Article Text

Abstract
Background Robots in surgery aid in performing delicate, precise maneuvers that humans, with inherent physical abilities, may be limited to perform. The CorPath 200 system is FDA approved and is being implemented in the US for interventional cardiology procedures. CorPath GRX robotic-assisted platform is the next-generation successor of CorPath 200.
Objective To discuss the feasibility and early experience with the use of the CorPath GRX robotic-assisted platform for neuroendovascular procedures, including transradial diagnostic cerebral angiograms and transradial carotid artery stenting.
Methods The cases of 10 consecutive patients who underwent neuroendovascular robotic-assisted procedures between December 1, 2019 and December 30, 2019, are presented.
Results Seven patients underwent elective diagnostic cerebral angiography, and three patients underwent carotid artery angioplasty and stenting using the CorPath GRX robotic-assisted platform. All procedures were performed successfully, and no complications were encountered. Conversion to manual control occurred in three diagnostic cases because of a bovine arch that was previously not known. The fluoroscopy time and the procedure time continued to improve with subsequent procedures as we streamlined the workflow.
Conclusion This series demonstrates the early use of this technology. It could potentially be used in the near future for acute stroke interventions in remote geographic locations and in places where a neurointerventionalist is not available.
- aneurysm
- angiography
- device
- intervention
- stroke
Statistics from Altmetric.com
Introduction
Robots are electromechanical machines that can be used to perform repetitive, challenging tasks, or tasks that need extreme precision.1 The purpose of any robotic surgery system is to increase human performance beyond the limitations of inherent physical abilities and to perform surgeries from remote locations. Advancements in robotic technology over the past two decades have spurred the use of robotics in surgical procedures after its introduction in the 1980s. However, early models were primarily designed for the demands of other surgical specialties and, therefore, have not found a broader niche in neurosurgical procedures. It was not until a few years ago that robotic systems were specifically designed to assist in neurosurgical procedures, allowing their routine incorporation in spine surgeries.
CorPath GRX robotic-assisted platform (Corindus Inc, Waltham, USA) is the next-generation system after CorPath 200 (Corindus Inc., Waltham, USA) and was initially designed for interventional cardiology procedures. CorPath 200 was evaluated in prior clinical trials, and the robotic platform has been approved for use by the Food and Drug Administration (FDA) and CE mark for percutaneous coronary interventions (PCIs).1 This system is now in use in several centers in the United States for interventional cardiology procedures.1
We discuss the feasibility, early experience, and proof of principle of the CorPath GRX robotic-assisted platform (Corindus Inc, Waltham, USA) for some neuroendovascular procedures. The procedures in this series include transradial diagnostic cerebral angiograms and transradial carotid artery stenting.
Methods
Patient population
We report our experience with 10 patients who underwent neuroendovascular procedures (diagnostic and interventional) using the CorPath GRX robotic-assisted platform between December 1, 2019 and December 30, 2019. This was a retrospective chart review. Informed consent was obtained for all patients before the procedure. The FDA approval statement for CorPath GRX is “The CorPath GRX system is intended for use in the remote delivery and manipulation of guidewires and rapid exchange catheters, and remote manipulation of guide catheters during percutaneous coronary and vascular procedures.” Carotid artery stenting and cerebral diagnostic angiography fall under the label of peripheral vascular procedures, and thus both were on-label procedures. A clear discussion was held with the patients about the risks associated with the procedure in general. Also, the patients were informed that it is a new technology that had received FDA approval for peripheral vascular procedures, including carotid artery stenting. In addition, it was explained to them that diagnostic cerebral angiograms are obtained by parking the catheter in the extracranial supra-aortic vessels, and thus diagnostic cerebral angiography would be on-label use of the device. The patients were informed of the possibility and low threshold of conversion to a manual procedure if any problem occurred that could jeopardize safety. Detailed discussion was undertaken about the nuances of this technology, such as precise and fine navigation of the catheters, early experience, and lack of haptic feedback. The study protocol was reviewed and approved by the institutional review board. Consent was waived owing to the retrospective nature.
Setup and technique
The CorPath GRX robotic-assisted platform consists of a remote physician unit (figure 1A) and a bedside unit (figure 1B).2 The bedside unit comprises an articulated arm, a robotic drive, and a single-use disposable cassette (figure 2). The cassette is the mechanical transmission module that translates the real-time commands issued from the remote physician unit's designated joysticks to manipulate the devices. This can enable the operator to advance, retract, and rotate the catheters and wires. The robotic system is an open-architecture system that is compatible with 0.014 and 0.018 inch guidewires, rapid exchange catheter systems, and other devices. This system allows manipulation of the guidewire, balloon, and/or stent catheter with one hand and allows operation of the automatic contrast media injector with the other hand. We, however, did not use the automatic contrast media injector in this case series.

(A) Remote physician unit of the robotic system. (i) High definition screen to view fluoroscopy images; (ii) guide catheter/diagnostic catheter joystick; (iii) guidewire joystick; (iv) device joystick; (v) joystick feedback monitor. (B) Bedside unit of the robotic system. (i) Robotic arm; (ii) disposable cassette.
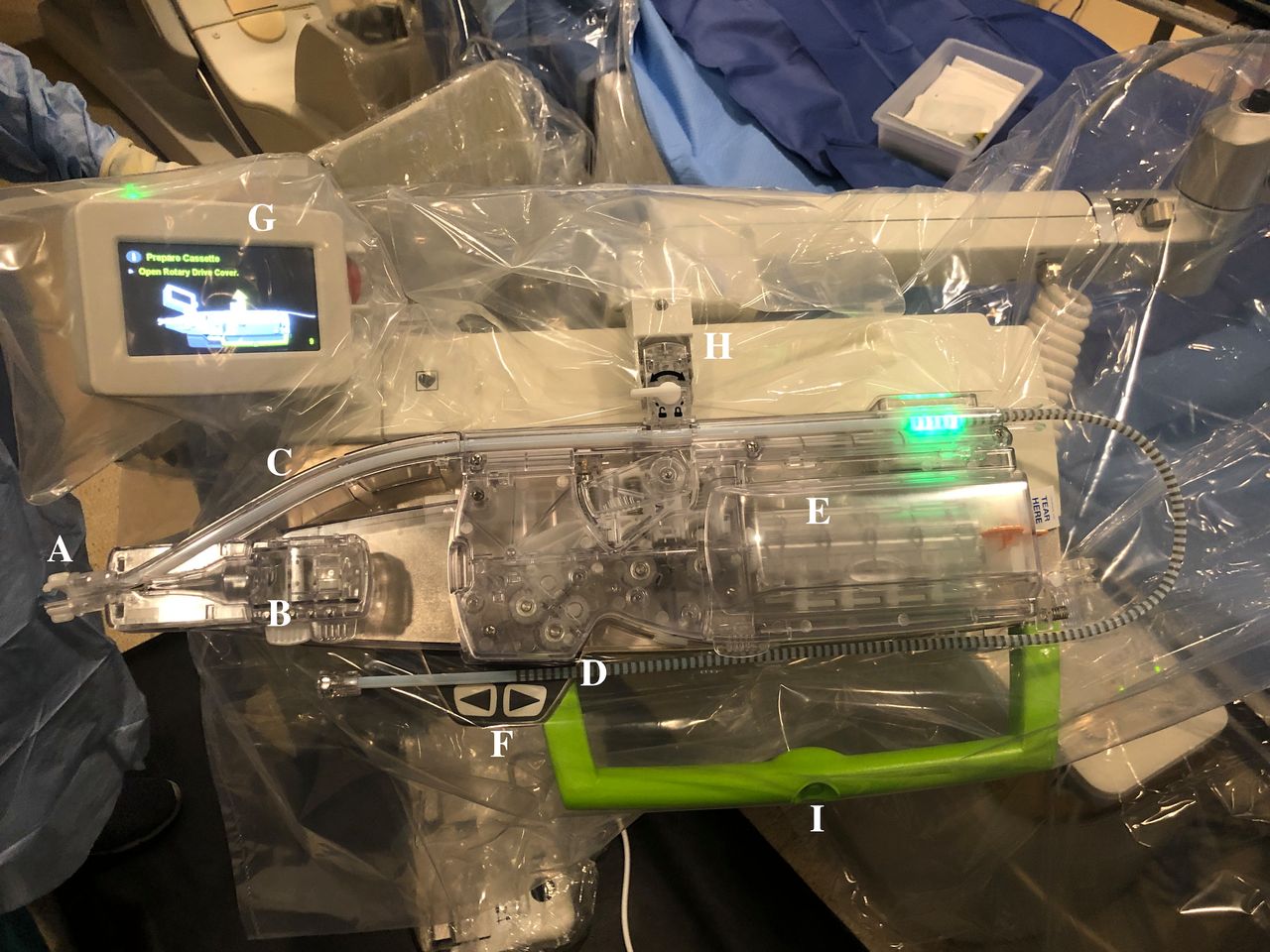
Parts of the disposable cassette. (A) Sheath attachment; (B) guide catheter rotation module; (C) guide support track; (D) device port., manual port is not well visualized in the closed cassette; (E) guidewire rotation module; (F) micro-adjustment buttons; (G) robotic arm feedback console; (H) cassette lock; (I) robotic arm toggle button.
Our setup of the remote physician unit stationed outside the room completely eliminates radiation exposure for the physician, while minimizing radiation exposure for the technicians.
The fluoroscopy and hemodynamic monitors are seen on the remote physician unit, enabling visualization in real time. Axial and rotation motions are performed by commands obtained from the remote physician unit using joysticks (figure 1A). The joysticks can translate precise and highly sensitive movements while the catheter is watched on the fluoroscopy monitor. When a power injector is connected to the injection port of the diagnostic catheter, and a wireless fluoroscopic pedal is placed outside the room, a diagnostic cervical and cerebral angiogram, including a 3D angiogram, can be obtained by selecting the proximal vessels.
The robotic arm of the CorPath GRX system was prepared under sterile conditions, and the disposable cassette was attached to the platform of the arm. The proximal end of the catheter to be used was attached to a hemostatic valve (Copilot, Santa Clara, California, USA). The cassette of the robotic arm had a guide slot (figure 2) that could secure the catheter with the copilot attached to it. The guide support track could then be pulled over the Simmons Select catheter (Penumbra, Alameda, California, USA) or the Benchmark catheter (Penumbra, Alameda, USA) and locked (figure 3) onto the side port of the radial sheath. The time required to install a device into the cassette is about 20 s. The cassette is then locked and ready for the robotic unit to manipulate the catheter (online supplementary video 1).
Supplementary video

{kind=link}
{kind=link}
{kind=link}
Cassette is shown open. (A) Prepared to be loaded with the diagnostic or the guide catheter. (i) Device port; (ii) manual port. (B) Diagnostic catheter and the guidewire loaded into the guidewire rotation module.
For the diagnostic cerebral angiograms (DCAs), we accessed the right radial artery at the distal transradial (anatomic snuffbox) site using a micropuncture needle and advanced a 0.021 inch radial access wire. The needle was then exchanged for a 5 F sheath and a radial cocktail, consisting of 2000 units of heparin, 5 mg nicardipine, and 200 μg nitroglycerin, was injected into the sheath. After this, a Sim Select catheter (Penumbra, Alameda, California, USA) was advanced over the wire into the descending aorta manually. At this point, the catheter was connected to the bedside unit of the robot, and the physician operating the remote unit took over the procedure. Using the robotic arm, the Sim catheter was reshaped in the descending aorta, and the carotid and vertebral arteries were accessed. Angiograms of the supra-aortic vessels were obtained. After this, the catheter was brought down into the descending aorta and then removed. A Vasc Band was used to remove the sheath (online supplementary video 2).
Supplementary video
For the carotid stenting procedures, we accessed the right radial artery using a micropuncture needle, which was exchanged for a 7 F radial sheath over a 0.021 inch wire. The patient was heparinized according to protocol. A coaxial system of a 6 F Benchmark guide catheter and 5 F diagnostic catheters (Penumbra Sim select or Berenstein select) over a 0.038 inch glidewire was used. A Benchmark catheter over a Sim Select catheter was advanced and positioned in the aortic arch manually and then connected to the bedside unit of the robot. The physician at the remote unit then took over the procedure. Under a biplane roadmap, a Synchro2 wire (Stryker Neurovascular, Fremont, California, USA) was advanced with robotic assistance while precisely avoiding plaque. A Spider FX filter device 6.0 mm (Medtronic, Irvine, California, USA) was advanced over the wire and deployed with robotic assistance in the infrapetrous carotid artery. Next, an Aviator plus balloon 6×40 mm (Cordis, Hialeah, USA) was advanced over the wire and the lesion was crossed with robotic assistance. Balloon angioplasty was performed manually. The balloon was then deflated manually and removed with robotic assistance. Next, a 7×40 mm Precise carotid stent (Cordis, Hialeah, USA) was advanced with robotic assistance, and the lesion was crossed. The stent was then deployed manually. The stent catheter was robotically removed, and a carotid injection was performed, which showed improvement of stenosis. The Benchmark catheter was then removed with robotic assistance, and the sheath was removed with the help of a Vasc Band (online supplementary video 3).
Supplementary video
Outcomes
Our primary goal was completion of the endovascular procedure using robotic assistance. We set a safety and efficacy goal to use a single catheter and a single attempt with robotic assistance. If catheterization of the vessel of interest failed with the first catheter, we did not use robotic assistance for the second attempt, but instead moved to a manual procedure.
Results
Seven patients underwent elective DCA, and three patients underwent carotid angioplasty and stenting using the CorPath GRX robotic-assisted platform. All procedures were successful, and no complications were encountered (table 1)
Procedural Details.
Conversion to a manual procedure occurred in cases that had a bovine arch that was not previously known. In our regular practice, for catheterization of the left common carotid artery from the right radial artery, we use either a Bernstein catheter (Cordis, Florida, USA) to access the left common carotid artery, or we advance the glidewire (Terumo Medical Incorporation, Somerset, New Jersey, USA) followed by the Sim Select catheter into the left common carotid artery. Patients 3, 5, and 7 had a bovine arch, and the procedure was converted to manual after completing the vertebral and right common carotid artery injections. This was in keeping up with our goal of using a single catheter and a single attempt. We were unsuccessful in using the Chikai black 0.018 wire (Asahi Intecc Co, Japan) and the Aristotle 0.018 wire (Scientia Vascular, West Valley City, Utah, USA) over a Phenom 21 microcatheter (Medtronic, Irvine, California, USA) to access the left internal carotid artery in patient 5. We did not attempt similar access in patients 3 and 7. This is a limitation of the system in not being able to use the 0.035 or 0.038 glidewires robotically, as described later. Therefore, we converted parts of these procedures to manual, accessed the left common carotid artery, and completed the DCAs. In the rest of the patients, we were able to perform all the planned technical steps, achieving good technical success with no complications.
The fluoroscopy time and the procedure time continued to improve with subsequent procedures as we streamlined the workflow.
Discussion
Advantages
Robotic-assisted neurointerventions have potential benefits for a patient’s safety owing to precise device control and deployments. Minor movements due to physiological tremor are eliminated for more controlled navigation. The benefits for the operating team include avoiding radiation and other occupational hazards. Elimination of ionizing radiation can reduce cancers, lens opacities, and atherosclerosis in the interventionalists. No data are available on the long-term health effects of cumulative radiation exposure.3 It was also previously shown in the RELID (Retrospective Evaluation study of Lens Injuries and Dose) study and other studies that interventionalists have cataract-type eye opacities three times more often than an age-matched controlled group.4 5 Other advantages include much more controlled and precise device manipulations and deployments. After reaching the target site, the system is extremely stable to make submillimeter movements.
The neurointerventional field is growing with increasing numbers and types of procedures. As the volume and types of procedure grow, we will start to see lengthy procedures to achieve better outcomes (eg, achieving a Thrombolysis in Cerebral Infarction (TICI) score of 2a/3 instead of stopping at TICI 2a) and higher procedural volumes. Radiation exposure is a particular concern and requires monitoring.6 These and other factors will lead to increments in fluoroscopy time and physical demands on neurointerventionalists. A critique of transradial procedures is that the interventionalist is positioned closer to the radiation source and might have higher radiation exposure. This could be eliminated by using a robotic system.
During a neurointerventional procedure, the interventionalists will be standing with heavy personal protective equipment, which exerts continuous force on the musculoskeletal system, leading to cervical and lumbar injuries.1 Obtaining diagnostic cerebral angiograms represents a large portion of the work performed in the neurointerventional field, and use of robotic systems can decrease radiation exposure and other occupational hazards, such as 'interventionalist's disc disease'.7 Spine problems were previously shown to be related to the annual procedure case load and number of years in practice.3 In their web-based survey, Goldstein et al noted a striking incidence of orthopedic problems, which can lead to work absenteeism. Robotic assistance is beneficial in this area, reducing the physical demands and fatigue. Additionally, the neurointerventionalist can control the procedure remotely and sit comfortably without wearing a lead apron, and thus robotic assistance can minimize back discomfort and orthopedic injuries.1
It was previously shown that the learning curve for the Corindus robot is short.8 After performing three cases, interventionalists could complete the robotically assisted procedure more quickly without compromising safety. The other advantage of these robotic systems in cases of tortuous vascular anatomy is better navigation without herniating into the arch, as the straight vector force translated to the guide catheter is homogeneous compared with manual operation. This results in a continuous momentum and a smooth positioning of the catheter without herniation into the arch. This nuance becomes clearer, especially when the left carotid artery is accessed from the right radial access site.
Some of the complications during the interventions occur during lengthy procedures and are due to physical and cognitive fatigue when performing repetitive unsuccessful, and unyielding actions. However, as it is a more comfortable to perform the procedures without the heavy lead apron, errors due to fatigue can be overcome.
Limitations
The CorPath robot and other such systems are not yet approved by the FDA or CE mark for intracranial procedures. It is a new technology, and many aspects have to be worked out before widespread adoption. Although we continue to improve the workflow with every case, the cassette of the robot is not designed for neurodiagnostics and neurointerventions. A physician still needs to obtain vascular access and guide the catheter into the arch. Other personnel have to be present in the room to operate the table. The cassette is not designed for robotic manipulation of neurointerventional workhorse wires such as the 0.038 or 0.035 glidewire. This precluded use of these wires initially.
The cassette design also limits the navigation into the left common carotid in bovine arches. We attempted to overcome this limitation by using a coaxial system of the Phenom 21 microcatheter over an Asahi Chikai black 0.018 wire or Aristotle support 0.018 wire to super select the vessels, as described earlier. This coaxial system was placed in the device port to move it independently of the diagnostic catheter. Despite this, we were unable to super select the vessels without the catheter herniating into the arch owing to the lack of support offered by the microcatheter and microwire.
We later on positioned the glidewire in the manual port to manually operate the glidewire to super select the supra-aortic vessels. This was done in patient 8 to successfully super select the supra-aortic vessels without dismantling the cassette. This allowed us to continue using the robot to choose the other supra-aortic vessels to complete the angiogram.
The inability of the cassette to manipulate over the wire equipment is a significant limitation that precludes use of almost all modern neurointerventional devices. The device deployments were performed manually while the robotic arm navigated the device to the site of the lesion. The robotic arm cannot perform device deployments. These steps have to be done manually through the manual port of the robotic arm.
For intracranial procedures, force feedback or haptic feedback is essential during the microcatheter, microwire, and device manipulation. Force feedback devices for clinical vascular interventions are either non-existent or still in infancy.9 10 The Corindus system and other such robotic systems do not have dependable haptic feedback. This might impede widespread adoption until such systems are available. The other potential limitation in the cases done from remote locations is the internet speed and the delay, in addition to a limitation of the ability to salvage if a complication occurs.
Although the robotic system is expensive (about $600 000) as with any newer technology, the potential long-term health of the physicians and the safety it provides for patients have to be taken into account. The disposable cassettes also have an additional cost (about $300). Until advanced cassettes are available for rapid use during strokes, it might be deleterious to rely on robotic systems to perform time-sensitive procedures such as mechanical thrombectomies.
Future directions
The safety and efficacy of using such a system may be maximized by streamlining the workflow and enhancing the setup. Having wireless fluoroscopy pedals, power injector controls, and the table operating controls near the remote physician unit allows radiation exposure for the team to be reduced. We can also advance the Simmons catheter into the arch over a 0.018 wire that is supported by the system and then connect a power injector both for 'puffing' the Simmons into the cervical vessels and for angiographic runs.
Further investigation and improvement of this technology are warranted before it can become commonplace. The ability to perform remote robotic-assisted PCI was initially described by Beyar et al and, subsequently, the PRECISE (Percutaneous Robotically Enhanced Coronary Intervention) pivotal trial demonstrated the safety and feasibility of robotic-assisted PCI in a large multicenter study of 164 patients.8 In 2016, Mahmud et al reported the results of a smaller feasibility study, Robotic-Assisted Peripheral Intervention for peripheral arterial Disease (RAPID), evaluating the CorPath platform for use in performing peripheral arterial revascularization.11
The CorPath GRX robot has been used in India to perform remote robot-assisted PCIs from 20 and >100 miles away.6 12 We hope that such application may be applied in the future for stroke treatment, in deprived remote areas.
The future of this technology includes its use for remotely performed procedures like stroke thrombectomies where a neurointerventionalist is not available, with the stipulation that a fast internet connection is needed. This might especially be possible after the roll out of faster internet speeds with low lag times, such as the 5G. To achieve this, we would need additional modules, such as video displays similar to that used for a telestroke. Other technologies, such as steerable microcatheters, can also help in advancing this technology and ensure widespread adoption.
The other occasion on which these systems could be used is to remotely monitor new devices, which have been expanding fast in this field.
Conclusions
The CorPath system was easy to set up and user friendly for diagnostic cerebral angiography and carotid artery stenting. The advantage of this system is elimination of physician radiation exposure in our setup, and reduction of orthopedic injuries associated with high volumes of procedures by providing the ergonomic advantage of not wearing a lead apron. The rapid improvements in technological engineering may enable stroke interventions to be performed remotely.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @PascalJabbourMD
Contributors KCS, AS, FAS, NC, PJ drafted the manuscript and revised the manuscript for important intellectual content. RFS, MBA, RA assisted with data acquisition and analysis. HZ, VR, KCS, PJ reviewed the important intellectual content presented in the manuscript. SIT, MRG, NH, RR, PJ performed the treatment procedures and critically revised the important intellectual content. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PJ is a consultant for Medtronic and MicroVention. SIT is a consultant for Stryker.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.