Article Text

Abstract
Background Debate exists as to whether patients with acute ischemic stroke who are undergoing mechanical thrombectomy should receive general anaesthesia or conscious sedation during the procedure. Using a multihospital administrative database, we compared outcomes and complications of patients receiving mechanical thrombectomy, who were receiving general anaesthesia and conscious sedation, and studied trends in usage over time.
Materials and methods Premier database patients who underwent mechanical thrombectomy from 2006 to 2013 for acute ischemic stroke were identified. Using propensity score analysis, recipients of general anaesthesia and conscious sedation underwent 1:1 matching. Outcomes including usage trends, discharge status, mortality, length of stay, haemorrhage and pneumonia were examined.
Results A total of 2512 patients receiving mechanical thrombectomy were identified. 1999 (80%) received general anaesthesia and 513 (20%) received conscious sedation. Following 1:1 matching by the propensity score matching, 507 general anaesthesia and 507 conscious sedation patients were matched. Patients who received general anaesthesia during their procedure had significantly higher rates of in-hospital mortality (25% vs 12%, OR=2.37 95% CI 1.68 to 3.37, p<0.0001), and pneumonia (17.0% vs 9.3%, OR=2.0, 95% CI 1.35 to 2.96, p=0.0005) compared with patients of thrombectomy who received conscious sedation. ICH/SAH rates were similar between patients receiving general anaesthesia and patients receiving conscious sedation (11% vs 12%, p=0.62). Usage rate of general anaesthesia decreased from 83.8% in 2006 and 74.0% in 2013.
Conclusions In our cohort, thrombectomy patients receiving conscious sedation have decreased in-hospital mortality, decreased rates of pneumonia, and lower hospital costs and lengths of stay when compared with patients who received general anaesthesia. However, most practitioners continue to use general anaesthesia in the setting of acute stroke interventions.
- Stroke
- Complication
Statistics from Altmetric.com
Introduction
Intra-arterial reperfusion therapies are increasingly being used in the treatment of acute ischemic stroke.1 Timely reperfusion is essential to decreasing morbidity and mortality, as every minute after acute ischemic stroke has been estimated to result in the loss of approximately two million neurons.2 Many factors contribute to outcomes in acute ischemic stroke patients following mechanical thrombectomy.
Moderate conscious sedation and general anaesthesia with intubation are the two most commonly used techniques in anaesthesia for patients of acute ischemic stroke undergoing mechanical thrombectomy.3 Physicians preferring general anaesthesia over conscious sedation often cite factors such as decreased patient movement, perceived procedural safety, and improved procedural efficacy.3 Advantages in conscious sedation include the ability to continuously monitor the patient's neurologic status, haemodynamic stability, and decreased procedural time.4 There exists much debate regarding which anaesthesia strategy, general anaesthesia or conscious sedation, results in improved patient outcomes.5 ,6 We evaluated a large inpatient database to study in-hospital outcomes of patients of acute ischemic stroke who are undergoing general anaesthesia or conscious sedation during mechanical thrombectomy.
Methods
Data source and study population
The Perspective database (Premier, Charlotte, North Carolina, USA) is a voluntary, fee-supported collection of data developed to assess the quality and resource usage of healthcare delivery within the USA. As of 2014, the Perspective database consisted of approximately 20% of hospitalisations nationwide and represented more than 2900 US hospitals. Patient demographics, hospital information, diagnoses, procedures, discharge status, and all billed items are recorded in this database.
Patients who presented with acute ischemic stroke (ICD-9-CM diagnostic codes 433.×1 and 434.×1) from 2006 to 2013 were identified from the Perspective database. Patients were only included if the stroke code was listed as the primary hospitalisation diagnosis to avoid including patients with a previous history of stroke. Patients of acute ischemic stroke who underwent thrombectomy during their hospitalisation were identified using ICD-9 procedural code 39.74. Patients who underwent another invasive surgery on the same day as their thrombectomy were identified using ICD-9 procedural codes and excluded from the subsequent analysis to avoid including patients who received anaesthesia for a procedure other than thrombectomy. The following baseline patient characteristics were collected for each patient: age, gender, race, admission status, admission source, Charlson comorbidity index,7 payor, hospital region, hospital number of beds, hospital location, hospital teaching status and tissue plasminogen activator (tPA) administration (ICD-9 procedure code 99.10).
Anaesthesiology classification
Mechanical thrombectomy patients were subclassified by whether they received general anaesthesia or conscious sedation during the thrombectomy procedure. Patients who received general anaesthesia during their procedure were identified if they were billed for (1) anaesthesia billing items (ie, pharmacy, anaesthesiologist time) specifically labeled for general anaesthesia or (2) unspecified anaesthesia billing items and mechanical ventilator billing items (ie, intubation, ventilator). Patients who received conscious sedation during their procedure were identified if they were billed for (1) anaesthesia billing items (pharmacy, anaesthesiologist's time) specifically labeled for conscious sedation or (2) unspecified anaesthesia billing items in the absence of mechanical ventilation billing items. Anaesthesia and mechanical ventilator billing items were only included if they were billed on the same day as the thrombectomy procedure to avoid confounding from other surgical procedures the patient may have undergone during the hospitalisation.
Outcome variables
The primary outcome variables of this study were death during hospitalisation, unfavourable discharge (discharge to hospice, skilled nursing facility, long-term-care hospital, or rehab facility), and discharge to home (self-care or home-care organisation). Secondary outcomes as identified by ICD-9 diagnostic codes were subarachnoid hemorrhage (SAH) or intracranial hemorrhage (ICH) (ICD-9 code 430 or 431), urinary tract infection (UTI) (599), sepsis (785.52, 995.91, 995.92), deep venous thrombosis (DVT) (453.4×), pulmonary embolism (PE) (415.1×), edema (518.4), congestive heart failure (428), and pneumonia. Pneumonia was subclassified into bacterial pneumonia (ICD-9 code 481, 482.×, 486), ventilator-associated pneumonia (997.31), other respiratory complications (997.39), and aspiration pneumonia (507.×). Complications identified from ICD-9 diagnostic codes were only included if they were listed as not present on admission to avoid including complications that occurred before the hospitalisation. Total length of stay and hospitalisation costs were examined.
We also studied trends in usage of general anaesthesia versus conscious sedation from 2006 to 2012. We determined the proportion of patients receiving general anesthesia (GA) and conscious sedation (CS) at high-volume and low-volume centres between 2007 and 2012. High-volume centres were defined as those in the 75 percentile or above for mechanical thrombectomy treatments per year. Criteria for high-volume centres differed by year as in 2007, high-volume centres were defined as centres performing ≥7 cases, in 2008, high-volume centres performed ≥6 cases, in 2009, high-volume centres performed ≥7 cases, in 2010 high-volume centres performed ≥6 cases, in 2011, high-volume centres performed ≥9 cases, and in 2012, high-volume centres performed ≥13 cases. We also determined the proportion of centres using conscious sedation from 2007 to 2012. Data from 2013 were not included in this trends analysis as only first-quarter data were available.
Propensity score analysis
Propensity score analysis was performed using the MatchIt package in R as previously described.8 Propensity scores representing the probability of receiving general anaesthesia were calculated for each patient in the general anaesthesia and conscious sedation groups using a logistic regression model. The covariates used to generate these propensity scores included patient variables (age, gender, race, admission status and source, Charlson comorbidity score7 and payor), and hospital variables (region, number of beds, urban or rural location, and teaching or non-teaching status). Following propensity score generation, recipients of general anaesthesia and conscious sedation underwent 1:1 nearest-neighbour (Greedy-type) matching of the logit of the propensity score with a caliper width of 0.25. Matching was performed without replacement, and unpaired patients not meeting matching criteria were excluded. Each propensity score-derived matched pair was assigned a unique pair ID using an R script. Improvement in covariate balance following matching was determined using conditional logistic regression, conditioned on the pair ID. ORs of primary and secondary outcomes were calculated following matching using Fisher's exact test.
Statistics
Data were extracted from the Perspective database using SAS (SAS, V.9.3; SAS Institute, Cary, North Carolina, USA) and analysed using JMP (V.9, SAS Institute) and R (V.2.15, R Foundation for Statistical Computing, Vienna, Austria). Continuous results are presented as median and IQR to account for non-parametric data distributions. Categorical results are presented as relative frequencies (%). Patient, procedure and hospital covariates and outcome incidences were compared between general anaesthesia and conscious sedation groups using Wilcoxon rank-sum test for continuous variables and Fisher's Exact test for categorical variables.
Results
Patient demographics
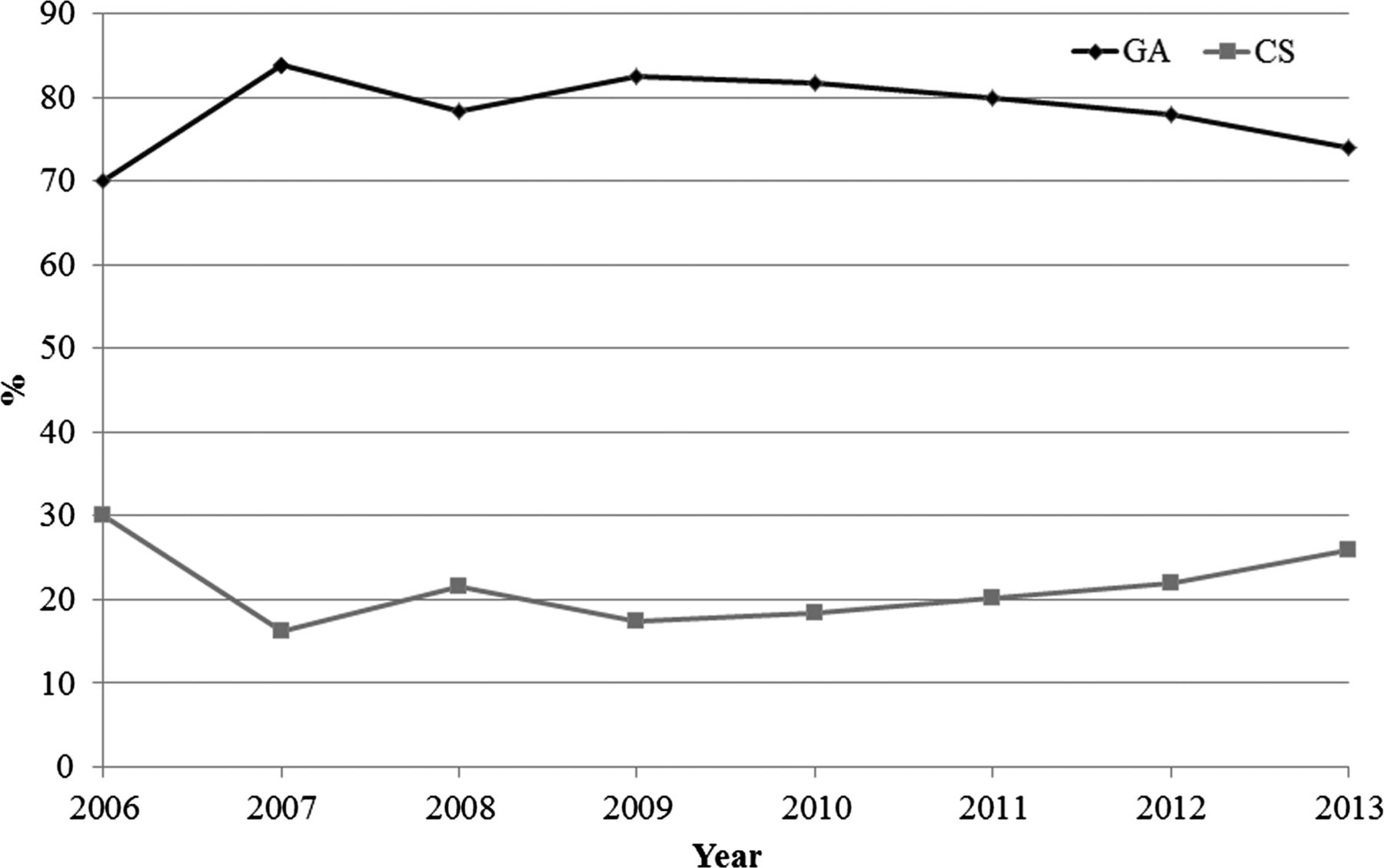
A total of 2512 patients with acute ischemic stroke who underwent thrombectomy at 108 unique medical centres were identified within the Perspective database from 2006 to 2013 (table 1). Of those patients, 1999 (80%) received general anaesthesia and 513 (20%) received conscious sedation for their thrombectomy procedure. Utilization rate of general anaesthesia was 70% in 2006 and 74% in 2013. Utilization rate of conscious sedation was 30% in 2006 and 26% in 2013 (figure 1). The proportion of centres using conscious sedation increased between 2007 and 2012 as 48% of centres in 2007, 2008 and 2009 used conscious sedation on at least one patient, 57% of centres in 2010 used conscious sedation on at least one patient, and 59% of centres in 2011 and 2012 used conscious sedation on at least one patient. Patients at high-volume centres were more likely to receive general anaesthesia, as 83.1% of high-volume-centre patients received general anaesthesia and 16.9% received conscious sedation compared with 72.5% of patients receiving general anaesthesia and 27.5% receiving conscious sedation at low-volume centres (p<0.0001). Patients who received general anaesthesia were more likely to be transferred from another medical centre and were more likely to be classified as emergency admissions compared with patients who received conscious sedation. The majority of thrombectomy procedures were performed at urban medical centres (2433, 97%) and teaching hospitals (1620, 64%). Utilization rate of tPA was similar between the general anaesthesia and conscious sedation groups (56% vs 57%, p=0.55).
Patient and hospital demographics of unmatched patients
{kind=link}
Usage rate of general anaesthesia and conscious sedation among patients of mechanical thrombectomy: 2006–2013.
Following 1:1 matching by the propensity score of the likelihood of receiving general anaesthesia during thrombectomy, 507 general anaesthesia and 507 conscious sedation patients were matched based upon similarities in their demographic and clinical characteristics (table 2). Following matching, most covariates were statistically similar between the two groups, with significant differences remaining in Charlson score (p=0.0300), hospital region (p=0.0008) and hospital bed size (p=0.0170).
Patient and hospital demographics of patients matched by propensity score
Propensity score-adjusted outcomes
Propensity score-adjusted outcome incidence rates and ORs are shown in table 3. Following 1:1 matching, thrombectomy patients, who received general anaesthesia during their procedure, had significantly higher rates of in-hospital mortality (25% vs 12%, OR=2.37 (95% CI 1.68 to 3.37), p<0.0001), pneumonia (17% vs 9.3%, OR=2.00 (1.35 to 2.99), p=0.0005), and sepsis (3.9% vs 1.4%, OR=2.93 (1.18 to 8.28), p=0.0170) compared with thrombectomy patients, who received conscious sedation. Recipients of general anaesthesia also had non-significantly higher rates of UTI (11% vs 7.9%), DVT (1.8% vs 0.8%), PE (0.8% vs 0%), and congestive heart failure (2.0% vs 0.6%) compared with recipients of conscious sedation. No differences in ICH/SAH rates were seen between recipients of general anaesthesia and recipients of conscious sedation (11% vs 12%, p=0.62). Median hospitalisation costs were US$26 775 (IQR=18 790–39 935) for recipients of conscious sedation, and US$34 903 (IQR=25 530–55 444) for recipients of general anaesthesia (p<0.0001). Median length of stay was significantly lower for recipients of conscious sedation (6 days, IQR=4–11 days), compared with recipients of general anaesthesia (8 days, IQR=5–13 days) (p<0.0001).
Patient outcomes following 1:1 matching by propensity score
Discussion
Our study of a multihospital inpatient database demonstrated that mechanical thrombectomy patients receiving conscious sedation have decreased in-hospital mortality and decreased rates of pneumonia complications when compared with recipients of general anaesthesia. Recipients of conscious sedation were significantly more likely to have unfavourable discharge (discharge to locations other than home) than their general anaesthesia counterparts. However, the relative increase in unfavourable discharge among recipients of conscious sedation was less than the relative decrease in in-hospital mortality. Hospital costs and lengths of stay were also lower in patients who received conscious sedation. Over the course of the study time-period, conscious sedation was used in roughly 20% of patients, and usage of conscious sedation did not change substantially between 2006 and 2013. Given the significantly lower rate of in-hospital mortality among recipients of conscious sedation, these findings suggest that conscious sedation may be underutilized during the treatment of acute ischemic stroke.
A number of factors likely contribute to the higher mortality rates seen in the general anaesthesia group. Previous studies have demonstrated that inhalational and intravenous anaesthetic agents can profoundly reduce cerebral blood flow with the risk of causing cerebral hypoperfusion and increased ischemic injury.9 ,10 Anaesthetic agents such as isoflurane have been found to increase intracranial pressure by inducing cerebral vasodilatation,9 ,11 which could steal flow from ischemic areas with poor autoregulation. Induction and recovery phases of general anaesthesia are often associated with significant haemodynamic changes (hypotension and rapid blood pressure fluctuations) that could exacerbate ischemic injury.12 Some studies have found that induction of general anaesthesia is associated with delays in reperfusion, potentially resulting in increased morbidity and mortality.13 ,14 By contrast, conscious sedation allows for intraprocedural monitoring of neurological deficits, which could allow the operator to adjust the treatment strategy if needed.15 Assessment of neurological status during the procedure allows the operator to assess both neurologic and angiographic outcomes.16 Midazolam sedation has been found to preserve dynamic cerebral autoregulation, which could contribute to decreased volatility in intraprocedural cerebral perfusion.17
Yet, as demonstrated in our study, general anaesthesia remains the favoured method of administration of anaesthesia for intra-arterial treatment of acute ischemic stroke. The main argument in favour of general anaesthesia is decreased patient movement during the procedure.5 Patients who are awake during endovascular treatment may move during endovascular therapy, thus limiting the ability of the interventionalist to interpret the angiographic images and catheterise the cerebral vessels.18 Patient movement during the procedure can also result in wire perforation which could result in significant vascular injury and intracranial haemorrhage. However, no studies have demonstrated that conscious sedation is associated with higher rates of wire perforation or intracranial haemorrhage than general anaesthesia.19 ,20 Additionally, many practitioners cite perceived procedural safety, specifically, avoiding emergent endotracheal intubation, as an advantage of general anaesthesia over conscious sedation.3 Emergent intubation is associated with a number of complications including airway trauma, aspiration and death.21 ,22 However, a number of previous studies have suggested that the potential need for emergent endotracheal intubation among patients receiving conscious sedation and receiving neuroendovascular therapies is relatively low.20 ,23–25 Jumaa et al20 found that less than three percent of mechanical thrombectomy patients receiving conscious sedation required intraprocedural emergent intubation.
A number of previous studies have demonstrated superior outcomes for mechanical thrombectomy patients receiving conscious sedation relative to those receiving general anaesthesia. Abou-Chebl et al19 found that patients receiving general anaesthesia during mechanical thrombectomy procedures had higher rates of poor neurologic outcome at 90 days, and higher mortality when compared with patients receiving conscious sedation. Davis et al26 found that conscious sedation/local anaesthesia was an independent predictor of good neurological outcome even when controlling for initial stroke severity and time to reperfusion. Li et al13 found higher rates of mortality among patients receiving general anaesthesia when compared with patients receiving conscious sedation. Nichols et al27 found that increasing levels of sedation and pharmacologic paralysis were associated with higher rates of mortality and lower rates of successful angiographic reperfusion. Jumaa et al20 found that patients receiving conscious sedation had lower rates of in-hospital mortality, higher rates of good clinical outcome, and smaller final infarct volumes. Use of general anaesthesia was independently associated with worse outcomes despite comparable rates of recanalisation among patients included in the North American SOLITAIRE stent retriever registry.28 Finally, a systematic review of studies comparing the use of general anaesthesia and conscious sedation found that patients receiving general anaesthesia experienced poorer outcomes than patients receiving conscious sedation receiving mechanical thrombectomy.29 One recently published study demonstrated that over 80% of patients of mechanical thrombectomy could be safely treated while under conscious sedation with high rates of good neurologic outcome.30 These studies, along with the findings from our study, suggest that conscious sedation is safe and effective in the setting of mechanical thrombectomy for acute ischemic stroke, and can be safely used in a majority of patients.
Limitations
The main strength of our analysis is the size of the population analysed, and the representation of a wide range of practices across the country. Our study has limitations. Because our patient population is from an administrative database, a number of important clinical variables were not available, and thus, not included in the propensity score model. Data on initial stroke severity, time to treatment, blood glucose, blood pressure during and after the procedure, and location of occlusion were not available. Selection bias is a possibility, as it is likely that patients with more severe strokes received general anaesthesia, or were intubated before the procedure due to an inability to preserve airway patency. We did not include the device type in our propensity score analysis, as this information was not always included in the billing data. Furthermore, important outcomes, such as recanalisation, preoperative and postoperative NIH Stroke Scale (NIHSS) scores, and long-term post-hospitalisation neurological status, are not available. Coding errors are a potential limitation of our study.
Conclusions
Our study of a multihospital administrative database found that mechanical thrombectomy patients receiving conscious sedation had significantly lower rates of in-hospital mortality when compared with patients receiving general anaesthesia. General anaesthesia was used in approximately 80% of mechanical thrombectomy patients. Further studies, including randomised controlled trials, are needed to determine if general anaesthesia is associated with higher rates of complications and impaired neurological outcome for acute ischemic stroke patients receiving mechanical thrombectomy. In the meantime, when deemed possible, it is reasonable to favour conscious sedation over general anaesthesia during acute endovascular stroke therapy based on available collective evidence.
References
Footnotes
Contributors All authors contributed to the writing of the manuscript. WB and JSM contributed to data analysis. All authors contributed to interpretation of results.
Competing interests HJC: Grants: Cordis Endovascular*. DFK: Consultancy: ev3,* Medtronic,* Codman*; Grants/Grants Pending: ev3,* MicroVention,* Sequent,* Codman*; Payment for Lectures (including service on speakers bureaus): MicroVention*; Royalties: UVA Patent Foundation*; Payment for Development of Educational Presentations: ev3*; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: MicroVention.* GL: Consultancy: Edge Therapeutics; Payment for Development of Educational Presentations: Covidien/ev3*; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Boston Biomedica Associates
*Money paid to institution.
Ethics approval Because these data were from a publicly available and deidentified administrative database, this study was exempted from IRB approval.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Authors are happy to provide additional tables and findings to anyone interested.