Article Text

Abstract
Background Intra-arterial treatment is gaining importance in acute ischemic stroke, but its role in patients with apparent occlusion of the extracranial internal carotid artery (ICA) on computed tomographic angiography (CTA) is inconclusive.
Objective To review retrospectively the results of intra-arterial treatment in patients with stroke and apparent extracranial ICA occlusion.
Methods In more than 3000 patients with stroke admitted to our institution during 2008–2013, and the subgroup with suboptimal results after intravenous thrombolysis (IVT), CTA showed the absence of contrast in the extracranial ICA in 16 patients. Angiography showed true occlusion of the extracranial ICA in 10 and pseudo-occlusion in 6 patients. Treatment was considered technically successful when Thrombolysis in Cerebral Infarction scale (TICI) scores improved to 2 or 3 and clinically successful when the National Institutes of Health Stroke Scale (NIHSS) improved by at least 10 points or a NIHSS score of 0 or 1 was found at discharge.
Results Recanalization was achieved in 5 of 6 patients with pseudo-occlusions and in 6 of 10 patients with true occlusion of the extracranial ICA. Favorable clinical outcomes were seen in 3 of 6 patients with pseudo-occlusions and in 4 of 10 patients with true occlusions. Four patients died, and in these patients infarction of >15% of the affected hemisphere had been seen on admission CT.
Conclusions In cases of acute stroke and apparent occlusion of the extracranial ICA, intra-arterial treatment should be considered, especially when IVT fails and <15% of the hemisphere is infarcted on CT. Endovascular treatment may be beneficial especially in pseudo-occlusions but also in true occlusions of the extracranial ICA.
- Stroke
- CT Angiography
- Stent
- Thrombolysis
- Thrombectomy
Statistics from Altmetric.com
Introduction
Occlusion of the internal carotid artery (ICA) in stroke is usually diagnosed on computed tomographic angiography (CTA) by the absence of intraluminal contrast material. However, this appearance is known to have multiple causes. It may be caused by a true occlusion of the vessel because of thrombosis or dissection, but also by a pseudo-occlusion with severely reduced blood flow or stasis due to a high-grade stenosis of the extracranial ICA or an occlusion of the intracranial ICA or proximal middle cerebral artery (MCA). In these cases of slow flow and altered fluid dynamics, the rapid CTA acquisition can ‘outrun’ the contrast material resulting in an inadequate arterial opacification suggesting an occlusion.1–3
According to the neurological literature, the prognosis for patients with acute stroke and carotid occlusion is poor with permanent disability in 40–69%, death in 16–55%, and good recovery in only 2–12%.4 Occlusion of the extracranial ICA on CTA is often associated with coexistent intracranial acute occlusions. Complete ICA occlusion at all levels is associated with poor clinical outcome, while partial distal preservation of the vessel is more likely to benefit from intra-arterial therapy.5 Until now, such patients with apparent ICA occlusions have usually been treated with intravenous thrombolysis (IVT), with a low recanalization rate of around 30%.6 Although intra-arterial treatment is gaining importance in the treatment of acute ischemic stroke,7 its role in patients with apparent occlusion of the extracranial ICA on CTA is inconclusive. However, treatment of extracranial ICA occlusions is mandatory to facilitate intra-arterial thrombolysis (IAT) or mechanical thrombectomy (MT) of intracranial vessels and to prevent re-occlusion or new distal embolism.8 Several studies have shown that stenting of the extracranial ICA in acute stroke is feasible to restore blood flow for short occlusions.9–13 In patients with complete thrombosis of the entire length of the ICA and especially those with a dissection, restoration of blood flow is more demanding.
Once the blood flow in the ICA is restored, the patient's thrombolytic system may be more effective and the often coexisting embolus in the MCA can be reached and treated more easily.14 Revascularization of a distal occlusion in the intracranial ICA, MCA or anterior cerebral artery is critical to maximize the chance of a good functional outcome.13–15
Our study aimed at assessing the technical and clinical results of endovascular treatment in patients with a stroke with apparent occlusion of the extracranial ICA on CTA.
Patients and methods
Between June 2008 and June 2013 more than 3000 patients presented with an acute stroke at the first aid department of our hospital. In all these patients unenhanced CT of the brain was performed to rule out other pathologies such as hemorrhage, tumor, and chronic subdural hematoma. All patients were scanned on either a 16-slice Toshiba Aquillion, Tokyo, Japan or a 2×128 slice Siemens Somatom Definition Flash, Erlangen, Germany.
When an ischemic cause of stroke was proved, patients were considered for IVT with recombinant tissue plasminogen activator (0.9 mg/kg body weight). Patients with uncontrolled hypertension, recent hemorrhage, surgery, or large areas of cerebral infarction were not eligible. Patients who received IVT were observed during the following hour and if no clinical improvement was seen they were considered for IAT or MT.
Patients who were candidates for intra-arterial treatment underwent subsequent triggered CTA to define the site and extent of occlusion of a carotid, cerebral, vertebral, or basilar artery (120 kV, 390 mA, pitch 0.75, slice thickness 0.75 mm, 100 cc iodine contrast (Xenetix 300) with saline flush, flow rate 3.5 cc/s, scan range from 3 cm below the aortic arch to the vertex).
During the 5 years mentioned above, 42 patients underwent intra-arterial treatment. For 16 of these 42 patients (seven men, nine women; mean age 61.8 (range 38–84) years) the extracranial ICA appeared to be occluded on CTA (figure 1). In 15 of these 16 patients this was in combination with an occlusion of the ipsilateral MCA. All 16 patients had major neurological deficits such as aphasia, hemiplegia, or hemiparesis defined as a National Institutes of Health Stroke Scale (NIHSS) of ≥3. None of the 16 patients responded successfully to IVT as described above and they were subsequently referred for intra-arterial treatment.

Selection of included patients. CTA, computed tomographic angiography; ICA, internal carotid artery; IVT, intravenous thrombolysis; MCA, middle cerebral artery.
Informed consent for intra-arterial treatment was obtained from the patient or their family in all cases.
The procedure
The common femoral artery was punctured under ultrasound guidance and an eight French sheath was inserted. After systemic heparinization (5000 IU), the common carotid artery or extracranial ICA was selectively catheterized, an eight French guiding sheath was placed, and angiography was performed.
Angiography showed occlusion of the entire length of the extracranial ICA in 10 patients, but in the other six the extracranial ICA was patent but the flow was sluggish.
In the 10 patients with a true occlusion, the ICA was catheterized with a 0.014 inch guidewire (Balanced Middle Weight, Abbott, Santa Clara, California, USA). If recanalization was achieved, a self-expandable carotid stent was placed from the distal common carotid artery to the proximal ICA, covering the origin of the external carotid artery. Carotid Wallstent (BSC, Natick, Massachusetts, USA) and Precise Pro RX stents (Cordis, Bridgewater, New Jersey, USA) were used.
Patients with an additional intracranial occlusion underwent subsequent IAT and/or MT. The occluded intracranial ICA and MCA were catheterized with the combination of a Synchro 0.014 inch hydrophilic guidewire (BSC, Natick, Massachusetts, USA) and a microcatheter (Rebar 18, ev3, Irvine, California, USA, or Trevo Pro 18, Concentric, Mountain View, California, USA). A thrombolytic agent was then injected into the thrombus. The initial injection included 1–10 mg of dissolved recombinant tissue plasminogen activator (1 mg/mL), with a total amount ranging from 10 to 50 mg. Patients received either 1 mg Nimotop (nimodipine) or nitroglycerin intra-arterially to prevent and treat vasospasm. MT of the intracranial ICA or MCA occlusion was performed with a Merci Retriever System, a Trevo (Concentric) or a Solitaire FR revascularization device (ev3).
In the six patients with an angiographically non-occluded extracranial ICA, any high-grade stenosis of the extracranial ICA was also treated with a stent. Treatment of occlusions of the intracranial ICA and MCA was performed as described above.
After endovascular treatment, the patients were closely monitored in the stroke unit for 24 h. CT scans were obtained the day after treatment and if clinical deterioration was seen to rule out hemorrhage and to document the extent of the infarction. Patients received oral antiplatelet agents (aspirin 100 mg/daily and clopidogrel (Plavix) 75 mg/daily or dipyridamole (Persantin) 200 mg/daily or phenprocoumon on indication). This treatment was given only after 24 h.
Outcome measures
All patients were examined by a neurologist. Neurological status was defined at admission and at discharge from the hospital according to NIHSS criteria. Favorable clinical outcome was defined as an NIHSS improvement of at least 10 points or a NIHSS score of 0 or 1 at discharge.
A board-certified neuroradiologist studied the initial CT scans to rule out hemorrhage, to detect early signs of infarction, and to assess the extent of infarcted brain tissue. CTAs were examined to determine the site and extent of arterial occlusion. On follow-up CT scans the presence and amount of infarcted tissue and intracranial hemorrhage was documented.
Successful recanalization was defined as achievement of a Thrombolysis in Cerebral Infarction (TICI) scale16 of 2 or 3 in all treatable vessels. The final angiographic images were scored by one of the interventional radiologists.
Furthermore, we assessed any symptomatic intracranial hemorrhage and the time between the onset of stroke symptoms and the moment of intra-arterial access, which was related to the clinical outcome.
Results
Table 1 shows the CTA and angiographic findings for the 16 patients, and the type of intra-arterial treatment performed.
Computed tomographic angiography (CTA) and angiography findings and treatment performed in the 16 patients, subdivided by true and pseudo-occlusions of the extracranial internal carotid artery (ICA)
We subdivided the patients according to their angiographic findings into those with either true or pseudo-occlusions of the extracranial ICA. Ten patients had a true occlusion of the extracranial ICA on angiography caused by either complete thrombosis in atherosclerotic vessels (five patients) or dissection (five patients).
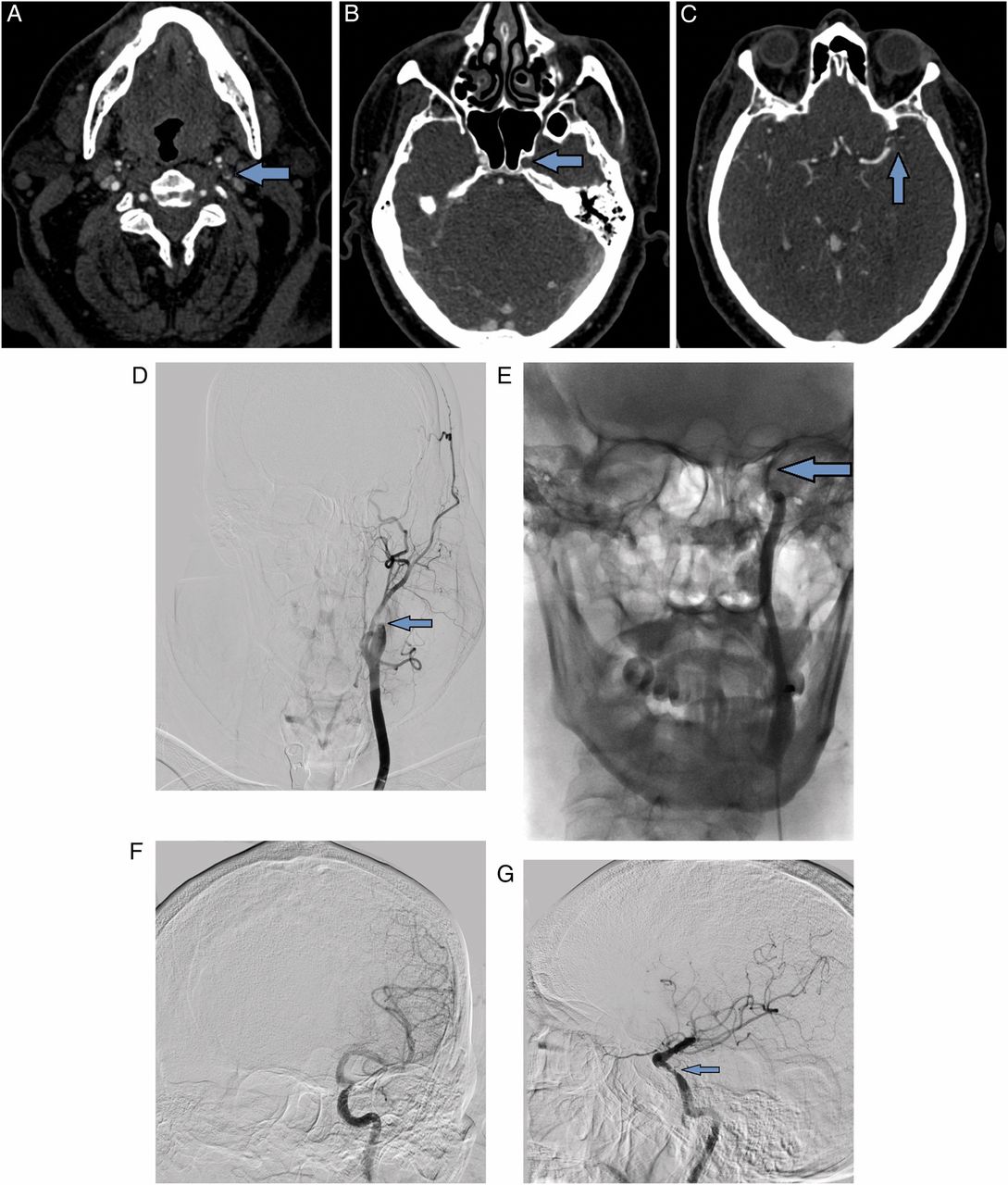
Angiography showed a pseudo-occlusion of the extracranial ICA in six patients. In four patients this was caused by stasis or reduced flow of blood proximal to an intracranial ICA occlusion. In two of four patients the intracranial ICA was occluded at the level of the carotid T (intracranial ICA bifurcation), and in the other two patients the intracranial ICA was occluded at the cavernous segment. In one of these four patients, patency of the extracranial ICA was best demonstrated after selective catheterization of the ICA. Figure 2A–G illustrates the discrepancy between CTA and angiographic images of patient 14.

{kind=link}
{kind=link}
Computed tomographic angiography (CTA): (A) Absence of contrast in left extracranial internal carotid artery (ICA). (B) Absence of contrast in intracranial ICA at the level of the carotid siphon. (C) Absence of contrast in distal M1 segment. Angiography: (D) Guiding catheter in left common carotid artery with occlusion of proximal extracranial ICA (arrow) in accordance with findings on CTA. (E) Selective catheterization of left intracranial ICA showing occlusion at the cavernous segment (arrow), but no thrombus in the extracranial ICA (unsubtracted image). (F) After thrombectomy (coronal view): patent middle cerebral artery (MCA) and persistent stenosis of the intracranial ICA. (G) After thrombectomy (sagittal view): patent MCA and persistent stenosis of intracranial ICA (arrow).
In two patients with a pseudo-occlusion of the ICA on CTA, no occlusion of the entire (extracranial and intracranial) ICA was found at angiography. In one of two patients a severe stenosis of the ICA at the extracranial carotid bifurcation impeded the flow. In the other patient angiography showed an occlusion of the MCA which had not been present on the previously performed CTA. In this case the thrombus that caused apparent occlusion of the extracranial ICA might have been resolved after previously administered IVT and subsequently embolized to the MCA.
Angiographic and clinical outcomes are displayed in table 2, showing the TICI, NIHSS scores and favorable clinical outcome before treatment and at discharge for all 16 patients.
Angiographic and clinical outcomes of the 16 patients
In the patients with true occlusions, successful recanalization (TICI 2 or 3) was achieved in six of 10 patients (recanalization rate 60%). In four patients, including two patients with a dissection of the ICA, no recanalization and no distal flow was achieved. Favorable clinical outcome was seen in four of 10 patients (mean NIHSS score of 14 at admission (range 3–22) and 3 at discharge (range 1–6)). Three of the 10 patients with true occlusions of the extracranial ICA died in the days after the stroke owing to a mass effect, two of these patients in spite of successful endovascular recanalization. An unenhanced CT scan at the time of admission had shown cerebral infarction with the amount of parenchyma affected varying from 15% to 50% of the hemisphere in these three patients. No early signs of infarction had been seen in the other seven patients in this group.
In the patients with pseudo-occlusions, a TICI score of 2 or 3 was achieved in five of six patients (recanalization rate 83%). In three patients NIHSS scores improved by ≥10 points. The mean NIHSS score in these patients was 15 at admission (range 11–17) and 2 at discharge (range 0–6). The NIHSS score in one patient improved from 6 to 2. In the patient in whom recanalization was not achieved (patient 12) prolonged IAT was unsuccessfully given at the occluded carotid T. Little clinical improvement was seen immediately after the procedure. The initial CT scan of this patient had shown 30% infarction of the affected hemisphere. The patient died a few weeks later in a nursing home owing to pneumonia. In the other five patients in this group no signs of infarction had been seen on initial CT scans.
All 16 patients were treated within 4 h after the onset of symptoms. There was no significant difference in the angiographic or clinical outcomes of patients treated after 2–4 h. In addition, no significant intracranial hemorrhage was seen in any of the 16 patients.
Discussion
Endovascular treatment should be considered in patients with acute ischemic stroke and an apparent occlusion of the extracranial ICA on CTA. First, this is because CTA can incorrectly suggest an extracranial ICA occlusion. This phenomenon of pseudo-occlusions, which was seen in six of 16 patients in our study, was first described by Kim et al.1 A second reason for considering endovascular treatment in such patients is because recanalization may be achieved both in patients with pseudo-occlusions and in those with a true ICA occlusion.
In our study, recanalization rates were higher in patients with pseudo-occlusions, but recanalization was achieved in more than half of patients (6/10) with a true occlusion of the extracranial ICA.
Two recent studies describe endovascular treatment of patients with stroke and combined extracranial ICA and MCA occlusions and report recanalization rates (TICI 2 or 3) of 62.5–100%.9 ,11
Kappelhof et al2 reported recanalization rates of 55% in patients with stroke and an intracranial occlusion and 71% in patients with an extracranial occlusion of the ICA. These rates are more or less consistent with the recanalization rates of 60% and 83% in patients with true and pseudo-occlusions of the extracranial ICA found in our study. In our experience, recanalization of dissections is especially difficult and challenging. Compared with IAT, significantly higher recanalization rates for MT in intracranial occlusions and stenting in extracranial ICA occlusions, respectively, were reported by Kappelhof et al. This finding is supported by our study, in which all of the successfully recanalized patients received either MT alone or a combination of MT, stenting, and/or IAT.
A favorable clinical outcome was seen in almost half of the patients in our study, which is somewhat higher than reported by Stampfl et al (25% vs 44% in our study).9 This might be owing to a high proportion of patients with intracranial hemorrhage in their series, probably caused by relatively aggressive antiplatelet therapy. In our institution, to prevent such bleeding complications, antiplatelet agents are given only after 24 h, when intracranial hemorrhage has been ruled out on follow-up CT. Kappelhof et al2 report favorable clinical outcomes in 25% of patients with intracranial occlusions and in 68% of patients with extracranial occlusions of the ICA. This is reasonably consistent with the results of our study, although definitions of favorable outcomes differ between the two studies. In our study, higher favorable outcomes were seen in patients with pseudo-occlusions, but also in almost half of the patients (4/10) with true occlusions of the extracranial ICA.
It is known that the extent of infarcted hemisphere is a prognostic factor of clinical outcome17 and the four patients in our study, in whom more than 15% of the hemisphere showed infarction on the initial unenhanced CT, died in the following days or weeks after treatment, despite successful recanalization in two of them. This amount roughly correlates with the 33% of MCA territory as used in the European Cooperative Acute Stroke Study.7 As our experience of intra-arterial treatment of patients with stroke has increased, it has resulted in a more conservative policy whether to treat intra-arterially or not. Our mortality rate of 25% is comparable to those of other studies, with rates ranging from 11% to 33%.2 ,9 ,11 ,15
Conclusion
Our study suggests that in patients with acute stroke and apparent occlusion of the extracranial ICA, intra-arterial treatment should be considered, especially when IVT has failed and <15% of the hemisphere is infarcted on CT. Intra-arterial treatment seems particularly beneficial for patients with a pseudo-occlusion of the extracranial ICA on CTA. In patients with a true extracranial ICA occlusion the results are less good, but, nevertheless, recanalization can be achieved in more than half of patients with a favorable outcome in almost half of them.
References
Footnotes
Contributors HMD, HvO: study design, analysis of results, primary manuscript writing. HMD, HvO, FS, LCvD, FET, RWK, AM, CBM: data collection, critical evaluation of manuscript. HMD: tables and figures.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.