Article Text

Abstract
Background The Pipeline Embolisation Device with Shield technology (PED-Shield) is suggested to have reduced thrombogenicity. This reduced thrombogenicity may make it possible to use safely in the acute treatment of aneurysmal subarachnoid haemorrhage (aSAH) on single antiplatelet therapy (SAPT).
Objective To evaluate the safety and efficacy of the off-label use of PED-Shield with SAPT for the acute treatment of aSAH.
Methods Patients who underwent acute treatment of ruptured intracranial aneurysms with the PED-Shield with SAPT were retrospectively identified from prospectively maintained databases at three Australian neurointerventional centres. Patient demographics, aneurysm characteristics, clinical and imaging outcomes were reviewed.
Results Fourteen patients were identified (12 women), median age 64 (IQR 21.5) years. Aneurysm morphology was saccular in seven, fusiform in five, and blister in two. Aneurysms arose from the anterior circulation in eight patients (57.1%). Six (42.9%) patients were poor grade (World Federation of Neurological Societies grade ≥IV) SAH. Median time to treatment was 1 (IQR 0.5) day. Complete or near complete aneurysm occlusion (Raymond-Roy <3) was achieved in 12 (85.7%) patients at the end of early-acute follow-up (median day 7 after SAH). Permanent, treatment-related morbidity occurred in one (7.1%) patient and one (7.1%) treatment-related death occurred. The use of a postoperative heparin infusion (n=5) was associated with a higher rate of all complications (80.0% vs 11.1%, p=0.023) and symptomatic complications (60% vs 0.0%, p=0.028). No symptomatic ischaemic or haemorrhagic complications were observed in the patients who did not receive a post-operative heparin infusion. Nine (64.3%) patients were functionally independent on discharge from the treatment centre.
Conclusion The PED-Shield may be safe to use in the acute treatment of ruptured intracranial aneurysms with SAPT. Further investigation with a formal treatment registry is needed.
- aneurysm
- hemorrhage
- stent
- stroke
- platelets
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Endovascular management of ruptured intracranial aneurysms is well established.1 However, broad-necked saccular, fusiform or blister aneurysms pose specific challenges for conventional endovascular treatments. These aneurysms may also pose challenges for microsurgical clipping.2 Few options are available for the safe and effective treatment of this subpopulation of ruptured intracranial aneurysms. In these aneurysms, the use of stent-assisted coiling or flow diversion may be a viable treatment strategy.3 4 However, there is understandable resistance to the use of intravascular stents for subarachnoid haemorrhage, owing to the risks of thromboembolic and haemorrhagic complications.5 Dual antiplatelet therapy (DAPT) reduces the risk of the former at the cost of increasing the risk of the latter.6–8
A surface modified flow-diverter stent, (Pipeline Flex with Shield Technology, Medtronic Neurovascular, Irvine, California, USA) has been introduced. The PED-Shield has 3 nm of phosphorylcholine covalently bound to the braid wires. Phosphorylcholine is a major constituent of red blood cell membranes and has been shown to reduce platelet adhesion and activation.9 The PED-Shield has demonstrated significantly reduced surface thrombus formation compared with the unmodified PED-Flex.10 These preliminary data suggest that it might be possible to use the PED-Shield off-label with single antiplatelet therapy (SAPT) in the acute treatment of ruptured intracranial aneurysms.
Previously, our group described the first successful example of the PED-Shield used for the acute treatment of a ruptured intracranial aneurysm with SAPT.11 We report here our further experience using this technique in a total of 14 cases across three centers. We discuss changes to our original approach and describe our current protocol as the basis for further investigation.
Methods
Prospectively maintained databases at three Australian neurointerventional centers were retrospectively interrogated from July 2015 (corresponding to the release of PED-Shield) to September 2018. Patients with aneurysmal subarachnoid haemorrhage (aSAH) who underwent PED-Shield placement under aspirin cover within 5 days of ictus, either for flow diversion or stent-assisted coiling, were identified.
All patients underwent routine cerebral DSA, including three-dimensional (3D) rotational angiography, at the time of admission. The decision to offer endovascular therapy was based on consensus between the on-call neurointerventionist and the on-call open neurosurgeon on the day of admission. The dose and timing of aspirin therapy were at the discretion of the operator as was the use of intraoperative heparin and GPIIb/IIIa inhibitors as a one-off dose . Postoperative heparin infusion was allowed; however, the addition of a P2Y12 inhibitor or further GPIIb/IIIa inhibitor within the first 7 days postoperatively was considered treatment failure. Patients with a history of P2Y12 inhibitor use before surgery were excluded. The timing and modality of postoperative imaging were dependent on the operator’s preference and the clinical status of the patient. All patients were admitted to the intensive care unit after treatment.
Basic patient demographic data—aneurysm size, location, number and size of PED-Shields used, use of coiling, clinical outcomes, and imaging data—were collected. Aneurysm occlusion was recorded with conventional DSA. A non-contrast CT brain scan was used to assess for evidence of ischaemia in the target vessel territory and perforator territory in the postoperative period within 7 days of ictus whenever possible. The follow-up period was defined as the first 7 days after SAH (early-acute), which avoids the peak vasospasm period potentially confounding results. After this point, the decision to withhold a P2Y12 inhibitor was reassessed based on the ongoing haemorrhage risk. Clinical outcomes were assessed at discharge from the treatment centre.
Differences between categorical variables were assessed using Fisher’s exact test and continuous variables with Wilcox rank sum test. Comparisons with a published meta-analysis of patients with aSAH treated with flow diverters while receiving DAPT12 were made with the t-test and Z-test for two populations. All statistical analysis was performed in RStudio (RStudio, Inc, Boston, Massachusetts, USA).
Results
Baseline patient and aneurysm characteristics
Fourteen patients were identified who fulfilled the selection criteria. The median age was 64 (IQR 21.5) years, and 12 patients (85.7%) were female. Three patients were current smokers, and a further patient had a smoking history. Three patients (21.4%) had a history of regular aspirin use before ictus. The median Fisher grade was IV. The median World Federation of Neurological Societies (WFNS) grade was 2.5 (42.9% WFNS ≥IV). Aneurysms were located in the anterior circulation in eight patients (57.1%). Aneurysm morphology was saccular in seven (50%), fusiform in five (35.7%) and blister in two (14.3%). The mean aneurysm size was 8.8 mm. Aneurysms involved the internal carotid artery-first segment of the middle cerebral artery (ICA-M1) in three (21.4%), the vertebral artery in three (14.3%), the posterior inferior cerebellar artery (PICA) in two (14.3%), and the A1/2 junction in two (14.3%) patients. Further aneurysms were located at the anterior communicating artery, the posterior communicating artery, the anterior choroidal artery, and the A2 artery in one patient each (table 1).
Baseline characteristics
Treatment
The median time from ictus to treatment was 1 (IQR 0.5) day. External ventricular drains (EVDs) were placed before surgery in eight patients (57.1%). Two patients (14.3%) required an EVD within the first 7 days after treatment, and one patient (7.1%) was treated with serial lumbar puncture. Two patients (14.3%) were preloaded with aspirin, and two patients were loaded with aspirin immediately postoperatively. The remaining 10 (71.4%) patients were loaded intraoperatively at a dose of 500 mg IV in nine (64.3%) and 600 mg via nasogastric tube in one. Intraoperative heparin was administered in six patients (42.9%), and five of these had a postoperative heparin infusion. A single intraoperative IV dose of the GPIIb/IIIa inhibitor, abciximab, was administered in five patients (35.7%) at a median dose of 10 (IQR 4) mg. An average of 1.2 (SD 0.7) PED-Shield devices per patient were implanted. PED-Shield deployment was successful in all 14 patients. The devices were placed in the M1-ICA in five (35.7%) patients, the vertebral artery in four (28.6%) patients, and the A1/2 in two (14.3%) patients. Devices were placed in the posterior inferior cerebellar artery in one, the anterior communicating artery in one, and the A2 in another patient. Adjunctive coil embolization was performed in 12 (85.7%) patients. Immediate aneurysm occlusion (Raymond-Roy 1) was achieved in seven (50.0%) patients with three patients (21.4%) achieving almost total occlusion (Raymond-Roy 2). No instances of intraoperative stent thrombosis, platelet aggregation, or haemorrhage were identified, and no other operative complications were recorded (table 2).
Operative characteristics
Outcomes
All patients underwent early follow-up imaging (median day 7 after SAH). Digital subtraction angiography (DSA) was used in 13 (92.9%) and CT angiography in the remaining patient. Complete stent thrombosis was identified in one (7.1%) patient at SAH day 2, PED-Shield day 1. This was treated successfully with endovascular thrombectomy. No further symptomatic ischaemic events were observed in the early-acute follow-up period. No asymptomatic stent occlusions were seen at follow-up imaging. No clinical or imaging evidence of perforator strokes was identified. Minor, non-flow-limiting platelet aggregation was noted on the PED-Shield of 2 (14.3 %) patients at follow-up imaging. These patients were judged to be at low risk of haemorrhagic complications or further intracranial procedures and treatment was started with a P2Y12 inhibitor without incident (SAH days 8–9). There was no association with smoking history (p=0.506), postoperative heparin infusion (p=1.0), or posterior circulation (p=0.473). No patients crossed-over to DAPT in the early-acute period (up to day 7 after SAH). Complete or near complete aneurysm occlusion (Raymond-Roy grades 1 and 2) was confirmed at early-acute follow-up imaging in 12 patients (85.7%). Aneurysmal rebleeding occurred in two (14.3%) patients in the early-acute period. This caused one death. The second patient made a full recovery. Both patients had unsecured aneurysms (Raymond-Roy 3) and received a heparin infusion postoperatively. Three patients died (21.4%) before acute hospital discharge, one patient from aneurysmal rebleeding and two from medical complications (hospital-acquired pneumonia). Mortality was associated with older patients (p=0.029).
Treatment-related complications and antiplatelet protocol
In total, three symptomatic (21.4%) and two asymptomatic (14.3%) complications were observed. The permanent treatment-related morbidity was 7.1% and mortality 7.1%. The use of a heparin infusion postoperatively (first five patients) was associated with all complications combined (80.0% vs 11.1%, p=0.023) and symptomatic complications (60.0% vs 0.0%, p=0.028). In the patients who did not receive a postoperative heparin infusion one asymptomatic complication (11.1%, asymptomatic platelet aggregation at early-acute follow-up) occurred and no symptomatic complications. In the most recent five patients a twice daily aspirin dosing protocol has been used. No symptomatic or asymptomatic complications have been recorded in these patients (table 3).
Complications by postoperative antiplatelet protocol
Comparison with the reference population
The meta-analysis of the use of flow diverters with DAPT in aSAH by Cagnazzo and colleagues was used as a reference population. This meta-analysis included 20 studies and 223 patients12 Our study included older patients (mean age 63.0 vs 53.3, p=0.038), more women (85.7% vs 34.0%, p<0.001), and more saccular aneurysms (50.0% vs 18.8%, p=0.005) than this reference population. Patients in our study were also treated more acutely than in the meta-analysis (mean number of days between SAH and treatment 1.4 vs 6.7, p<0.001), were more likely to have adjunctive coiling (85.7% vs 19.0%, p<0.001), and more likely to achieve immediate aneurysm occlusion or near occlusion (Raymond-Roy 1 and 2: 71.4% vs 32.0%, p=0.007). No statistically significant difference was seen between the two studies for stent thrombosis (7.1% vs 4.0%, p=0.342), permanent treatment-related morbidity (7.1% vs 7.0%, p=1.0), and treatment-related mortality (7.1% vs 4.5%, p=0.342) (tables 4 and 5).
Comparison of patient and aneurysm characteristics with those reported by Cagnazzo et al 12
Comparison of outcomes with Cagnazzo et al
Discussion
We report here the operative, and early-acute outcomes in a series of aneurysmal subarachnoid haemorrhage patients with complex ruptured aneurysms treated acutely, off-label, with the PED-Shield device with SAPT. The data is limited, however, as the protocol has matured the rate of complications with the use of PED-Shield with SAPT has reduced. This technique requires further study, however, may provide a valid treatment option for complex ruptured aneurysms.
The International Subarachnoid Aneurysm Trial established endovascular surgery as a first-line treatment for ruptured intracranial aneurysms.13 However, specific morphologies, such as blister, fusiform, and wide-necked aneurysms pose significant challenges both for endovascular and open microsurgical treatment. In an elective setting, such aneurysms have been successfully treated using stent-assisted coiling techniques and flow diversion. However, the use of intravascular stents, and, in particular, the high metal-density flow diverters, requires the use of DAPT to prevent stent thrombosis and ischaemic complications. This, in turn, increases the risk and severity of haemorrhagic complications in patients with acutely ruptured aneurysms.8 The phosphorylcholine coating of the PED-Shield device has been shown to reduce platelet adhesion and activation.9 In animal studies, PED-Shield with SAPT showed both reduced thrombus formation and increased endothelialization compared with PED-Flex.10 14 Interestingly, in an ex vivo model, PED-Shield with SAPT had similar thrombogenicity to PED-Flex with DAPT.15 Therefore, there is experimental evidence to support the use of PED-Shield with SAPT in extreme circumstances.
Previous studies have reviewed stent-assisted coiling in the treatment of ruptured aneurysms with DAPT and reported an overall complication rate of ~10–45%. In these series, thromboembolic and haemorrhagic complications were relatively evenly distributed.16–20 A meta-analysis of the use of flow diverter stents with DAPT in aSAH has recently been perforemd by Cagnazzo et al. 12 When our current study was compared to this meta-analysis, no statistically significant difference was seen in acute stent thrombosis, permanent morbidity, or mortality . Our patients were more likely to have saccular aneurysms, which were shown to have higher rates of haemorrhagic and ischaemic complications in the meta-analysis.12 In addition, patients in our study were treated significantly earlier and were more likely to achieve immediate aneurysm occlusion or near occlusion (see tables 4 and 5). This suggests at least a theoretical advantage of the current technique. Many operators prefer to delay aneurysm treatment when DAPT is required to minimise the need for additional intracranial procedures such as EVD placement. These preliminary results suggest this may not be necessary when using PED-Shield with SAPT. This may reduce the risk of aneurysm rebleeding before surgery. This early rebleed risk is unlikely to be completely identified in the retrospective case series which currently dominate the literature.
Limitations
Our study has several inherent limitations, which should be considered while interpreting the results. This is a multicenter, retrospective, observational study and, as such, has inherent selection bias. Selection bias is seen in the clinical severity of the patients studied and the complexity of the aneurysms. This bias is only natural given the lack of evidence surrounding the use of SAPT with PED-Shield. When this technique is used, patients should have no other viable alternatives. These data are considered preliminary and further investigation is necessary.
Protocol advice
The small numbers in this study may preclude a detailed exploratory analysis; however, we can report our anecdotal experience and how our protocol has evolved. Whenever possible, we perform adjunctive aneurysm coiling to achieve acute aneurysm occlusion (Raymond-Roy 1). Initially, patients received both intraoperative heparin and a single dose of an intraoperative GPIIb/IIIa antagonist (abciximab). Both have now been replaced by intraoperative IV aspirin (500 mg). The postoperative heparin infusion was discontinued after the first five patients. This infusion has now been shown to have a statistically significant association with all complications. No symptomatic complications have been seen in the absence of postoperative heparin.
Recently, the concept of accelerated platelet function recovery21 has prompted a change to aspirin 100–150 mg twice daily given that stressful states such as SAH may drive increased platelet turnover. Since switching to twice daily aspirin dosing (n=5) no symptomatic or asymptomatic complications have been seen. Routine DSA is performed at day ~7– 10 and the need to continue to withhold the second oral antiplatelet agent is reconsidered based on angiography and the patients' clinical state. See Figure 1 for illustrative cases.
Conclusion
In this small series, the PED-Shield has been used to treat acutely ruptured intracranial aneurysms with SAPT in a clinically severe patient population with complex aneurysms. These early results compare reasonably with previous treatment strategies and suggest the need for further investigation of this technique with a formal treatment registry.
{kind=link}
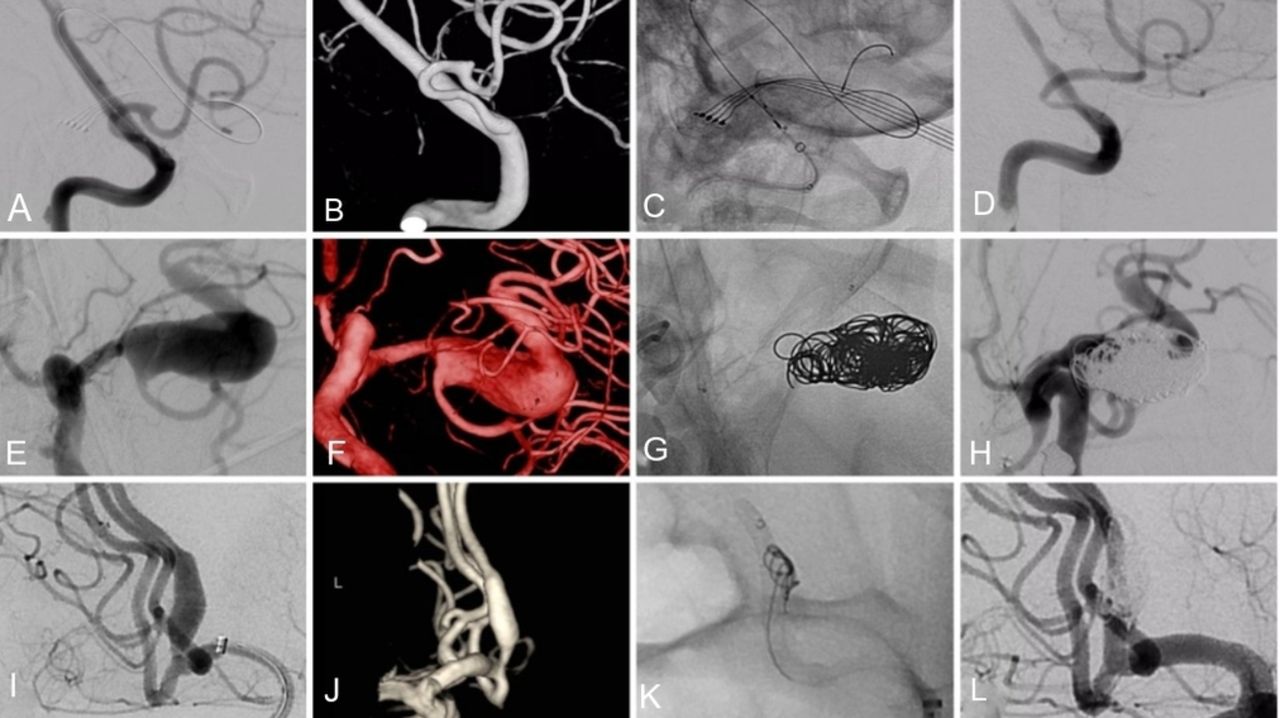
Illustrative cases. Ruptured right posterior inferior cerebellar artery (PICA) blister aneurysm (A–D). A balloon can be seen coming from the contralateral vertebral artery in the case of intraoperative rupture (A and C). The aneurysm is excluded at day 8 DSA with early vasospasm involving the PICA and vertebral artery (D). Ruptured giant, fusiform, left M1 aneurysm (E–H). Three-stent constructs deployed from distal M1 to the internal carotid artery with coiling. Proximal aneurysm body filling supplying posterior M2 (left intentionally) persists at the day 4 DSA (H). Ruptured fusiform A2 aneurysm (I–L). Single stent with adjunctive coiling. Aneurysm is completely excluded at day 8 DSA (L).
References
Footnotes
Contributors NWM was responsible for concept and design. All authors acquired and analyzed data. The manuscript was prepared by NWM and all authors reviewed and made critical revisions to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests NWM, AC, TJP, and JDW have been paid proctors and consultants for Medtronic Neurovascular. Medtronic is a provider of educational grants to the Prince of Wales Hospital Foundation.
Patient consent Not required.
Ethics approval University of NSW ethics board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data may be available on request. Requests should be directed to the corresponding author.