Article Text

Abstract
Background The transradial approach as a frontline approach is a novel technique in neuroendovascular procedures. In this study we aim to present our early experience with full transition to transradial access as the first-line approach for neuroendovascular procedures.
Methods We prospectively collected data on the first 100 consecutive patients who underwent a diagnostic or interventional neuroendovascular procedure using the transradial approach at our institution between March 22 and April 30, 2019. Baseline characteristics were collected in addition to the type of procedure, access site, catheters and wires used, complications, and whether there was crossover to transfemoral access.
Results Transradial access was attempted in 121 cases and 91 cases were completed successfully (72 diagnostic procedures and 19 interventional procedures). Mean (SD) age was 56.8 (14.7) years, 54.9% (50/91) underwent the procedure in the outpatient setting, and 60.4% (55/91) were women. Seven patients had minor immediate complications related to the radial access. Interventional procedures successfully performed included aneurysm embolization (ruptured (n=3) and unruptured (n=8)), tumor embolization (n=2), cervical internal carotid artery stenting (n=2), balloon occlusion test (n=1), vertebral artery sacrifice (n=1), and arteriovenous malformation embolization (n=2).
Conclusion In this early experience, full transition to the transradial approach as the frontline approach is feasible with a low complication rate for both diagnostic and interventional neuroendovascular procedures.
- angiography
- catheter
- device
- guidewire
- technique
Statistics from Altmetric.com
Introduction
The transfemoral approach (TFA) has been the traditional frontline approach for neuroendovascular procedures given the accessibility, large diameter, and relatively straight angle of approach to the great vessels of the aortic arch. However, the transradial approach (TRA) has been used in interventional cardiology for more than three decades with greater patient comfort and a notably lower rate of access site complications, given its superficial location and compressibility.1–4 These features allow for local external compression that has largely supplanted vascular closure devices, leading to a reduction in the procedure-related cost.5–7 However, despite the widespread adoption of TRA in the cardiology community, the reported TRA case series in the neuroendovascular field have been limited to a few experienced centers.
In this study we aimed to assess the feasibility of a full transition to TRA for both diagnostic and interventional procedures over a short time course. In addition, we discuss in detail our procedural methods to facilitate the adoption of this technique in other institutions.
Methods
Setting
The neuroendovascular center at the Medical University of South Carolina (MUSC) is located in the south-eastern United States with an average of 1500 procedures a year (1000 diagnostic and 500 interventions). We prospectively collected data on the first 100 consecutive patients who underwent neuroendovascular procedures (diagnostic and interventional) using TRA at MUSC starting from the date of adoption of a radial-first approach (March 22, 2019). All the procedures were done by two operators (AMS and JRL) from March 22 to April 30, 2019. Both operators had minimal prior experience with TRA as it was used as a rescue technique for patients who fail TFA (one case every 1–2 years).
Exclusion criteria
We excluded patients with the following criteria4: (1) known vasoocclusive disease such as Raynaud disease, Takayasu arteritis, or thromboangiitis obliterans; (2) known complex radial or brachiocephalic anatomy such as aberrant right subclavian artery or situs inversus; (3) thrombectomy patients. We did not attempt TRA for thrombectomy cases during the study period because our upfront modality in stroke thrombectomy is A Direct Aspiration, First Pass Technique (ADAPT), for which we use a Neuron Max 088 (Penumbra, California, USA) as the guide sheath to accommodate either a 0.068 inch, 0.071 inch, or 0.072 inch aspiration catheter. This requires an 8 French access sheath, which currently limits its applicability to radial approaches (as 7 French is the maximum recommended radial sheath size).
Procedural protocol and technique
Patients rested in a supine position with the arm extended beside the torso during the procedure. TRA was attempted using ultrasonography. Historically, Allen’s or modified Allen’s test has been described for assessing collateral circulation of the hand, but has recently been demonstrated to be unnecessary so our protocol did not involve performing this test.8 9 Vascular access was achieved through the right radial artery except in two cases: (1) a basilar artery aneurysm embolization where the left vertebral artery was dominant, so the access was done through the left radial artery; and (2) a case with a known small radial artery from a prior TRA attempt, so the access was done through the right ulnar artery. The preference for using the right radial artery was because our angiography table and room set-up favors the right-sided approach for operator comfort. A 21-gauge needle (Cook Medical, Indiana, USA) and a Benston wire guide (Cook Medical) were used to obtain access under ultrasound guidance using the traditional Seldinger technique (through-and-through puncture).10 A 4/5 French Slender sheath (Terumo, New Jersey, USA) was used for diagnostic procedures and a 5/6 French Slender sheath (Terumo) was used for interventional procedures. In patients who had an arterial line for continuous hemodynamic monitoring already in place in the right radial artery (n=2), the arterial line was exchanged over a wire for a 6/7 French Slender sheath. At the conclusion of the procedure, an arterial line was replaced over a wire for ongoing hemodynamic monitoring post-procedure.
All patients who had successful radial access were administered 5 mg verapamil intra-arterially and 3000 units of heparin intravenously immediately after obtaining the access. The only exception were those patients with an indwelling arterial line in place; in these instances, the verapamil was administered prior to performing the wire exchange for the arterial sheath. A control angiography of the radial artery was performed after obtaining access in all cases and an additional 5 mg of intra-arterial verapamil was given if radial artery spasm was encountered (n=9). Interventional cases received intermittent boluses of intravenous heparin to maintain an activating clotting time of 2–2.5 times the patient’s baseline.
Hemostasis post-procedure was achieved using a TR BAND (Terumo) inflated with 15–18 mL of air, then titrated to stop the bleeding with preserving the radial pulse. We used the reversed Barbeau’s test to confirm the radial artery patency following the placement of the TR BAND.11 All patients were examined following the procedure and prior to discharge, and all of them had a palpable pulse at the site of access.
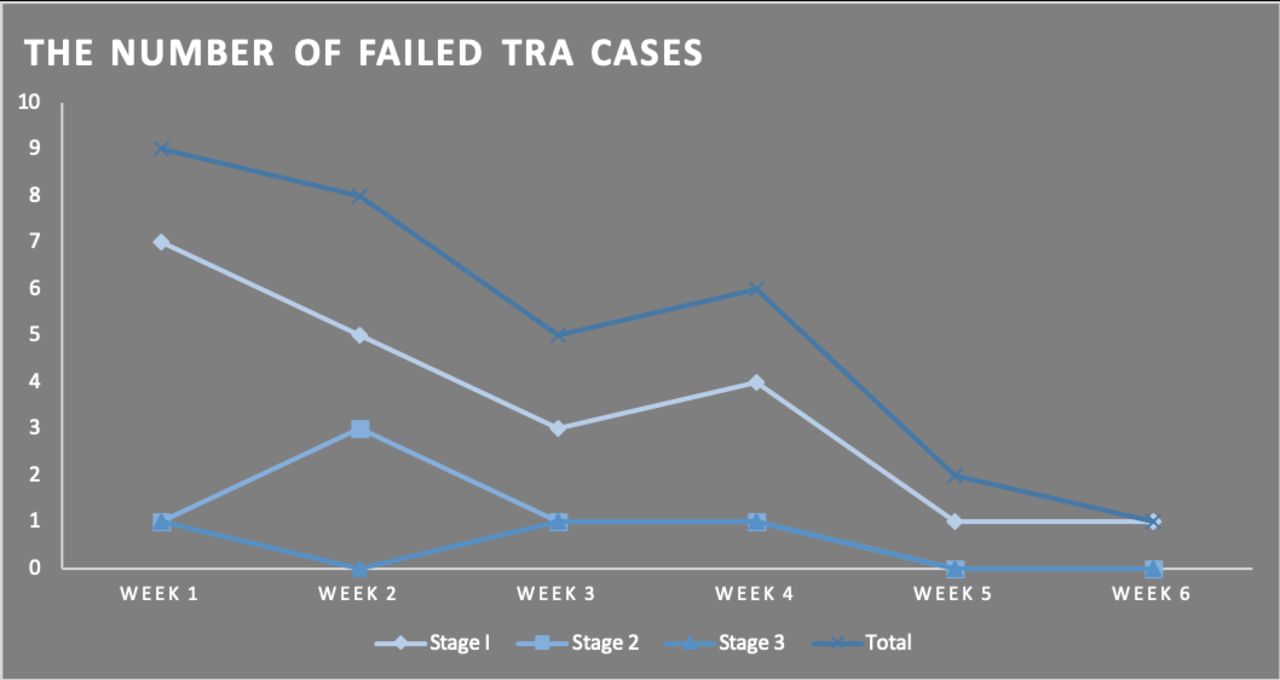
TFA access was obtained in patients who failed TRA puncture. TRA failure was categorized into three stages:
Stage I: failure to insert the sheath (secondary to small radial artery on ultrasound, no return of blood following the arterial puncture, inability to advance the wire due to vasospasm, or atherosclerotic plaque).
Stage II: The sheath is in the radial artery but the operator is unable to advance the guidewire and/or the catheter (because of radial artery tortuosity or radial artery vasospasm).
Stage III: The guidewire and the catheter reached the aortic arch but the operator is unable to reach the target artery.
For the diagnostic cases, we considered a radial artery diameter less than the outer diameter of the 4/5 French Slender sheath (2.14 mm) to be insufficient. For the interventional cases, we considered a radial artery diameter less than the outer diameter of the 5/6 French Slender sheath (2.44 mm) to be insufficient.
Covariates
All included patients had a neuroendovascular procedure done between March 22 and April 30, 2019. Collected data included age, sex, date, indication of the procedure, sheath size, catheter and wire type, number of catheters and wires used, duration of the procedure, radiation dose, vessels selected, the need to convert to TFA, and complications.
Statistical analysis
Descriptive statistics were used to report patient demographic and clinical characteristics in the included patients. The analysis was conducted using SPSS Software Version 25 (IBM Corporation, New York, USA).
Results
A total of 121 procedures were included. TRA was successful in 91 (75.2%) patients (72 patients underwent a diagnostic procedure and 19 had an interventional procedure). Figure 1 shows the trend of interventional/diagnostic cases ratio over time.

The trend of interventional/diagnostic cases ratio over time.
Mean (SD) age was 56.8 (14.7) years, 54.9% (50/91) underwent the procedure in the outpatient setting, and 60.4% (55/91) were women. Crossover to TFA was required in 30/121 cases that failed TRA (Stage I: 21 cases, Stage II: 6 cases, Stage III: 3 cases). A total of 20 cases failed TRA in the first 60 attempted procedures and 10 cases failed TRA in the last 61 attempted procedures (p=0.052). Figure 2 shows the trend in cases that failed TRA requiring crossover to TFA during the study period. Of note, one of the cases that failed TRA was a spinal angiogram; although segmental artery selection was successful, the rostral-most branches could not be reached and the operator converted to TFA to complete spinal angiography of the arteries in the lumbar region.

{kind=link}
{kind=link}
Trend of cases that failed a transradial approach (TRA) during the study period.
Diagnostic cases
A total of 79 diagnostic procedures were performed including 78 cerebral angiograms and one spinal angiogram.
After obtaining radial artery access, a 5 French Simmons Glide-1 (Terumo) catheter was used first-line in most cases (n=57). Other catheters used first-line included 5 French Simmons Glide-2 (Terumo) (n=12), 5 French Dav (Cook Medical) (n=2), and 5 French VTK (Cook Medical) (n=1). There was a need to convert to a different catheter in nine cases to help in reaching the target blood vessel.
A 0.038 inch pre-shaped glidewire (Terumo) was used in all cases. A long tapered 0.038 inch glidewire (Terumo) was used as a second-line guidewire in six cases to help in reaching the target blood vessel.
All six major cerebral blood vessels (bilateral vertebral artery, external carotid artery, and internal carotid artery (ICA)) were imaged in 22 of the 72 successful cases. Table 1 summarizes the procedural metrics of the successful cerebral angiograms obtained through TRA. The highest success rate was for the right vertebral artery (63/72) followed by the right ICA (62/72), then the left ICA (59/72) and finally the left vertebral artery (48/72). Imaging was obtained from the subclavian arteries or the contralateral vertebral artery (in the case of difficulty selecting a vertebral artery) or from the common carotid artery (CCA) (in the case of difficulty selecting an ICA).
Procedural metrics of the cerebral angiograms performed through the transradial artery approach
In some cases due to tortuosity, imaging of the right ICA was obtained by injecting the right CCA (n=10), imaging of the left ICA was obtained by injecting the left CCA (n=13), imaging of the right vertebral artery was obtained by injecting the right subclavian artery or the left subclavian artery (n=9), and imaging of the left vertebral artery was obtained (n=31).
No major immediate complications were noted. Minor complications included forearm hematoma that improved with local compression (n=2) and radial artery spasm that improved with intra-arterial verapamil (n=5).
Interventional cases
Table 2 summarizes the successful interventional procedures performed through TRA. Interventional procedures successfully performed included: aneurysm embolization (ruptured (n=3) and unruptured (n=8)), tumor embolization through the middle meningeal artery (n=2), cervical ICA stenting (n=2), balloon occlusion test (n=1), vertebral artery sacrifice (n=1), and arteriovenous malformation embolization (n=2). Of the two patients with an indwelling arterial line, both underwent successful conversion of the radial arterial line for access and successful salvage of the arterial line after procedure completion. Median (IQR) duration of the procedure was 72 (54–88) min, duration of fluoroscopy was 37 (19–50) min, radiation dose was 2800 (1600–4000) µGy, and contrast used was 130 (90–165) mL.
Interventional cases performed successfully through the transradial approach
Discussion
In this study we report our experience with full transition to TRA as the frontline approach for both diagnostic and interventional procedures over a short time course. To our knowledge, this is the first prospective case series involving both diagnostic and interventional cases being performed for the first time in an institution with minimal experience of TRA. Table 3 summarizes previously reported large case series in neuroendovascular procedures using TRA.
Summary of previous large case series describing the use of the transradial approach (TRA) in neuroendovascular procedures
The observed learning curve in our study (shown in figure 2) corresponds to reports from other institutions. Snelling et al analyzed data from 150 diagnostic cerebral angiograms using TRA and found that the operator efficiency improved with the number of procedures performed and the number of days since adoption of the TRA technique.12 Furthermore, Zussman et al found that the institutional learning curve in TRA can be overcome after performing 30–50 cases. This was reflected in our study by the rapid decline in the number of cases that failed TRA between the first half and second half of the attempted procedures. In addition, the time under fluoroscopy was significantly shorter for the second half of the diagnostic procedures once the operators were more familiar with the technique. However, the rate of crossover to TFA was 30/121 (24.8%), which is higher than that reported by Snelling et al (7/150; 4.7%), probably because the study was performed in a more experienced center and did not include interventional cases.
One of the remaining challenges of the TRA is that dedicated radial-specific catheters for neuroendovascular procedures are not yet widely commercially available. In our case series the Simmons Glide-1 catheter was the most used catheter given that it is highly flexible and can be formed into the arch without selecting a vessel (technique of pulling the wire back just proximal to the second curve to create a transition point, then advanceing the catheter while turning it). It is also highly trackable and can follow a 0.038 inch glidewire over significant tortuosity (for example, when advanced into the left ICA from the left CCA origin from the arch). The Simmons Glide-2 has a longer curve to it and has become our second-choice catheter. It is advantageous when more purchase is needed into the great vessels arising from the arch to select them, or when the angles of the vessels are more acute. For the interventional cases, the 6 French Benchmark has been our long-term guide catheter of choice for interventional cases (except thrombectomies) so the operators feel comfortable with it. In addition, it fits in a 6 French sheath as opposed to other guide catheters (eg, Neuron Max 088; Penumbra, California, USA) or AXS Infinity; Stryker, California, USA) which require an 8 French sheath.
Observational data suggest that TRA offers more advantages in neuroendovascular procedures in patients with complex iliofemoral anatomy, pregnant patients, patients with aortic dissection, and when the target vessel is in the vertebrobasilar system.13–16 This was reflected in our study by the high success rate of interventional cases with the target vessel in the posterior circulation. Moreover, previous studies have reported that women are at higher risk for access-related vascular complications in cardiac interventions and that the use of radial access reduces this risk.17–19 With TRA, however, the challenge remains that radial access may be more difficult in women due to smaller radial arteries and increased rates of radial artery spasm, potentially leading to lower procedural success rates. Interestingly, there was no difference in the rate of crossover to TFA in women compared with men in our cohort. Given the high success rates in this age group and the known high risk for ovarian radiation exposure with TFA, which is particularly important in women of childbearing age, we advocate TRA in this patient group.20 21
An important aspect of our study is that 46% of the included patients had their procedure done in the inpatient setting. TRA provides an advantage in this setting in patients who are on anticoagulation, given that it is less likely to cause access-related complications including bleeding and hematoma.1 2 22
The antispasmodic agent of choice in our study was verapamil, which has proven efficacy in the interventional cardiology literature.4 Other agents that have been used include intra-arterial nitroglycerin, which is more expensive and there is no strong evidence to support the notion that adding nitroglycerin to verapamil is more effective in preventing vasospasm.23
We also report two patients with indwelling arterial lines that were successfully utilized for access. This does not appear to be well documented in the literature and offers an easy route to minimize additional puncture attempts and facilitate faster access in the endovascular suite. In order to maintain the arterial line for continuous blood pressure monitoring, we augmented the TR Band protocol such that patent hemostasis was observed around the sheath. The arterial line remained functional after TR band deflation and avoided additional procedures in each patient.
Our study is limited by the single-center design and the small sample size. Larger-scale studies are needed to confirm the initial findings and discuss the cost-effectiveness of this approach.
Conclusion
This is the first prospective study to report the feasibility of using TRA for both diagnostic and interventional neuroendovascular procedures in a center with minimal experience in this approach. Our data show that upfront adoption of radial artery access for both diagnostic and therapeutic neuroendovascular procedures is feasible with a low complication rate and can be achieved in a matter of weeks.
References
Footnotes
Contributors All authors have provided a substantial contribution to the conception and design of the studies and/or the acquisition and/or the analysis of the data and/or the interpretation of the data. They have drafted the work or revised it for significant intellectual content and approved the final version of the manuscript. They agree to be accountable for all aspects of the work, including its accuracy and integrity.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The authors confirm that the study is an observational minimal risk study and no consent is required per the Medical University of South Carolina institute policy. Our study was approved by the institutional review board of the Medical University of South Carolina.
Competing interests AS: Penumbra consulting, Minnetronix consulting, Cerenovus consulting.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data from this project can be acquired by contacting the corresponding author.
Patient consent for publication Not required.