Article Text

Abstract
Backround The treatment of wide neck bifurcation aneurysms remains challenging despite the introduction of new techniques (Y stenting, waffle cone technique, or flow diverter stents). The Woven EndoBridge (WEB) device is an innovative solution for this type of cerebral aneurysm. A new WEB 17 is now available and has been designed to offer smaller sized devices to optimize navigability and delivery.
Methods Between February 2017 and April 2018 all patients treated with the WEB 17 device in our center were retrospectively reviewed. 25 patients with 28 non-ruptured aneurysms were identified and analyzed. Three patients with two aneurysms both treated with the WEB device were identified.
Results The device was successfully deployed in all cases. Procedure related morbidity was 4% and mortality was 0%. In one case, a delayed postprocedural thromboembolic event occurred owing to device protrusion. Technical success, complications, angiographic outcomes, procedural data, and follow-ups are reported. The modified Rankin Scale score at discharge was 0 for 24 patients (96%). At the 3, 6, or 9 month follow-up, angiograms were taken of 21 of the 25 patients (84%) (24 of 28 aneurysms had been controlled); 3 patients (3 aneurysms) did not receive angiographic follow-up at the time of submission of this work. Complete occlusion was achieved in 22 of 24 aneurysms (91.66%), and 2 of 24 aneurysm (8.33%) showed a neck remnant.
Conclusions The WEB 17 is safe and technically feasible, according to this retrospective single center analysis. For very small bifurcation aneurysms, the WEB 17 seems to have lower complication rates than stent assisted techniques. However, further studies are needed to evaluate the complication rate and long term efficiency.
- aneurysm
- device
- intervention
- technique
Statistics from Altmetric.com
Introduction
Endovascular treatment (EVT) is now the firstline treatment for ruptured and unruptured aneurysms since the International Subarachnoid Aneurysm Trial (ISAT)1 and the Clinical and Anatomic Results in the Treatment of Ruptured Intracranial Aneurysms (CLARITY)2 study. Aneurysms with a complex anatomy (specifically, wide neck aneurysms) are in some cases untreatable or difficult to treat with standard coiling, balloon assisted coiling, stent assisted coiling, and flow diversion.3–5 The safety and efficacy of the self-expanding intra-aneurysmal flow disruptor, the Woven EndoBridge (WEB; Sequent Medical, Aliso Viejo, California, USA) device, has now been well described, and its use for the treatment of wide neck aneurysms has shown promising rates of adequate occlusion with low rates of morbidity and mortality6 7
The device has been progressively developed since 2010 from a dual layer version (WEB DL) to single layer versions (WEB SL and WEB SLS (single layer spherical)). Good clinical practice trials showed good safety and efficacy of the treatment with no mortality and 2.7% morbidity 1 month following treatment.8-11 In a recent meta-analysis, perioperative morbidity and mortality rates were 4% and 1%, respectively.12
However, the treatment of distal (M2–M3 segments) and small (<5 mm) unruptured complex bifurcation aneurysms remains challenging12 and often requires device assisted procedures, such as a balloon or stent.13 Owing to this fact, the procedure takes longer, which increases the rate of ischemic and hemorrhagic complications.
The new fifth generation WEB device (WEB 17) offers two notable technical improvements. First, the number of wires used for the new generation is lower compared with the old generation (72–108 vs 144–216) with no change in the visibility of the device on angiograms. This aspect allows much smaller devices to be used—the smallest device measures 3 mm in diameter and is 2 mm high (WEB SL 3×2 mm). Moreover, it allows better conformity to aneurysm shape and easy microcatheter navigability. The second improvement is a complete redesign of the pusher and diameter, downsizing from 0.020 inches to 0.015 inches. These improvements allows the WEB 17 device to be loaded into a 0.017 inch microcatheter (VIA 17). Thus the applicability of the device has increased tremendously as small bifurcation or side wall aneurysms can now be treated, and more distal locations can be attempted for treatment due to the better distal catheterization capacity of VIA 17.
In this study, we report our experience of treatment of unruptured aneurysms with the new WEB 17 system at a single center.
Methods
Patients
Between February 2017 and April 2018, 25 patients (15 women and 10 men; aged 20–74 years; median 54.5 years), who presented with 28 unruptured intracranial aneurysm, were retrospectively enrolled in this study in accordance with the guidelines of our institution. All patients with unruptured aneurysms were discussed in a meeting with neurologists, neurosurgeons, and neuroradiologists to define treatment procedures for each patient. This study was designated as a clinical audit, and no ethics committee review was required.
Treatment technique
Endovascular treatment was performed on a biplane angiographic system (AlluraClarity; Philips Healthcare, Best, The Netherlands). Antiplatelet agents were administrated before EVT for all patients (aspirin and ticagrelor) in accordance with our institutional protocol. All procedures were carried out under general anesthesia and systemic heparinization. A single femoral puncture allowed the positioning of a long delivery catheter (Neuron Max 088, Penumbra, Alameda, California, USA) at the origin of the internal carotid artery or vertebral artery. Then a guiding catheter (Fargomax, Balt, Montmorency, France or Navien, Covidien, Irvine, California, USA) was advanced into the intracranial internal carotid artery or vertebral artery. After this, the microcatheter (VIA 17, Sequent Medical) was navigated into the aneurysm dome. Measurements were taken using three-dimensional rotational angiography (3DRA) to better chose the size of the WEB device. After the procedure, as per the institution’s protocol, Vaso-CT10 was used to analyze the WEB position. Antiplatelet agents were discontinued except in four cases owing to a small protrusion of the device inside the parent artery.
WEB sizing
We believe that choosing the correct size of WEB device is crucial for successful EVT. The WEB width (the primary measurement) should be a little larger (usually 1 mm) than the aneurysm to avoid any residual blood flow around the WEB. The height of the device should be a little smaller (usually 1 mm) than the aneurysm to avoid any distortion of the device (the +1/–1 rule).14 In six aneurysms (21.4%), the Vaso-CT control demonstrated that the initial choice of the size of the WEB device was not correct, and the device was replaced with a smaller one in two patients and with a larger device in four patients. This proves that sizing is still challenging in a notable proportion of patients, and is dependent on operator experience.
The WEB 17 is an electrothermally detachable device, and no complications occurred at the time of treatment in all cases.
Evaluation
Procedures
The WEB 17 device was successfully deployed in all cases. No intraprocedural rupture or thrombotic complications occurred.
Angiographic follow-up
Twenty-one of 25 (84%) patients (24 of 28 aneurysms had been controlled) received angiographic follow-up, a mean time of 6 months after surgery (range 3–12 months). DSA, which consisted of 3DRA and Vaso-CT, was performed in all but one patient.
Immediately before detachment of the device, a Vaso-CT image was taken to confirm the size and position of the WEB 17 device and the patency of the parent artery. If the device was well positioned with no occlusion of the parent artery, the device was detached. Subsequently, 21 patients with unruptured aneurysms had DSA and clinical analysis (modified Rankin Scale (mRS) score) at 3, 6, 9, and 12 months. The angiographic results were classified using the Raymond–Roy occlusion classification.15
Results
Twenty-eight unruptured aneurysms (12 middle cerebral artery aneurysms, 10 anterior communicating artery aneurysms, three T shaped carotid aneurysms, one posterior inferior cerebellar artery aneurysm, one basilar tip aneurysm, and one anterior choroid artery aneurysm) were treated with the WEB 17 devices in 25 patients.
The device was successfully deployed in all cases. Final angiograms showed no residual clotting or branch occlusion, and no clinical consequences were observed. No clinically relevant hemorrhagic complications occurred during hospitalization for any of the 25 patients. On discharge, patients were evaluated by mRS score. Procedure related morbidity was 4% and mortality was 0%. Technical success, complications, angiographic outcomes, procedural data, and follow-up controls were reported. mRS score at discharge was 0 for 24 patients (96%); one patient had an mRS score of 4 and experienced a delayed thromboembolic complication with ischemic stroke symptoms. Short term (3 month) and mid term (6, 9, and 12 month) angiographic follow-up was available for 21 patients with 24 aneurysms (84%); 3 patients with 3 aneurysms (16%) did not have angiographic follow-up at the time of writing. Complete occlusion was achieved in 22 of 24 aneurysms (91.6633%), and 2 aneurysm (8.33%) had a neck remnant. No aneurysm remnant was noticed.
In one case, the device was undersized for an unruptured anterior communicating artery aneurysm, and 5 days later the patient experienced an acute ischemic stroke. On the angiographic image, the device was protruding into the right A2 segment. Our team decided to place a FRED Jr 2.5×18 mm stent between the right A1–A2 segments, but the stent collapsed owing to poor radial force, and re-catheterization of the device was not possible. Even though the contralateral carotid angiogram showed good collateral flow by leptomeningeal anastomoses of the left anterior cerebral artery, the patient developed a notable ischemic lesion in the right frontal lobe. At the 6 month follow-up appointment, this patient presented with a left-sided deficit (mRS=4) and partially thrombosed aneurysm (classified as an aneurysm remnant).
In three patients (patient Nos 1, 9, and 23), the operator chose to treat two aneurysms in the same procedure, as shown in figures 1 and 2. Owing to short procedure times and the low complication risks of this technique, treating two aneurysms in the same session is more feasible than with other EVTs .

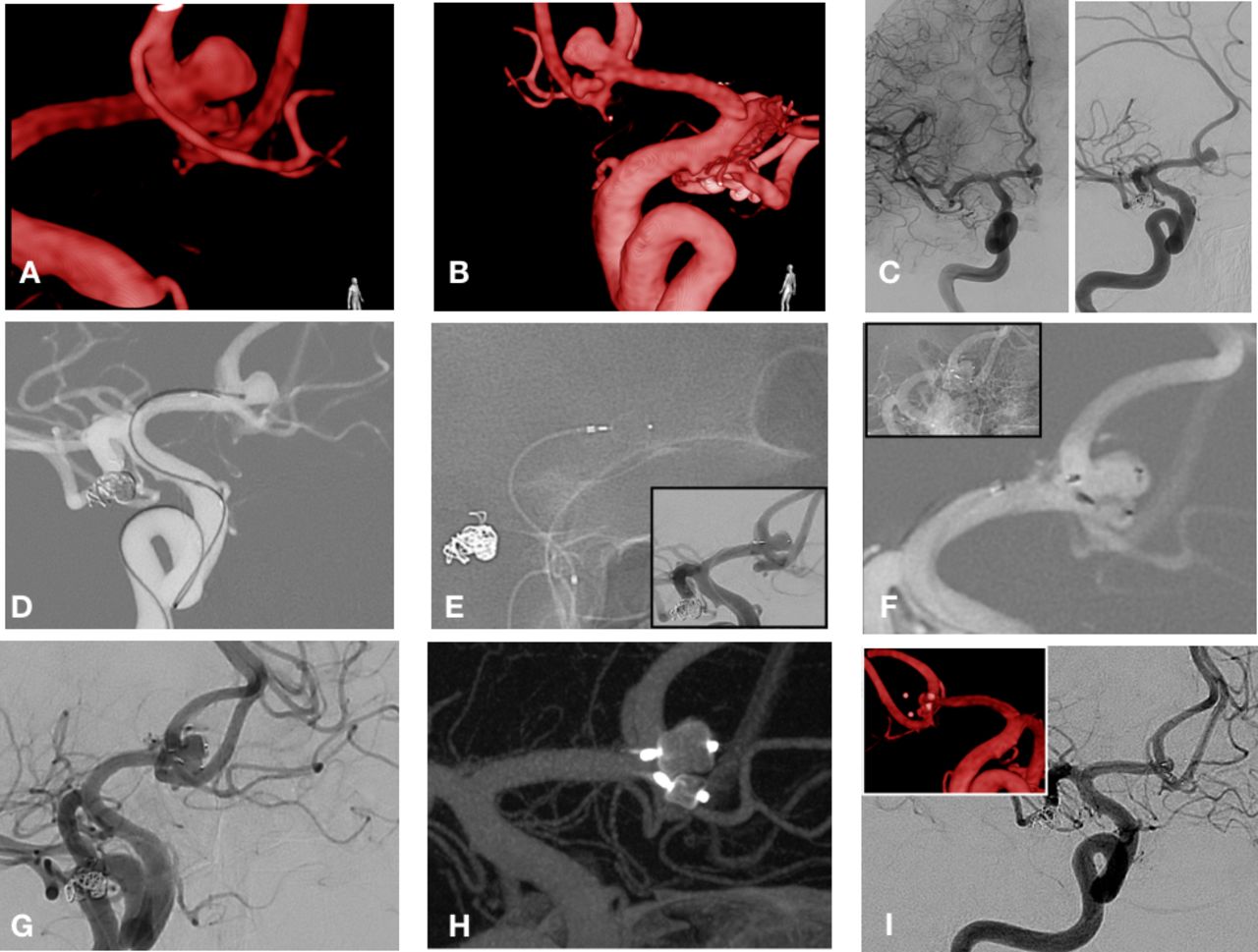
Patient No 1: right middle cerebral artery aneurysm and right T carotid. (A) Three-dimensional rotational angiography work projection measuring the size of the aneurysm; first aneurysm (height × dome) 3.5×4.5 mm; second aneurysm 3.3×2.5 mm. (B) DSA internal carotid artery (ICA) right work projection. (C) Unsubtracted image of the deployment of the first Woven EndoBridge (WEB) SL (4.5×2 mm). (D) DSA image after first deployment of the WEB SL (4.5×2 mm). (E) Catheterization of the ICA aneurysm. (F) Unsubtracted image of the deployment of the second WEB SL (3×2 mm; not detached) and the first WEB SL (4.5×2 mm). (G) DSA image of the WEB devices in place. (H) Vaso-CT taken immediately after detachment. (I) DSA image taken at the 6 month follow-up, showing total occlusion (TO).

Patient No 9: bi-lobed anterior communicating artery aneurysm. (A) Three-dimensional rotational angiography oblique plane image (first lobe: (height × dome) 4×3mm and second lobe 3×2mm). (B) Three-dimensional rotational angiography posterior–anterior image. (C) DSA posterior–anterior view and work projection. (D) VIA 17 microcatheter inside the first sac. (E) Unsubtracted image of deployment of the first Woven EndoBridge (WEB) SL (4.5×3 mm); DSA control image shown in the inset. (F) Deployment of second WEB SL (3×2 mm). (G) DSA image taken immediately after deployment of both WEB SL devices. (H) Vaso-CT taken immediately after detachment. (I) DSA image taken at the 3 month follow-up (three-dimensional rotational angiography image: total occlusion (TO)).
Discussion
One of the main advantages of the WEB 17 device is the easier and more distal navigation with the VIA 17 microcatheter compared with the more rigid VIA 27 microcatheter. The VIA 17 microcatheter is preferable for treatment where the anatomy is more difficult to treat, such as sharp angled carotid siphons and especially anterior communicating aneurysms. The smallest size of WEB 17 available (WEB SL 3×2 mm) up to WEB SL 7×5 mm or WEB SLS 7 mm, can be loaded in a VIA 17 microcatheter; the WEB SL has an oblong shape and the SLS is spherical.
Unsheathing and deploying the WEB 17 in the aneurysm is smooth, and recapturing is easy with less pulling force needed than old generation WEB devices.
The possibility to treat aneurysms as small as 3 mm in diameter with the WEB 17 device proved less technically complicated than stent assisted coiling or Y stenting coiling techniques.
Poly-lobed aneurysms are usually challenging to treat by balloon assisted coiling or even stent assisted coiling. Here, one bi-lobed anterior communicating artery aneurysm was treated by placing a WEB 17 device in each aneurysm lobe, as shown in figure 2. We strongly believe that this technical approach is useful in this type of aneurysm, providing higher feasibility and safety than other techniques.
The WEB 17 design, which has fewer wires, has two important morphologic characteristics compared with older generation devices, such as the WEB 21. First, the new device has weaker structural memory, and deployment in angulated aneurysms within the bifurcation can be challenging. Second, the device is more susceptible to deformation by pushing or pulling forces, and the shape at the neck can be affected, meaning neck remnant may occur immediately after first deployment. In both cases the necessity of device repositioning by a second deployment is mandatory and in our institution is validated by Vaso-CT protocol imaging after each deployment.
Devices measuring between 4 and 7 mm diameter can be loaded in either VIA 17 or VIA 21 microcatheters depending on operator preference. In all cases reported here, only VIA 17 microcatheters were used. In cases where devices of 6 mm or 7 mm in diameter were used, no device incompatibility was noticed.
Our study presents several limitations, especially concerning its retrospective nature and the small number of patients, which makes statistically significant results difficult.
The second limitation is the lack of long term follow-up, although we reported 91.66% total occlusion rate, which is similar to other studies.15 We are aware of the limited number of patients enrolled in this retrospective analysis and also the small number of long term (24 months or more) follow-ups. The adequate occlusion rate and flow disruption seemed to be similar between the older and newer generation WEB devices, but this needs further prove when more long term data are available (figure 3).
{kind=link}
{kind=link}
{kind=link}
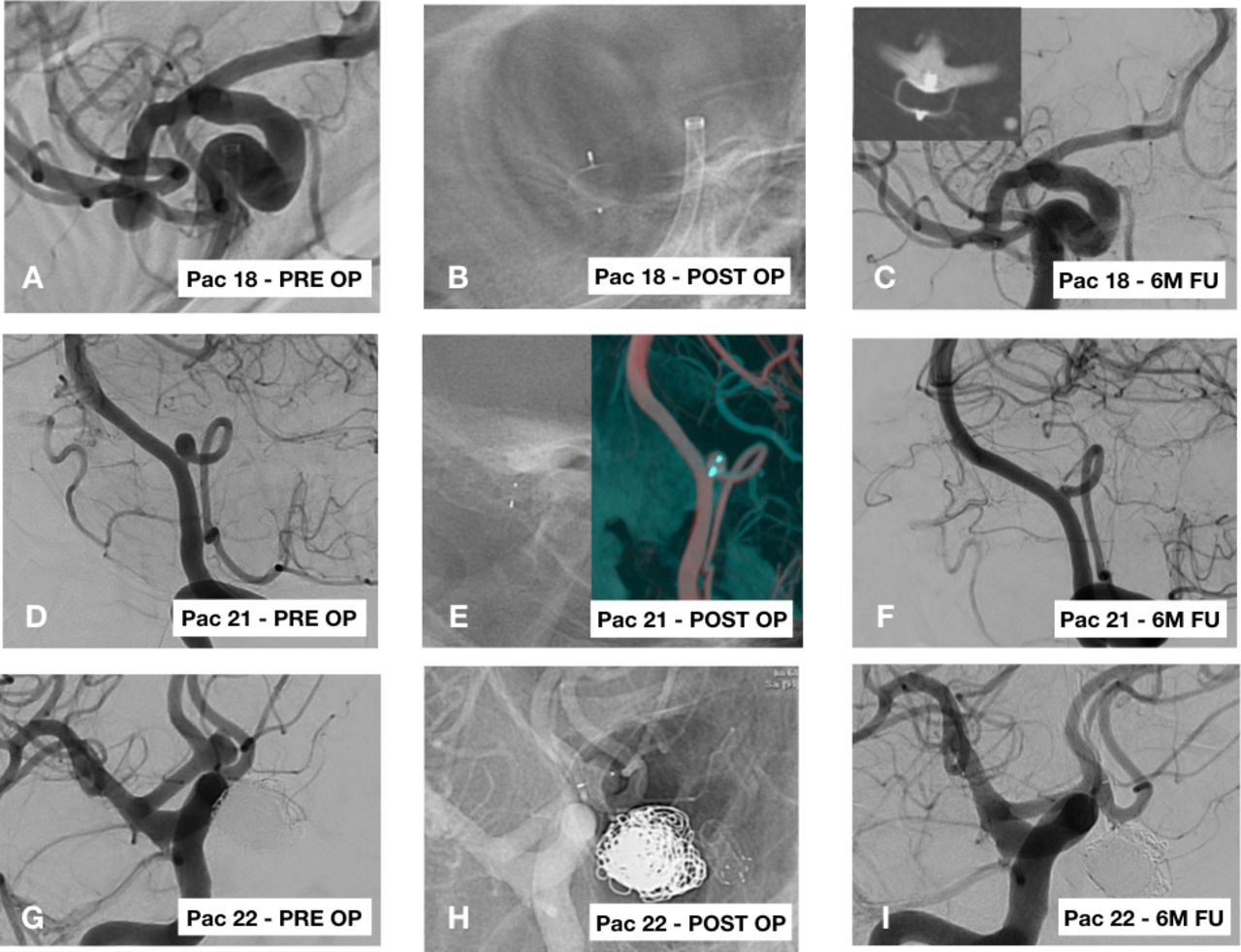
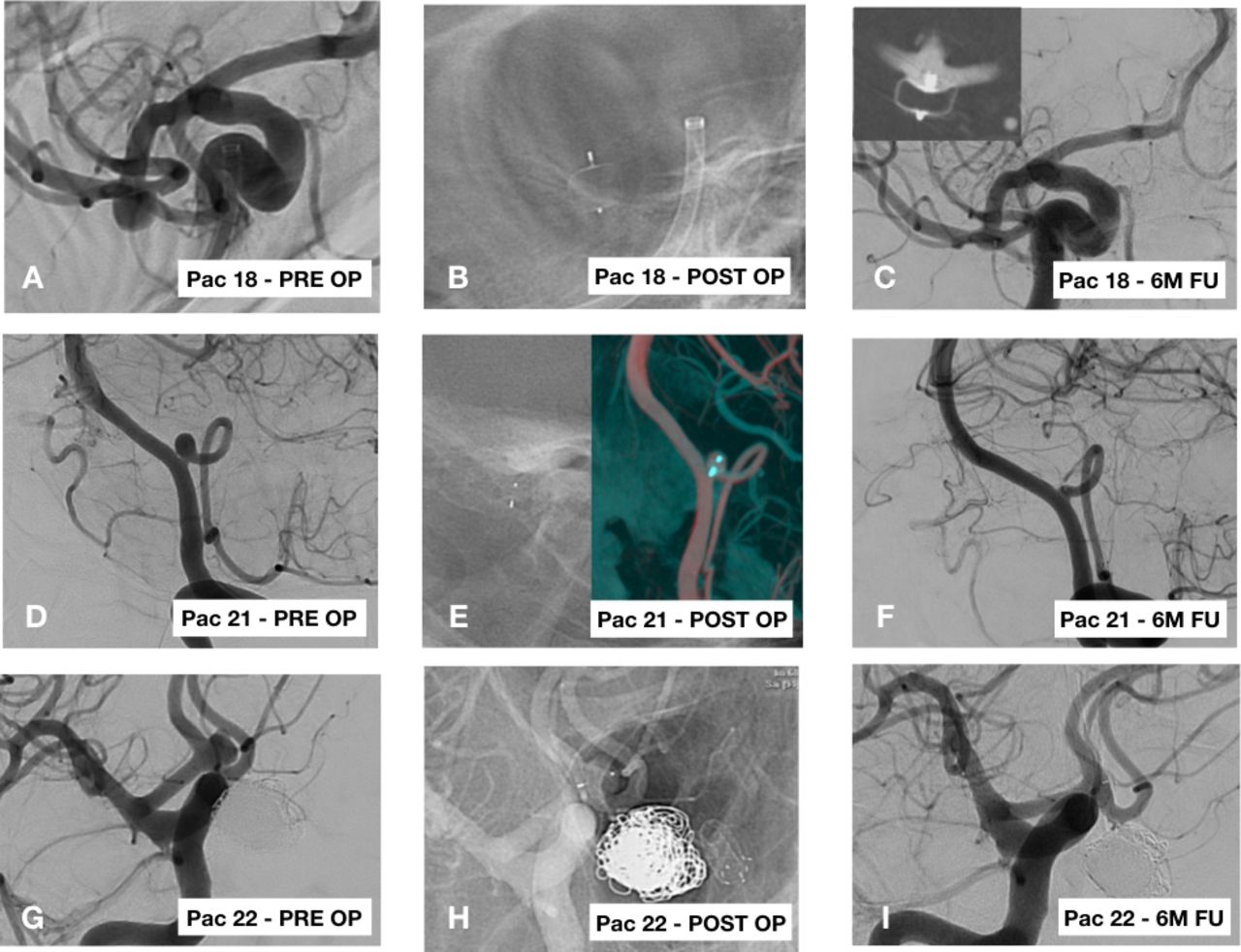
Patient No 18: right middle cerebral artery (MCA) aneurysm. (A) DSA work projection. (B) Unsubtracted image after deployment of the Woven EndoBridge (WEB) SL 6×3mm. (C) DSA and Vaso-CT at the 6-month follow-up (FU) DSA. Patient No 21: left posterior inferior cerebellar artery aneurysm. (D) DSA work projection. (E) Unsubtracted and Vaso-CT image after deployment of the WEB SL 4.5×3 mm). (F) DSA at the 6 month follow-up. Patient No 22: anterior communicating artery. (G) DSA work projection. (H) Unsubtracted image after deployment of the WEB SL 5×2 mm. (I) DSA at the 6 month follow-up: total occlusion (TO).
Conclusion
This preliminary study suggests that the newer generation of WEB 17 device is highly feasible for EVT of unruptured wide neck aneurysms. For very small bifurcation aneurysms, the newer generation of WEB devices seem to be safe and feasible solutions for this challenging type of aneurysms. However, further studies are needed to evaluate the complication rate and long term efficacy of WEB 17 devices in the treatment of these aneurysms.
Supplementary file 1
References
Footnotes
Contributors All authors have contributed equally to this work. CM, JC, IP, LI, GBH, SN, VC, and HP: substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of the data for the work. TY, JMD, MI, AO, and SG: drafting the work or revising it critically for important intellectual content. AR, BVP, SP, JM, and LS: final approval of the version to be published. CM, JC, and IP: agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice Since this paper was first published online, Pr has been removed from the author names Sorin Pescariu, Jacques Moret and Laurent Spelle.