional outcome was assessed on the full mRS at 90 days. Differences in outcome between subgroups were estimated as a common OR, which summarizes the shift in the direction of a better outcome on the mRS. Common ORs <1 signify a shift in the direction of worse outcomes. Adjustment for potential confounders included diabetes mellitus, systolic blood pressure, intravenous thrombolysis (IVT), EVT, time from onset to randomization, history of ischemic stroke, age, atrial fibrillation, and follow-up lesion volume. Follow-up lesion volume was determined using a validated automated measurement including both the infarct and hemorrhage volume.16 Additionally, we report the median follow-up lesion volume for all HT subgroups. The association of sICH with full scale functional outcome was analyzed separately using ‘no sICH’ as reference. As it is highly likely that acute neurological deterioration in patients with sICH was caused by hemorrhage and these hemorrhages are mostly large, we adjusted for the same potential confounders as mentioned above, excluding follow-up lesion volume.
As a secondary outcome we dichotomized mRS (mRS 0–2 vs 3–6) and assessed the association of HT with good functional outcome (mRS 0–2) using multivariable logistic regression. We adjusted for the same potential confounders as the primary analysis.
Due to death, decreased kidney function, or insufficient scan quality, there were no analyzable 24 hour follow-up CT angiographs to evaluate recanalization rate for 96 patients. With the large amount of missing values, we chose not to include recanalization rate in the multivariable analysis. Recanalization rate is very important to functional outcome and although we adjusted for EVT and IVT, which are the two major factors causing recanalization, we conducted a sensitivity analysis with the patients for which recanalization rate could be assessed.
Patient characteristics were compared using the Χ2 test for trend for categorical data, one way ANOVA for normally distributed continuous data, and the Kruskal–Wallis test for non-normally distributed continuous data. The statistical analysis was performed using R (R Core Team (V.3.4.2 (2017); R: A language and environment for statistical computing, R Foundation for Statistical Computing, Vienna, Austria; used packages rms,17 ggplot2,18 and tableone19).
Results
Twenty-two patients were excluded because of missing follow-up imaging due to death. Of the remaining 478 patients, 361 (76%) had follow-up CT imaging at approximately 5 days. For 117 (25%) patients, 24 hour follow-up CT was assessed. Of all included patients, 222 patients had HT (46%); 16% HI1 (n=76), 15% HI2 (n=71), 7.5% PH1 (n=36), and 8.2% PH2 (n=39). Baseline characteristics were evenly distributed between all groups except for NIHSS score (P=0.002), atrial fibrillation (P=0.003), systolic blood pressure (P<0.001), and follow-up lesion volume (P<0.001) (table 1). HI rates did not differ between 24 hour and 5 day follow-up imaging. Thirty-six patients were classified with HI on 24 hour CT scans (31%) and 111 patients on 5 day follow-up CT scans (31%).
Patient characteristics
Primary outcome
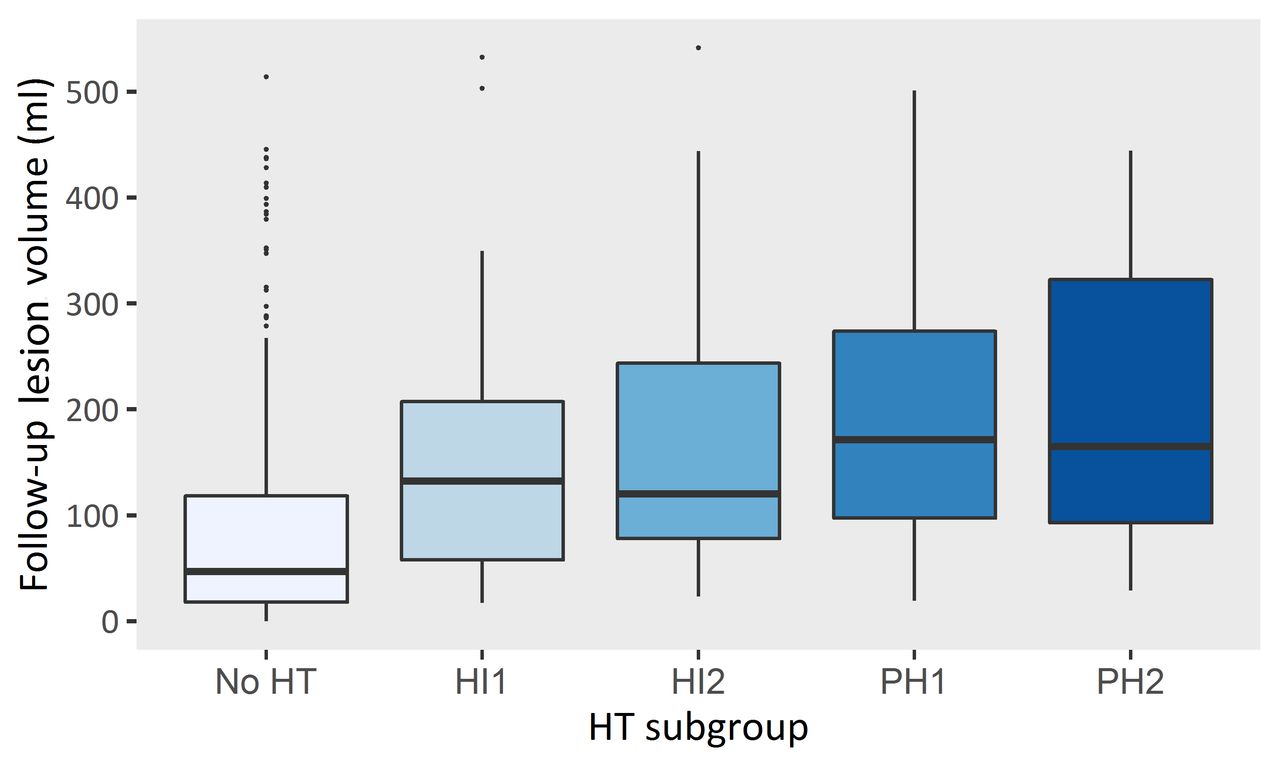
The mRS distribution for the individual HT subtypes is shown in figure 1. Twenty-three (66%) of the 35 patients with sICH died. For HI1, HI2, PH1, and PH2, these rates were 17%, 28%, 19%, and 46%, respectively. In patients without HT, 18% died. None of the patients with any HT had a score of 0 on the mRS. After adjustment for potential confounders, PH2 and HI2 were significantly associated with a worse functional outcome (adjusted common OR (acOR) 0.37, 95% CI 0.17 to 0.78 and 0.54, 95% CI 0.32 to 0.89, respectively). For HI1 and PH1, the point estimates also were in the direction of worse outcome but were not statistically significant (table 2). Patients with HT had larger lesion volumes than patients without HT (P<0.001) figure 2).
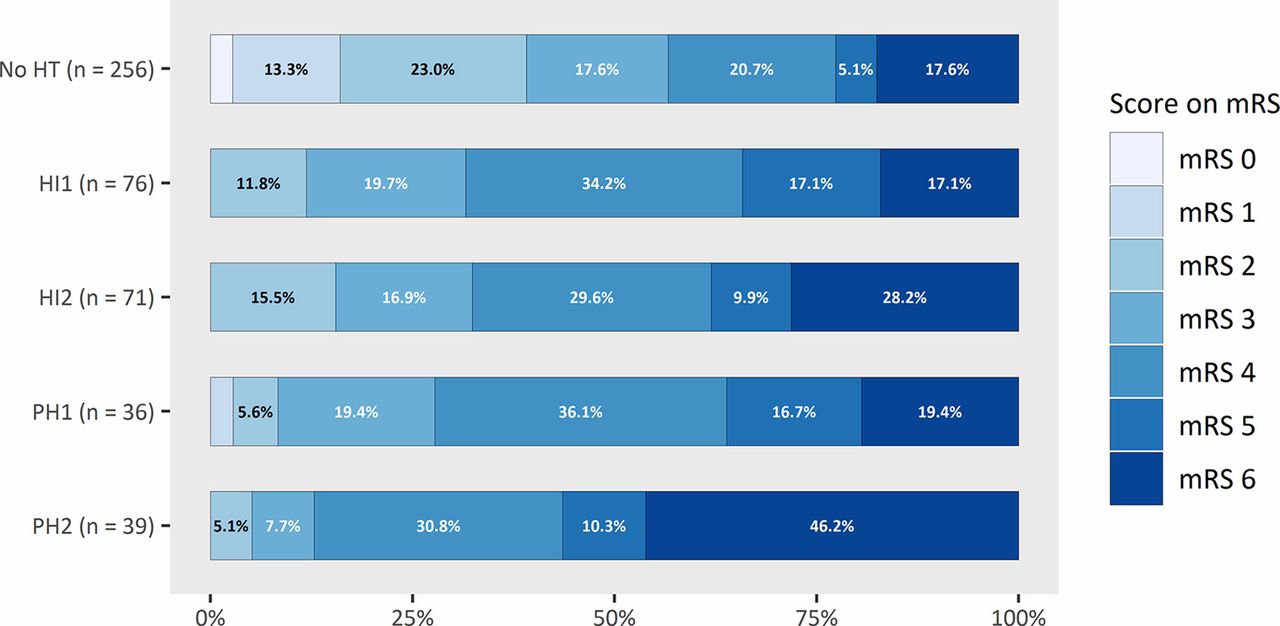
Functional outcome defined by the modified Rankin Scale score per group. HI, hemorrhagic infarction; mRS, modified Rankin Scale HT, hemorrhagic transformation; PH, parenchymal hematoma.
Adjusted and unadjusted ORs of the association of hemorrhage with functional outcome
{kind=link}
{kind=link}
Follow-up lesion volume per group. Follow-up lesion volume includes hemorrhage and infarct volume. Patients with any subtype of hemorrhagic transformation (HT) have larger lesion volumes than patients without HT (P<0.001). HI, hemorrhagic infarction; PH, parenchymal hematoma.
Of the patients with sICH, 28 had PH2 (80%), 2 had PH1 (5.7%), 2 had HI2 (5.7%), 1 had HI1 (2.9%), and 2 patients had a subarachnoid hemorrhage (5.7%). Both patients with symptomatic PH1 died, as did one of the patients with symptomatic HI2. The other patient with symptomatic HI2 had a moderately severe disability (mRS 4) as did the patient with symptomatic HI1. Two patients with sICH due to PH2 underwent hemicraniectomy. Of the 37 patients with PH2, 27 were classified as sICH (73%). Patients with sICH had a strong association with a worse functional outcome (acOR 0.17, 95% CI 0.08 to 0.35).
Secondary outcome
In the adjusted analysis of the association of HT with functional outcome on a dichotomous scale, only HI1 (acOR 0.35, 95% CI 0.13 to 0.85) and PH2 (acOR 0.22, 95% CI 0.03 to 0.96) were significantly associated with a poor functional outcome (table 2). HI2 and PH1 were not significantly associated with this secondary outcome measure.
Recanalization rate
In the sensitivity analysis in which recanalization rate was included in the analysis, in the analysis using the full mRS scale, HI2 (acOR 0.37, 95% CI 0.21 to 0.67) and PH2 (acOR 0.21, 95% CI 0.08 to 0.53) were significantly associated with a worse functional outcome. In the analysis using the mRS as dichotomous scale, HI1 and PH2 were significantly associated with a poor functional outcome (aOR 0.34, 95% CI 0.12 to 0.90 and aOR 0.15, 95% CI 0.02 to 0.70, respectively) (table 2).
Discussion
In our patient group, there was a high incidence of HT. HI1, HI2, and PH2 were significantly associated with worse functional outcome compared with patients without HT. However, point estimates for all types of HT were in the direction of worse functional outcome. After adjusting for revascularization rate, the results largely did not change and showed comparable point estimates as the analysis without adjustment for revascularization rate. Patients with PH2 had the largest adverse effect on functional outcome and higher mortality than patients with HI1, HI2, or PH1.
Only a few studies have reported an association of HI1 or HI2 with functional outcome. Nogueira et al reported a significant association of HI and PH with worse functional outcome.20 Further, Dzialowski et al reported that HI2, PH1, and PH2 were significantly associated with worse functional outcome compared with patients without HT.14 Other studies did not find an association of HI or PH1 with worse functional outcome.9–12 21–24 This difference might be explained by smaller sample sizes in some studies11 12 22 24 or by a lower incidence of HT compared with our study.9 10 23 Treatment with IVT might be the reason for this difference in incidence because IVT increases the risk of developing HT.25 26 In our population, 90% of patients received IVT whereas these rates were much lower in other studies.9 10 23 Additionally, the high incidence of HT in our study might be explained by the broad inclusion criteria of the MR CLEAN trial. Patients with early signs of infarction on CT indicating severe strokes were not excluded, in contrast with other studies with a lower incidence of HT.9 10 23
As large infarct volumes are associated with worse functional outcome and with HT, a large underlying infarct could drive an observed association of HT with functional outcome.10 Therefore, we adjusted for final lesion volume. However, it should be noted that this necessary adjustment for lesion volume might lead to underestimation of the association of HT with functional outcome. First, because follow-up lesion volume and HT are identified on the same follow-up CT, it may be complicated to separate them statistically. Also, lesion volume includes infarct volume and hemorrhage. However, it is difficult to separate the impact of infarct volume and HT on functional outcome since the infarct size of patients with PH2 is masked by hemorrhage and therefore its size cannot be determined.
Depending on the outcome measure (ie, dichotomized or full mRS) both HI1 and HI2 were significantly associated with poor functional outcome. Additionally, all point estimates were in the direction of poor functional outcome for patients with any HT. This might indicate that both HI1 and HI2 could have a negative influence on functional outcome compared with patients without HT. However, due to the alternating statistical significance it is difficult to determine their actual influence on functional outcome.
HI1, HI2, and PH2 were significantly associated with poor functional outcome. In contrast, PH1 was not significantly associated with poor functional outcome. This might be explained by the small number of patients in the PH1 group, combined with less adverse outcomes compared with the similarly common PH2. The point estimate, however, indicated an association with poor outcome.
In the newly proposed Heidelberg classification, HT is defined as HI1, HI2, and PH1. In this classification, PH2 is classified separately from HT, as the radiological entity PH2 appears to be distinctly different, and because of the assumption that only PH2 is clinically relevant.27 Our study suggests otherwise. While patients with PH2 are likely to show acute neurological deterioration in contrast with patients with other subtypes of HT, we found that PH2 was not the only condition relevant for functional outcome. The smaller subtypes of HT were associated with worse functional outcome after approximately 90 days of stroke onset and should therefore be considered relevant for functional outcome.
There are a few limitations of this study. First, this was a post hoc analysis of a randomized trial that was not designed to determine an association of HT with functional outcome. Therefore, the results should be interpreted with caution. Second, not all 5 day follow-up CT scans were available. In 117 cases, 24 hour CT scans were used to identify HT. It is possible that some of the patients who were identified with HT on a 24 hour CT had contrast staining which cannot be distinguished from a hemorrhage on conventional 24 hour CT scans. Although these patients with contrast staining have blood–brain barrier disruption, they might not all develop HT. Therefore, some patients might incorrectly be identified with HT while these patients had in fact contrast staining. This may have influenced the data in two different ways. First, the occurrence of HI might be overestimated. Second, patients with contrast staining might not develop any hemorrhage and therefore would not have impaired functional outcome, resulting in a more positive functional outcome for patients with HI. However, the rates of HI were not different between the 24 hour and 5 day CT scans.
In conclusion, we found that not only PH2 is relevant for functional outcome after AIS but smaller types of HT may influence functional outcome. However, it is difficult to determine their true impact on functional outcome. Future studies should focus on identifying patients with high risk characteristics and a suitable treatment that may reduce HT development. Treatment with thrombolytic agents is associated with an increased risk for HT. An upcoming trial (MR CLEAN-MED) that will randomize periprocedural antithrombotic drugs and aims to improve microvascular reperfusion might further improve our knowledge regarding HT risk.28 Additionally, other upcoming trials that will randomize treatment with thrombolytic agents (MR CLEAN-NO IV, SWIFT DIRECT, DIRECT-SAFE, and DIRECT MT) may clarify whether EVT alone will reduce the risk of HT and improve functional outcome after AIS.29–32
References
Footnotes
Contributors The MR CLEAN trial was designed by WHvZ, AvdL, RJvO, DWJD, YBWEMR, and CBLMM. OAB collected and prepared the data for the trial. OAB, AMMB, KMT, and KRvK prepared the data for this study. KRvK and KMT conducted the statistical analysis, interpreted the results, and drafted the paper. HAM assisted with the statistical analysis, interpretation of the results, and drafting the paper. AMMB, OAB, LAvdB, VC, HFL, WHvZ, AvdL, RJvO, DWJD, YBWEMR, and CBLMM critically revised the paper. All authors approved the version to be published.
Funding The MR CLEAN trial was partly funded by the Dutch Heart Foundation, grant No 2008T30, and by unrestricted grants from AngioCare BV, Medtronic/Covidien/EV3, MEDAC Gmbh/LAMEPRO, Penumbra Inc, Stryker, and Top Medical/Concentric.
Competing interests Academic Medical Center Amsterdam received funds from Stryker for consultations by CBLMM, YBWEMR, and OAB. CBLMM received research grants from CVON/Dutch Heart Foundation, European Commission, and Twin Foundation. HAM, AMMB, and CBLMM are shareholders of Nico.lab, a company that focuses on the use of artificial intelligence for medical image analysis. Erasmus MC received funds from Stryker for consultations by DWJD and AvdL, and Bracco Imaging for consultations by DWJD. Maastricht University Medical Center received funds from Stryker for consultations by WHvZ. WHvZ had speaking engagements with Stryker and Cerenovus.
Patient consent Obtained.
Ethics approval A central medical ethics committee and the research boards of all participating centers accepted the MR CLEAN trial.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Because of the sensitive nature of the data collected for this study, requests to access the data set may be sent to the MR CLEAN executive committee (https://www.mrclean-trial.org/).