Article Text

Abstract
Background A transradial approach (TRA) is associated with fewer access site complications than a transfemoral technique (TFA).However, there is concern that performing mechanical thrombectomy (MT) via TRA may lead to longer revascularization times and thus worse outcomes. Nonetheless, TRA may confer added benefits in MT since navigation of challenging aortic arch and carotid anatomy is often facilitated by a right radial artery trajectory.
Objective To compare outcomes in patients who underwent MT via TRA versus TFA.
Methods We performed a retrospective review of our institutional database to identify 51 patients with challenging vascular anatomy who underwent MT for anterior circulation large vessel occlusion between February 2015 and February 2018. Patient characteristics, procedural techniques, and outcomes were recorded. TFA and TRA cohorts were compared.
Results Of the 51 patients, 18 (35%) underwent MT via TRA. There were no significant cohort differences in patient characteristics, clot location, or aortic arch type and presence of carotid tortuosity. There were no significant differences in outcomes between the two cohorts, including single-pass recanalization rate (54.5% vs 55.6%, p=0.949) and average number of passes (1.9 vs 1.7, p=0.453). Mean access-to-reperfusion time (61.9 vs 61.1 min, p=0.920), successful revascularization rates (Thrombolysis in Cerebral Infarction score ≥2b 87.9% vs 88.9%, p=1.0) and functional outcomes (modified Rankin Scale score≤2, 39.4% vs 33.3%, p=0.669) were similar between TFA and TRA cohorts, respectively.
Conclusions Our results demonstrate equivalence in efficacy and efficiency between TRA and TFA for MT of anterior circulation large vessel occlusion in patients with challenging vascular anatomy. TRA may be better than TFA in well-selected patients undergoing MT.
- technique
- stroke
- intervention
- artery
Statistics from Altmetric.com
Introduction
The transradial approach (TRA) for interventional procedures has been shown to decrease morbidity and mortality in comparison with the transfemoral approach (TFA) in multiple large prospective randomized controlled trials.1–7 Given the improved safety profile, and evidence that patients prefer TRA rather than TFA for interventional procedures, we have been increasingly using this technique at our institution for all neurointerventional procedures, with promising results.8–11
However, in cases of large vessel occlusion, the time to reperfusion is critical for decreasing the likelihood of long-term disability, and so it remains unclear whether TRA is associated with delayed reperfusion or worse outcomes than TFA.12 We recently reported a significant association between procedural length with tortuosity of aortic arch and internal carotid artery (ICA) in cases of TFA mechanical thrombectomy.13 We found that the transradial approach has a more favorable trajectory in patients with complex arches and significant tortuosity. Given our experience, patients with complex arches or significant tortuosity noted on initial stroke evaluation CT angiography are now treated primarily with TRA in our center. In this study, we present our recent experience with these patients with complex arches who underwent mechanical thrombectomy (MT) for anterior circulation large vessel occlusion via the transradial versus transfemoral approach, comparing revascularization times, procedural success, and patient outcomes.
Methods
Selection criteria
After approval from our institutional review board, we conducted a review of a prospectively maintained database of all patients with acute ischemic stroke who had undergone endovascular therapy by three primary operators at Jackson Memorial Hospital, Miami, Florida from February 2015 through February 2018. Patients with the following characteristics were excluded from analysis: posterior circulation large vessel occlusion, tandem occlusion of the ICA, patients who only underwent catheterization and angiography without thrombectomy, patients in whom both the aortic arch type and ICA dolichoarteriopathy could not be assessed with preoperative CT angiography (CTA), and patients who underwent access site crossover during thrombectomy (femoral to radial in one patient, or radial to femoral in two patients). Of note, tandem occlusion of the ICA was excluded as the treatments are generally more complex and routinely require increased procedural length, which may introduce confounding. In addition, tandem occlusions prevent adequate visualization and evaluation ICA dolichoarteriopathy on preprocedural CTA.
Preprocedural vascular imaging and B.A.D. score
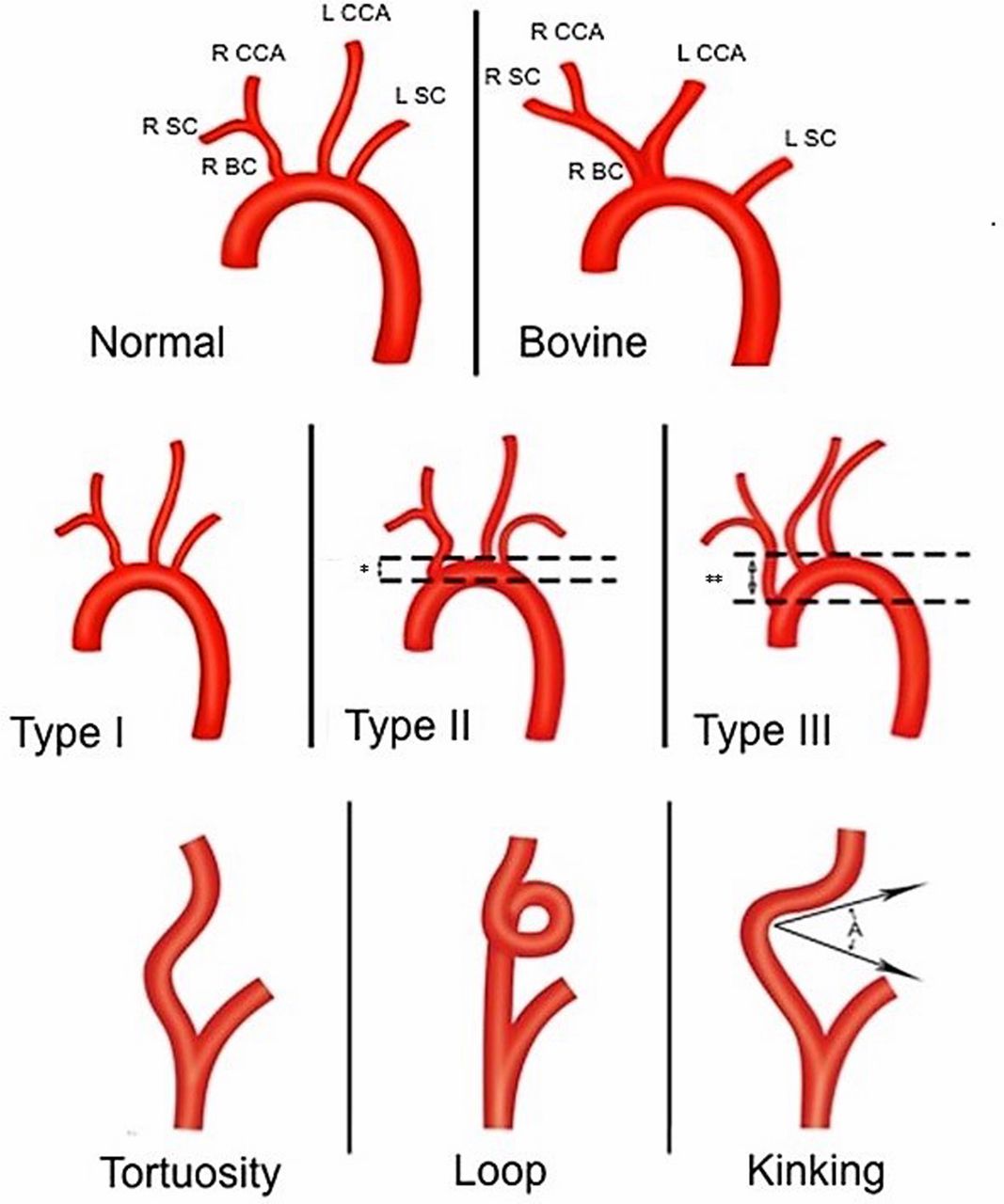
All cohort patients underwent CTA of the head and neck, including the aortic arch. Imaging was performed on a Siemen Somatotom Definition AS dual source spiral CT with an intravenous bolus of 100 mL of radiographic contrast agent administered via a power injector. Three-dimensional vessel reconstruction was performed at a control console immediately after completion of the combined injection and scanning. We have previously described the B.A.D. score as a predictor of time to revascularization and patient outcome after mechanical thrombectomy.13 The three important anatomical factors of this composite score are based on the preoperative imaging: (1) presence of a Bovine arch variant, (2) Aortic arch type, and (3) ICA Dolichoarteriopathy. One point is added for the presence of a bovine aortic arch variant in cases of a left-sided large vessel occlusion. The presence of a type I arch is 0 points, type II arch results in addition of 1 point, and type III arch 2 points. Patients with coiling, tortuosity, or kinking (30–90°) of the ICA ipsilateral to the side of the stroke receive an additional 1 point. Patients with a normal or mildly kinked ICA receive no additional points. High B.A.D. scores (2 or 3) were indicative of complex vascular anatomy and found to be associated with increased time to revascularization during transfemoral thrombectomy.13 TRA offers a more favorable trajectory in these patients and thus we sought to compare TRA with TFA in patients with B.A.D. scores ≥2 only. Two patients from the TRA cohort and 24 patients from the TFA cohort were excluded for B.A.D. scores of 0 or 1. Aortic arch anatomy, bovine variant common carotid origin, and ICA dolichoarteriopathy (tortuosity, kinking, coiling) are graphically depicted in figure 1.

{kind=link}
Graphic depictions of pertinent arch features with normal and bovine variant. Aortic arch ‘type I’; ‘type II’, and ‘type III’ are shown in the second row. If the distance between the innominate origin and the top of the aortic arch is one width or two widths of the CCA, then the arch is ‘type II’ (asterisk) or ‘type III’ (double asterisk), respectively. The third row depicts ICA tortuosity, coiling (or looping), and kinking. BC, brachiocephalic; CCA, common carotid artery; ICA, internal carotid artery; L, left; R, right; SC, subclavian. (Reprinted with permission from Snelling BM, Sur S, Shah SS, et al. Unfavorable vascular anatomy is associated with increased revascularization time and worse outcome in anterior circulation thrombectomy. World Neurosurg 2018:120:e976-83).
Endovascular procedure
Transradial access
At this time, we do not have a standardized protocol for decision to treat via TRA or TFA and choice of access is made on a case-by-case basis by the treating interventionalist. The right radial artery is always used for the TRA owing to simpler positioning and easier navigation of the catheters into the common and internal carotid arteries. Before puncture, Barbeau testing is performed to determine adequate ulnar collateral circulation to the hand.14 Patients with no return of plethysmography waveform after 2 min, or ‘Barbeau type D’, are excluded from receiving TRA. Ultrasound guidance is used to quickly measure the radial artery diameter and facilitate efficient access. A 6 French (F) short transradial introducer sheath (Glidesheath Slender, Terumo, Somerset, New Jersey) is placed and a radial angiogram obtained. Prophylactic spasmolytic agents (5 mg verapamil; 200 μg nitroglycerin) are given intra-arterially via the sheath after dilution in 20 mL of saline or blood aspirated from the sheath. Prophylactic intravenous heparin to prevent radial artery occlusion is not given during TRA MT owing to the risk of hemorrhagic conversion after stroke in the presence of low reported radial artery occlusion rates (4%) and negligible rates of hand ischemia.15
Various systems, based on preprocedural ultrasound radial artery diameter measurements, were used. In patients with smaller radial arteries, a 6 F Benchmark (Penumbra, Alameda, California, USA) or Envoy DA guide catheter (Codman Neuro, Raynham, Massachusetts, USA) is coaxially navigated into the target ICA over a 125 cm Simmons-2 shaped Select diagnostic catheter (Penumbra, Alameda, California, USA). The stent retriever is then deployed using standard procedure, and retrieved with manual aspiration of the guide catheter in the cervical ICA. For balloon guide plus stent retriever techniques, a 5 F Simmons-2 catheter is introduced into a 6 or 7 F sheath and used to navigate to the target ICA. Over an exchange length guidewire, the sheath and guide catheter are removed, and a 6 or 7 F Cello balloon guide (Medtronic, Irvine, California, USA) is brought into the ICA.
However, we found the catheter exchange technique to be cumbersome and slow compared with coaxial guide catheter placement, and thus our preferred technique in patients with radial arteries measuring at least 2.5 cm on preprocedural ultrasound was to use a 0.088" guide and an aspiration catheter. Access is performed using a 6 F Glidesheath Slender (Terumo, Somerset, New Jersey, USA) and the spasmolytic drugs are infused. A 3 mm J-wire is used to exchange the sheath for an 8 F Infinity guide catheter (Stryker Neurovascular, Kalamazoo, Michigan, USA), which is placed without a sheath into the radial artery and advanced to the subclavian artery. The stylet is then removed and a 125 cm Simmons-2 shaped Select catheter is navigated over a guidewire into the target ICA. The Infinity sheath is tracked over the Select catheter into the distal cervical ICA, and thrombectomy proceeds as previously described with instigation of continuous aspiration at the clot face just before unsheathing the stent retriever.16
Transfemoral access
A 9 F short guide sheath is placed in the femoral artery. A coaxial system consisting of a long diagnostic catheter and guidewire placed coaxially inside a 9 F balloon guide catheter (MERCI, Penumbra, Alameda, California, USA), Infinity guide catheter (Stryker, Kalamazoo, Michigan, USA), or rarely, a Neuron Max (Penumbra, Alameda, California, USA) is advanced into the target carotid artery. The diagnostic catheter is removed and a microcatheter with a microwire is introduced through the balloon guide catheter and navigated across the thrombus. The stent retriever device is deployed in a standard fashion and withdrawn after 5 min with the balloon inflated under fluoroscopy and manual aspiration during stent retrieval. In cases where mechanical aspiration is used, a coaxial system, consisting of our microsystem navigated through an intermediate catheter (Ace 68, Penumbra), is placed across the thrombus. The intermediate catheter is placed at the clot face and turned on just before unsheathing the stent retriever. The stent retriever is deployed for 5 min and removed under constant aspiration. Of note, early on in our MT practice, intra-arterial tissue plasminogen activator was often administered locally via the microcatheter in cases where multiple passes of the stent retriever were needed or the final result was not a Thrombolysis in Cerebral Infarction (TICI) score 3.
Statistical analysis
Data are presented as mean and SD for continuous variables, and as frequency for categorical variables. Analysis was carried out using unpaired t-test, Χ2, Fisher’s exact tests, and Levene’s test for detection of significant difference between radial and femoral access points. P values of ≤0.05 were considered statistically significant. Statistical analysis was carried out with SAS 9.4 (Cary, North Carolina, USA) and Python 3.7.
Results
Patient cohort
A total of 51 patients with a B.A.D. vessel score ≥2 underwent MT for anterior circulation large vessel occlusion from February 2015 through February 2018. The mean age was 78.3 years (range 44–93 years), and the majority of patients were female 66.7%. The average National Institutes of Health Stroke Scale (NIHSS) score on presentation was 15.9 (range 0–27). The M1 segment of the middle cerebral artery was the most common site of occlusion (53%), followed by M2 or M3 (33%) and then ICA terminus (14%). There were no significant differences between the radial and femoral cohort in patient characteristics, NIHSS score at time of presentation, location of large vessel occlusion, or each anatomical component comprising the B.A.D. vessel score (table 1).
Summary of patient and procedural characteristics by access site
Mechanical thrombectomy technique
Access was obtained via femoral artery puncture in 33 patients and radial artery puncture in 18 patients. A balloon guide catheter was used in 93.9% of TFA cases and only 33.3% of TRA cases (<0.0001). There was no difference in the number of cases in which mechanical aspiration through an intermediate catheter was employed (30.3% vs 33.3%, p=0.824). General anesthesia was also induced more often in TFA cases (54.5%) than in TRA cases (16.7%, p=0.0160) (table 1).
Summary of technical and clinical outcomes
Clinical outcomes
No significant differences in technical or clinical outcomes were found between two access technique cohorts. Intra-arterial recanalization was achieved after a single pass of the stent retriever in 54.5% of TFA cases and 55.6% of TRA cases (p=0.949). The average number of passes for TFA cases was 1.9 vs 1.7 in TRA cases (p=0.453). There was also no significant difference in mean time from groin or wrist puncture to reperfusion (61.9 vs 61.1 min, p=0.920) (table 2). A TICI score of ≥2b was considered a favorable radiographic outcome after mechanical thrombectomy. Successful revascularization was achieved in 87.9% of TFA patients and 88.9% TRA patients (p=1.0). There were no differences in post-thrombectomy radiographic hemorrhagic conversion or functional independence on discharge (modified Rankin Scale score ≤2).
Discussion
TRA has been widely adopted by interventional cardiologists, primarily owing to reduced access site complications. A Cochrane review of 31 randomized controlled trials comparing the TRA approach with TFA in acute coronary syndrome reported a significantly reduced rate of short-term net adverse clinical events, all-cause mortality, bleeding, and access site complications in the TRA cohort.17 Furthermore, the superficial and distal location of the radial artery confers the benefit of easy positioning, peripheral access, and reliable hemostasis. In patient preference studies, the majority of patients who underwent both methods, preferred TRA rather than TFA owing to rapid postprocedural mobilization, supination, and reduced access site discomfort.9 However, given the smaller size of the radial artery in comparison with the femoral artery, large-bore interventions such as MT, requiring the use of a triaxial system, may be more challenging. Given the critical timing in cases of large vessel occlusion, we sought to compare procedural times as well as clinical and angiographic outcomes in patients who underwent TRA versus TFA.
Several previous studies have demonstrated that complex aortic arch and carotid arterial anatomy is associated with increased technical difficulty and thus prolonged procedural times and complication rates.18–20 In our recent study of 95 patients who underwent a TRA for MT, we found that patients with complex aortic arch anatomy and ICA tortuosity as quantified by a B.A.D. vessel score was associated with significant increases in puncture to reperfusion times.13 While specialized catheters, such as the Simmons and Vitek catheters may facilitate carotid artery access through the TFA approach, the TRA approach offers more favorable trajectory for rapid access to the intracranial arteries, particularly in patients with a type II or III aortic arch, or bovine configuration of the left common carotid artery. Therefore, we hypothesized that a TRA could provide benefit in successful and efficient reperfusion compared with the standard TFA.
Our results are noteworthy for several reasons. First, no significant difference was seen in technical outcome or efficacy between transradial and transfemoral groups. Given the improved safety of the transradial approach, equivalence of technical and clinical success for neurological outcome implies significant benefit of the transradial approach over the standard transfemoral TFA, particularly if this finding can be replicated in larger studies across multiple arch anatomies.1–7
Second, there is a considerable learning curve associated with performing the TRA, and despite our interest in developing the transradial technique, all operators in this series were certainly more experienced and technically adept at MT via TFA.9 With further optimization and improvement, the potential for improving efficiency and efficacy of MT via TRA is significant. Our results here represent an early experience with transradial catheterization at our institution. Based on our previously published data on transradial angiography, improved technical success and efficiency are forthcoming.9
Finally, catheter and device selection is currently limited for the transradial approach. We have used a 6F system during radial artery access which limits our use of larger balloon guide catheters, which have been shown to be effective in MT. Furthermore, access catheters and guide systems have been designed for TFA primarily and there are no commercially available systems designed specifically for navigating the cervical and cranial vasculature via TRA at this time. With the advent of newer devices and technology, there is great potential for taking better advantage of the anatomical configuration of the great vessels approached via the right subclavian artery.
Limitations
This study has several limitations, including retrospective analysis of a prospective cohort. Although, to our knowledge, this is the first and largest reported series comparing TRA and TFA for MT, it included a relatively small number of patients with documented complex vascular anatomy who underwent either radial or femoral MT. Second, the decision to perform MT via the TRA versus the TFA was not randomized, introducing the possibility of selection bias. Additionally, the thrombectomy techniques were not standardized. It is possible that the differences in technique (use of balloon guide for most TFA cases, for example) have confounded the results. The functional status was also evaluated at discharge as many of the patients were lost to follow-up. While no patients had clinically significant symptomatic access complications, screening for asymptomatic radial artery occlusions was not routinely carried out. Furthermore, 30-day or more follow-up data were available for only 29 patients. Finally, there are differences in operator experience and technical equipment available between the transradial and transfemoral cohort as discussed above, which might have affected outcomes.
Conclusion
In this study, we found no significant differences in procedural or clinical outcomes in patients undergoing transradial versus transfemoral artery access for anterior circulation mechanical thrombectomy with difficult aortic arch and ICA anatomy. In well-selected patients, the TRA may be a safer and more efficient approach for mechanical thrombectomy after large vessel occlusion. However, further technological developments and studies are necessary.
References
Footnotes
Contributors All authors contributed to the conception, data collection, and drafting of this manuscript. RMS statistically analyzed the data. DRY, ECP, and RMS provided manuscript oversight and administrative support. All authors critically reviewed the manuscript and approved its final submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests BS is a shareholder in RIST Neurovascular. ECP is a consultant for Medtronic Neurovascular, Stryker Neurovascular, Penumbra, and Cerenovus, and is a stockholder in RIST Neurovascular. RMS is a consultant for Medtronic Neurovascular, Penumbra, Cerenovus, and Abbott.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.