Article Text

Abstract
Background Authors have noticed an increase in lung apex abnormalities on CT angiography (CTA) of the head and neck performed for stroke workup during the coronavirus disease 2019 (COVID-19) pandemic.
Objective To evaluate the incidence of these CTA findings and their relation to COVID-19 infection.
Methods In this retrospective multicenter institutional review board-approved study, assessment was made of CTA findings of code patients who had a stroke between March 16 and April 5, 2020 at six hospitals across New York City. Demographic data, comorbidities, COVID-19 status, and neurological findings were collected. Assessment of COVID-19 related lung findings on CTA was made blinded to COVID-19 status. Incidence rates of COVID-19 related apical findings were assessed in all code patients who had a stroke and in patients with a stroke confirmed by imaging.
Results The cohort consisted of a total of 118 patients with mean±SD age of 64.9±15.7 years and 57.6% (68/118) were male. Among all code patients who had a stroke, 28% (33/118) had COVID-19 related lung findings. RT-PCR was positive for COVID-19 in 93.9% (31/33) of these patients with apical CTA findings.
Among patients who had a stroke confirmed by imaging, 37.5% (18/48) had COVID-19 related apical findings. RT-PCR was positive for COVID-19 in all (18/18) of these patients with apical findings.
Conclusion The incidence of COVID-19 related lung findings in stroke CTA scans was 28% in all code patients who had a stroke and 37.5% in patients with a stroke confirmed by imaging. Stroke teams should closely assess the lung apices during this COVID-19 pandemic as CTA findings may be the first indicator of COVID-19 infection.
- CT angiography
- infection
- stroke
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Coronavirus disease 2019 (COVID-19) is a clinical manifestation of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), which was first detected in Wuhan, China in December of 2019.1 COVID-19 has since spread worldwide and was declared a global pandemic on March 11, 2020.2 As of April 5, 2020, at least 122 000 confirmed cases of COVID-19 had been detected in the state of New York, with at least 7000 succumbing to COVID-19 related deaths.3 The symptoms initially reported with COVID-19 were related to pneumonia, such as cough, fever, and dyspnea. However, subsequent studies have since shown that the severity of symptoms can vary greatly, from essentially asymptomatic to life-threatening complications,4–6 with manifestations transcending the respiratory system to include gastrointestinal disease, headaches, and altered mental status.7 8
Neurologic symptoms are prevalent in COVID-19 patients, with one report9 suggesting they can be seen in approximately 36% of hospitalized COVID-19 patients. Most recently, Poyiadji et al 10 reported that acute hemorrhagic necrotizing encephalopathy can be a manifestation of COVID-19 infection. The tendency of respiratory infections to increase the short-term risk of acute ischemic stroke11–14 may offer some explanation for the variety of neurological symptoms seen in this patient population. Although the exact pathway remains unestablished, it is believed that the systemic inflammatory response to the infection, rather than the microbe itself, is responsible for the elevated stroke risk. Proposed pathways include prothrombotic state, alterations in endothelial function, plaque instability, and rupture.15–18 Additionally, recent studies specific to SARS-CoV-2 have shown that the virus can cause a cytokine storm, which may induce acute ischemic strokes.19 20 CT angiography (CTA) of the neck and head that is obtained in acute workup for stroke will typically include the lung apices. With the recent alarming increase in incidence of COVID-19 infection, the authors observed abnormal findings in the apices that appeared more frequently than prior to the pandemic. Recent studies showing diagnostic utility of chest CT for COVID-19,21–23 prompted the authors to investigate whether evaluation of the lung apical portions captured on CTA may have utility in affecting patient care during the COVID-19 pandemic. In this study, we aim to assess (1) what proportion of all code patients who had a stroke have lung findings on CTA, (2) what proportion of patients with confirmed stroke have lung findings on CTA, and (3) how these findings correspond to COVID-19 status diagnosed by reverse transcriptase polymerase chain reaction (RT-PCR) from nasal swabs.
Methods
Study population
This multicenter retrospective study included patient populations of six hospitals spread across three New York City boroughs. Expedited institutional review board approval was obtained with a waiver of informed consent. Between March 16 and April 5, 2020, ‘code stroke’ was activated on a total of 141 patients presenting with acute neurological symptoms. All ‘code stroke’ patients were included in this analysis if they underwent head and neck CTA in addition to non-contrast head CT during their acute stroke workup. Patients were excluded if they (1) did not obtain a head and neck CTA scan such as for medical contraindication (n=20) or (2) did not have sufficient clinical data in our electronic medical record system (n=3).
Scanning parameters
Standard emergent stroke protocol was performed on a 64-slice LightSpeed VCT scanner (General Electric (GE) Healthcare, Waukesha, Wisconsin, USA) with helical rotation time of 400 ms and tube current of 200–600 mA. Scanning was timed to acquire a 0.625 mm axial slice thickness with field of view from the level of the aortic arch to the vertex based on the initial scout radiograph. An 80 kV tube voltage was used for all patients with matrix of 512 and with a pitch of 0.5. Angiography was performed with non-ionic iodinated contrast medium (Isovue 370 mg I/mL, Optiray, Guerbet) at an injection rate of 4 mL/s. Axial and coronal maximum-intensity projection images were reconstructed from initial axial images at a slab thickness of 5.0 mm and 5.0 mm reconstruction increment for axial and coronal maximum-intensity projection images.
Data collection
Demographic characteristics, vascular risk factors, vital signs, laboratory values, and COVID-19 status were collected from our institutional electronic medical record system. Vascular risk factors included the diagnoses of hypertension, coronary artery disease, diabetes mellitus type 2, atrial fibrillation, congestive heart failure, dyslipidemia, current or former smoking status, evidence of prior stroke, and overweight/obese body mass index. COVID-19 infection was confirmed by in-house in vitro RT-PCR of nasopharyngeal swabs performed on the Roche cobas 6800/8800 systems (Roche Diagnostic, Basel, Switzerland). Patients were considered COVID-19 negative if the RT-PCR was negative. Nasal swab was repeated typically up to three times in patients with high suspicion for COVID-19 infection if they presented with typical COVID-19 symptoms or if imaging (chest X-ray or CT chest) was incongruent with initial RT-PCR results. The presence or absence of stroke was confirmed on CT and/or MRI by a board-certified fellowship trained neuroradiologist.
Characterization of apical lung findings on CTA
Lung apices included in each CTA field of view were evaluated for the presence or absence of ground-glass opacity (GGO) and consolidation by a board-certified and fellowship-trained cardiothoracic radiologist blinded to the COVID-19 status of the patient. Ground-glass opacity is defined as an area of increased attenuation in the lungs on CT, through which bronchial and vascular markings are preserved. Consolidation refers to more dense opacification of the lungs with obscuration of underlying vascular markings.24 Parenchymal findings were further characterized as either ‘typical’ (figure 1), ‘indeterminate’ (figure 2), or ‘atypical’ (figure 3) based on a recent expert consensus statement for radiology reporting of COVID-19 chest CT findings.25 From this consensus, ‘typical’ findings suggest high likelihood for COVID-19 infection, but because of the community prevalence, ‘indeterminate’ was also grouped as suggestive for COVID-19 in the setting of the pandemic. Thus, ‘typical/indeterminate’ findings were grouped and considered as radiologically positive for COVID-19 related findings. ‘Atypical’ was considered unlikely to be related to COVID-19 infection.

Typical CT appearance of COVID-19 infection. Typical CT for COVID-19 pneumonia: axial CTA image of the lung apex in a patient in their 40s who presented with sudden aphasia and limb paresthesia and retrospectively found to have cough and fever for 1 week, shows bilateral peripheral ground-glass opacities in the upper lobes (arrows), some with a rounded morphology in the left lung. This patient tested positive for COVID-19 on RT-PCR.

Indeterminate CT appearance of COVID-19 infection. Indeterminate CT for COVID-19 pneumonia: axial CTA image of the lung apex in a patient in their 50s who presented with 2 weeks of headaches, myalgias, and worsening dysarthria, shows central, perihilar ground-glass opacities in the left upper lobe (arrows). The unilateral central and unilateral distribution makes this appearance ‘indeterminate’. This patient tested positive for COVID-19 on RT-PCR.

{kind=link}
{kind=link}
{kind=link}
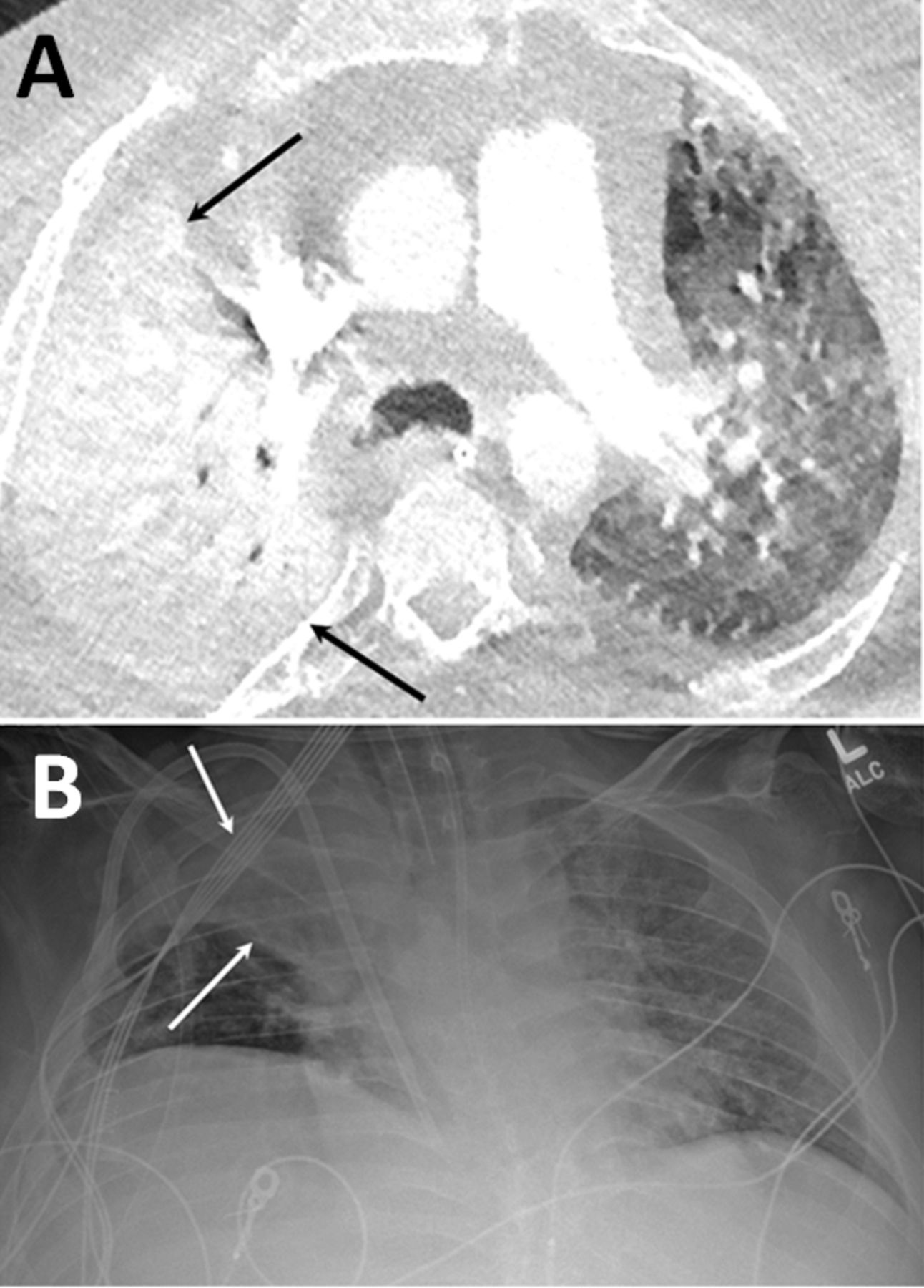
Atypical CT appearance of COVID-19 infection. Atypical CT for COVID-19 pneumonia: axial CTA image of the lung apex (A) in a patient in their 30s who presented with sudden altered mental status and syncope, shows completely right upper lobe consolidation (arrows). Corresponding anteroposterior chest X-ray examination (B) shows that the right upper lobe consolidation represents lobar collapse (arrows) secondary to mucus plugging. This patient tested negative for COVID-19 on RT-PCR.
Results
Clinical characteristics of patient population
Our patient cohort consisted of a total of 118 patients with mean±SD of age of 64.9±15.7 years with 57.6% (68/118) male (table 1). Of all code patients who had a stroke 40.7% (48/118) had acute infarction on imaging. Of the 118 patients, 31 (26.3%) were identified as COVID positive from nasal swab RT-PCR. The majority of patients worked up for acute stroke presented with altered mental status (35%) and dysarthria (38.1%).
Demographic characteristics study population
COVID-19 related lung findings on head and neck CTA
Of all code patients who had a stroke, 28% (33/118) of patients had COVID-19 related apical lung findings (table 1). All (33/33) patients with COVID-19 related lung findings had a component of GGO. Consolidations were seen in 18.2% (6/33) of patients with COVID-19 related apical findings. Subsequent RT-PCR revealed that 26.3% (31/118) of all code patients who had a stroke tested positive for COVID-19 status, and 93.9% (31/33) of patients with COVID-19 related apical findings tested positive for COVID-19 on RT-PCR.
Among patients with confirmed stroke, 37.5% (18/48) of patients had COVID-19 related apical findings with all (18/18) apical findings having a component of GGO and only 16.7% (3/18) with consolidations. RT-PCR was positive for COVID-19 in all (18/18) these patients with COVID-related apical findings.
Discussion
As the primary role of head and neck CTA during a ‘code stroke’ is to assess vascular pathology, such as a large vessel occlusion, aneurysm, or arteriovenous malformation, the lung apices may garner less attention and be regarded as having less clinical relevance. However, the authors have noticed an alarming increase in incidental findings in the apices of the lungs on CTA probably associated with an increase in COVID-19 cases during the pandemic. In this study, we demonstrated that 28% of all code patients who had a stroke and 37.5% of patients with confirmed stroke had lung apical findings on CTA related to COVID-19 and corresponding with RT-PCR findings. Thasan et al 26 had previously reported incidental findings in the lung apices on CTA in 20.8% of patients with confirmed strokes. In this study, we assessed only for COVID-19 related findings. The alarming rate of these lung findings draws attention to the importance of careful evaluation of the lung apices in patients who had a stroke. These findings may be the first and only indicator of a patient’s COVID-19 status during early emergency or inpatient evaluation, since standard RT-PCR from a nasal swab may take 6–12 hours or more for results. Furthermore, a patient presenting to the hospital with a suspected stroke is likely to undergo emergent CTA well before RT-PCR results are known or even performed. In addition, with low sensitivity and reliability of RT-PCR,27 management could be altered significantly if imaging findings suggest a positive incongruent COVID profile.
The importance of these observations to the endovascular surgeon and stroke neurologist are multifold. As these patients presented with predominantly neurologic symptoms, this study attests to the wide range of symptomatology associated with COVID-19 infection and raises awareness that if lung findings are observed, these patients should be placed in isolation or in a designated COVID investigation area and tested for COVID-19. If these findings are observed in the lung apices, the stroke team should wear appropriate personal protective equipment when revisiting the patient. Stroke neurologists and endovascular surgeons should be aware of the significance of apical findings on CTA and consider extra precautions when evaluating these patients.
Additionally, members of the stroke team may benefit from understanding the characteristic features of COVID-19 related lung findings and differentiate them from 'atypical' findings as lung findings for COVID-19 may be diverse.25 In this study, we characterized the appearance of COVID-19 related findings and demonstrated that these predominantly include GGOs. Although chest CT has been shown to be superior to chest X-ray examination21 23 28 and has a sensitivity of up to 93%,21 the utility of apical evaluation on neck CTA has not been previously evaluated. Recent studies have shown that the presence of GGOs in the periphery of lung parenchyma correlates with duration of the COVID-19 infection with a change in characteristic pattern with time.29
There are several limitations to our study. First, lung apices were evaluated by only one cardiothoracic rater. Having multiple reviewers score apical lung findings would improve the reliability of our assessment and reduce operator bias. Additionally, we used the 'gold standard' of RT-PCR from a nasal swab, for which the sensitivity and specificity for diagnosis of COVID-19 has not been definitively established. Despite the test’s approval under emergency use authorization, recent studies have shown that it may have sensitivity as low as 70% for the diagnosis of COVID-19.21 27 30 Furthermore, we acknowledge that chest imaging findings in COVID-19 patients are not specific and may overlap with other viral (particularly, influenza), bacterial, and autoimmune/inflammatory processes (eg, alveolar hemorrhage in patients with systemic lupus erythematosus) as imaging manifestations are probably from a systemic inflammatory response to the infection rather than the microbes themselves. However, given the ongoing COVID-19 pandemic and waning of the influenza season, these non-specific findings are more likely to be related to COVID-19 infection, due to a higher pretest probability at this time. Finally, this study was conducted in New York City, which is an epicenter of the pandemic. Thus, the incidence rate reported in our study may not necessarily be applicable to all institutions. However, given the spread of COVID-19 and ongoing pandemic, we believe that this study serves to raise awareness to the stroke team, which is applicable at all locations experiencing the pandemic.
In conclusion, to our knowledge this is the first study to evaluate the incidence of COVID-19 related apical lung findings on head and neck CTA scans during acute stroke workup. The alarming incidence of these findings should raise awareness for the stroke neurologists and endovascular surgeons to check the lung apices on CTA and consider extra precautions when evaluating patients with characteristics findings for COVID-19. This may become especially relevant when imaging is the first tool to suggest COVID-19 infection, and early recognition can facilitate more prompt isolation and treatment strategies. The alarming rate of lung apical findings in code patients who had a stroke may even prompt consideration for extension of the CTA protocol beyond the apices to confidently rule out patients in concert with a negative nasopharyngeal swab or for detection of COVID-19 in patients with chest imaging manifestations outside the lung apices. Ongoing efforts to improve early COVID-19 diagnosis and patient care may benefit from extending head/neck CTA protocol during code strokes to capture the entire chest during the COVID-19 pandemic.
References
Footnotes
Contributors Study design: SK, JS, MC, JM, PB. Data collection: SK, JS, MC, KM, BR. Statistical analysis: SK, PB. Manuscript writing: SK, JS, MC, KM, BR, BND, JM, AD, PB.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Institutional review board (IRB) of the Mount Sinai School of Medicine, in accordance with Mount Sinai’s Federal Wide Assurances (FWA#00005656, FWA#00005651) to the Department of Health and Human Services, approval was obtained on an expedited basis with a waiver of informed consent. IRB approval number: #20-03376.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data for this manuscript are included in the manuscript. There is no supplementary information.