Article Text

Abstract
Objective Utilization of the Pipeline embolization device (PED) in complex ruptured aneurysms has not been well studied. We evaluated the safety and effectiveness data from five participating US centers.
Methods Records of patients with ruptured cerebral aneurysms who underwent PED treatment between 2011 and 2013 were retrospectively reviewed.
Results 26 patients with ruptured aneurysms underwent PED treatment (mean age 51.4±13.2 years;16 women). At presentation, 8 patients (30.8%) had a Hunt–Hess grade of IV or above; 11 required extraventricular drain placement. Aneurysm morphologies were: 8 dissecting, 8 blister-like, 6 fusiform, and 4 saccular. There were 22 anterior circulation and 4 posterior circulation aneurysms. PED deployment was successful in all patients, with adjunctive coiling utilized in 12. Periprocedural complications occurred in 5 (19.2%), including 3 inhospital deaths. 23 patients (88.5%) had postoperative angiography at a mean of 5.9 months: 18 aneurysms (78.3%) were completely occluded, 3 (13.0%) had residual neck filling, and 2 (8.7%) had residual dome filling. All blister-type aneurysms were completely occluded at follow-up. Clinical follow-up was available for an average of 10.1 months (range 2–21 months), with one asymptomatic in-stent stenosis and one asymptomatic thromboembolic stroke noted. Good outcome (modified Rankin Scale (mRS) score of 0–2) was achieved in 20 patients (76.9%), fair (mRS 3–4) in 3 (11.5%), and 3 died (11.5%).
Conclusions The PED can be utilized for ruptured aneurysms and is a good option for blister-type aneurysms. However, due to periprocedural complications, it should be reserved for lesions that are difficult to treat by conventional clipping or coiling.
- Aneurysm
- Hemorrhage
- Flow Diverter
Statistics from Altmetric.com
Introduction
The use of flow diversion via a Pipeline embolization device (PED; Covidien, Irvine, California, USA) for the treatment of intracranial aneurysms has gained notable acceptance over recent years. The PED is a self-expanding stent composed of cobalt, chromium, and platinum, and encompasses 48 braided strands of 28–33 μm in diameter. This device differs from regular intracranial stents by providing 30–35% metal surface area coverage and hemodynamically diverting blood flow away from the aneurysm dome. The PED promotes gradual intra-aneurysmal flow stasis and thrombosis, as well as subsequent remodeling of the parent vessel with regression of the aneurysm.1 ,2 After the publication of promising results from large multicenter clinical trials,3 ,4 the US Food and Drug Administration approved utilization of the PED for the treatment of large or giant wide necked aneurysms of the internal carotid artery (ICA) from the petrous to the superior hypophyseal segments. Moreover, the utilization of flow diverters such as the PED could theoretically result in better aneurysm neck reconstruction, and a recent case controlled analysis showed that the PED could provide a higher rate of aneurysm occlusion than coiling.5
Early reports of the use of the PED for intracranial aneurysm treatment were largely focused on non-ruptured cases.1 ,2 ,4 ,6–8 PED treatment has not been widely attempted in ruptured cases because patients with aneurysmal subarachnoid hemorrhage (SAH) may require additional intracranial procedures, such as extraventricular drain (EVD) placement, ventriculoperitoneal shunt (VPS) insertion, and craniotomy for decompression or hematoma evacuation, which could be complicated by the dual antiplatelet therapy required in conjunction with such treatment.1 Nevertheless, certain cases of ruptured aneurysms, such as dissecting, giant, fusiform, or blister aneurysms, may pose difficult anatomical and technical challenges for both standard surgical and endovascular techniques; thus, the specific, targeted use of flow diversion in these situations may be warranted. Several investigators recently reported successful application of PED in ruptured aneurysms with a reasonable complication rate.9–11 Here we present data from five participating US centers on the use of PED for patients with SAH and aneurysms that would be considered challenging for conventional modalities in order to evaluate the safety and efficacy of this modality.
Patients and methods
Population, setting, and study design
The study included a consecutive surgical series of patients with SAH who underwent PED placement for the treatment of ruptured aneurysms at five North American neurosurgical centers between 2011 and 2013. In accordance with an institutional review board approved protocol at each of the centers, the medical records of these patients were retrospectively reviewed to obtain demographic and clinical information, such as age at presentation, sex, medical comorbidities, Hunt–Hess (HH) grade, Fisher grade, and results of radiographic studies, including CT, MRI/angiography, and digital subtraction angiography (DSA). Treatment course variables included the number of PEDs utilized, use of adjunct coil placement, and periprocedural (<30 days) and late (>30 days) complications. The PED was utilized as the primary treatment modality to secure the ruptured aneurysm during the initial interventional procedure (ie, immediate placement) or placed in a delayed fashion after the aneurysm was first treated by conventional endovascular or surgical means (ie, delayed placement).
Data measurement
Clinical outcome was measured by the modified Rankin Scale (mRS) score (favorable outcome, 0–2). Radiographic results were measured by degree of aneurysm thrombosis at the time of follow-up angiography. Angiographic outcome was evaluated according to the 3 point classification system established by Roy et al.12
Treatment protocol
All five participating centers had adopted similar protocols in terms of treating ruptured aneurysms and deploying PEDs. Briefly, all patients with SAH were evaluated in the emergency room by neurosurgeons, and EVDs were inserted for patients with an HH grade of III or above and those with clinical or radiographic evidence of hydrocephalus. Non-invasive imaging and DSA images were evaluated by both neurosurgical and endovascular teams at each center to determine the best treatment option for a specific aneurysm. If the aneurysm was deemed best treated with PED, all other invasive procedures (including EVD placement and central line insertion) were performed prior to the administration of any antiplatelet agents and at least 12 h before PED treatment. Patients received a loading dose of 650 mg of aspirin and 600 mg of Plavix (Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership, Bridgewater, New Jersey, and Princeton, New Jersey, USA) before intervention and were maintained on a daily regimen of 325 mg of aspirin and 75 mg of Plavix after PED placement. Aspirin responses and Plavix responses were regularly checked and maintained with aspirin responses <550 and Verify Now P2Y12 reaction units assay (Accumetrics, San Diego, California, USA) scale at least <200 and >50, respectively (60 mg of prasugrel were administered as a loading dose if the patient was a Plavix non-responder). Intraoperatively, a biaxial or triaxial system was usually employed to maintain stability of the construct, and a Marksman microcatheter (ev3/Covidien) was utilized for PED deployment. Heparin was routinely given when dome protection was achieved (ie, after adjunctive coils were placed or, if no coils were utilized, after placement of the first PED). Patients are kept on aspirin for life, and dual antiplatelet therapy was continued for at least 3 months for each aneurysm type and could be extended if the aneurysm was giant or fusiform, thus requiring a longer time period for endothelialization.
Statistical methods
The association between demographic and clinical risk factors and periprocedural complication rate as well as favorable outcome (mRS 0–2) was evaluated using χ2 and two tailed t tests for categorical and continuous variables, respectively. Statistical significance was defined as a type I error <0.05. All statistical analyses were performed using SAS V.9.2 (SAS Institute Inc, Cary, North Carolina, USA) and Excel 2007 (Microsoft Corp, Redmond, Washington, USA).
Results
Descriptive and outcome data
During the study period, 26 patients with 26 ruptured intracranial aneurysms were treated with PEDs at five participating US centers. Detailed information for each patient is listed in table 1. Demographic and clinical data are summarized in table 2. Representative cases are presented as illustrative case Nos 1–3 (Figures 1⇓–3). There were 16 women and 10 men, and mean age of the 26 patients at the time of PED placement was 51.4±13.2 years (range 19–75 years). Eight patients (30.8%) presented with an HH grade of IV or V and 17 patients (65.4%) with a Fisher grade of III or IV. Eleven patients (42.3%) required EVD placement on presentation.
Patients with ruptured aneurysms treated with the Pipeline embolization device
Demographic and clinical characteristics of the patient population

Illustrative case No 1 (patient No 10 in table 1). Ruptured paraclinoid internal carotid artery (ICA) dissecting aneurysm. This patient presented to an outside institution with sudden onset of severe headache and subsequent obtundation. The patient was intubated and transferred urgently for evaluation. Head CT scan (A) showed diffuse subarachnoid hemorrhage (Fisher grade 3), and brain CT angiogram (B) demonstrated a large left ICA paraclinoid aneurysm, measuring 18 mm×13 mm. An extraventricular drain (EVD) was emergently placed before the patient was transferred to the neuroangiography suite. Diagnostic cerebral angiogram (C, anteroposterior view; D, lateral view) revealed a left ICA dissecting aneurysm with a non-discernible neck. The aneurysm was treated with one Pipeline embolization device (PED) (3.75 mm×25 mm) and adjunctive coiling. During treatment, an intraluminal thrombus was noted after deployment of the PED (E, asterisk), and was treated with intra-arterial eptifibatide with good effect (F). Final angiographic image demonstrated no significant aneurysm filling (G). The patient's neurological status rapidly improved. The patient was weaned off the EVD 10 days later and discharged home with minimal neurological symptoms (modified Rankin Scale score of 1). Follow-up angiogram at 6 months shows no residual filling of the aneurysm (H).
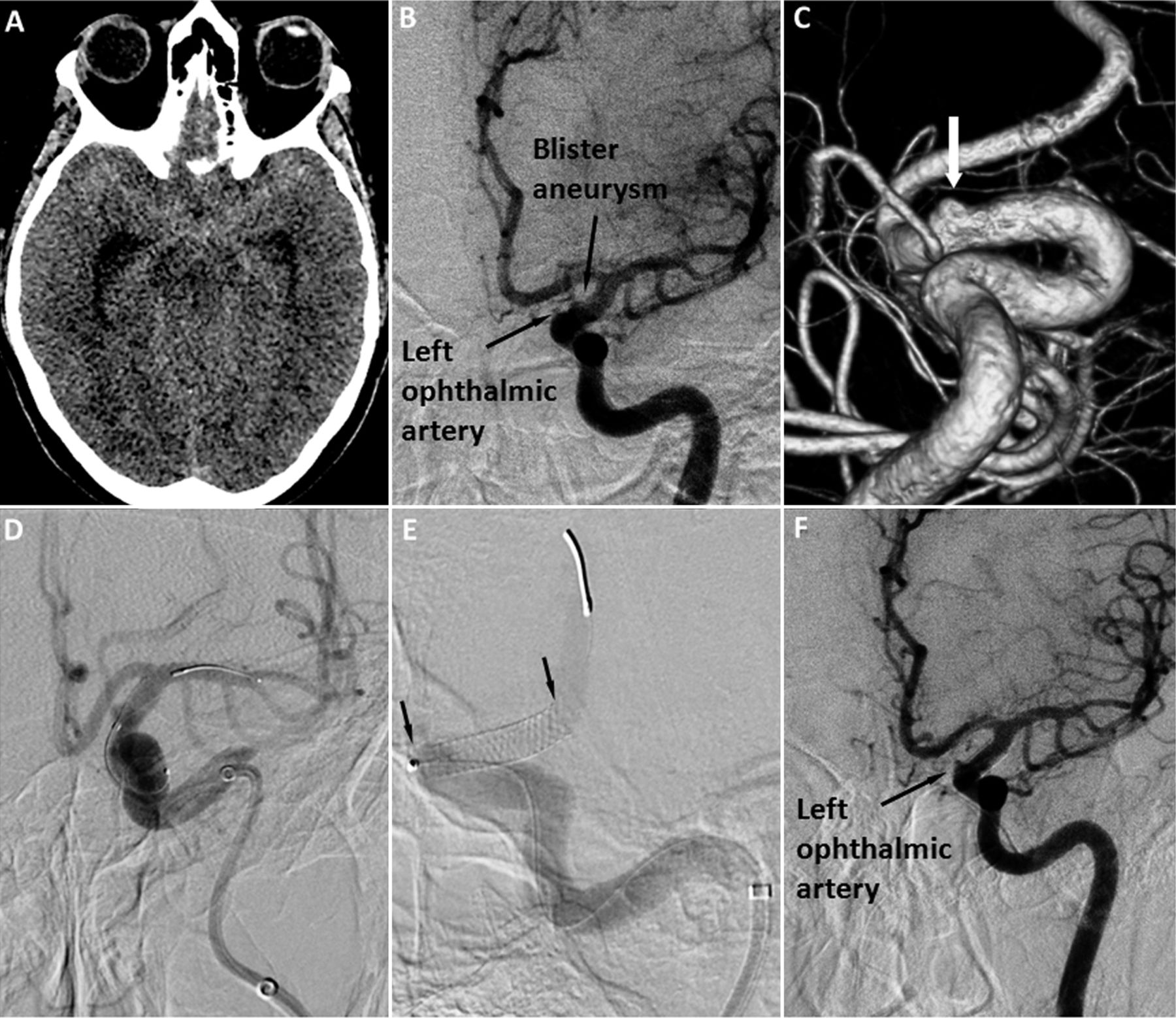
Illustrative case No 2 (patient No 5 in table 1). Ruptured blister aneurysm. This patient presented with Hunt–Hess grade I and Fisher grade 2 subarachnoid hemorrhage (A). Initial CT angiogram was suspicious for a left internal carotid artery (ICA) blister aneurysm, which was confirmed on diagnostic angiography (B) and three-dimensional reconstruction (C, arrow). A single Pipeline device (3.75 mm×14 mm) was deployed at the ophthalmic segment of the left ICA, covering the aneurysm neck (D, working view during Pipeline embolization device (PED) deployment; E, entire PED deployed). There was immediate aneurysm obliteration, and the follow-up angiogram at 3 months shows no aneurysm filling, good remodeling of the supraclinoid ICA, and a patent ophthalmic artery (F). The patient made a good recovery and was asymptomatic at the time of the 3 month follow-up evaluation (modified Rankin Scale score of 0).

{kind=link}
{kind=link}
{kind=link}
Illustrative case No 3 (case No 9 in table 1). Ruptured vertebral artery (VA) dissecting aneurysm. This patient presented with Hunt–Hess grade IV, Fisher grade 3 subarachnoid hemorrhage (A) from a ruptured right VA dissecting aneurysm. An extraventricular drain (EVD) was emergently placed before the patient was transferred to the neuroangiography suite. Diagnostic angiography showed a right VA dissection aneurysm (B, anteroposterior projection; C, three-dimensional reconstruction). The patient had a dominant right VA and a hypoplastic left VA, and therefore reconstruction of the right VA via the Pipeline embolization device (PED) was preferred in comparison with surgical or endovascular sacrifice of the right VA. The patient was treated with a single Pipeline device (2.5 mm×20 mm) without complications (D, working view during PED deployment; E, control angiogram after PED deployment). The patient was eventually weaned off the EVD and discharged to a rehabilitation facility with mild dysarthria and gait instability. Follow-up angiogram at 3 months (F) shows no residual filling of the aneurysm and good remodeling of the right VA. The patient made a good recovery and had mild dysarthria at the time of the 3 month follow-up evaluation (mRS score of 1).
Most aneurysms in the study cohort were located along the ICA: 15 at the paraclinoid segment and five at the posterior communicating artery segment. One aneurysm arose from the M1 segment of the middle cerebral artery, one from the A1 segment of the anterior cerebral artery, three from the vertebral artery, and one from the basilar artery. Overall, eight patients had dissecting aneurysms, eight had blister-like aneurysms, four had saccular aneurysms, and six had fusiform aneurysms. The average size of all aneurysms was 9.1 (±7.1) mm; if blister aneurysms were excluded, mean aneurysm size for the dissecting, saccular, and fusiform aneurysms was 12.2 (±6.4) mm.
PED deployment was successful in all 26 patients, with coils utilized in 12 cases (table 1). Twenty patients received one PED during treatment, and six others received two or more PEDs. Eighteen patients had PED placement during the first aneurysm embolization procedure whereas eight patients initially underwent endovascular coiling in an attempt to protect the aneurysm dome and a PED was placed in a delayed fashion. All patients who had delayed PED placement received flow diversion treatment during the same hospitalization or within 4 weeks after the initial coiling procedure.
Of 11 patients who required EVD placement on admission, eight had an EVD successfully weaned during hospitalization; but one of them (patient No 26, table 1) developed delayed hydrocephalus and underwent VPS placement approximately 6 weeks after PED treatment. Plavix was held periprocedurally for the VPS procedure. For the three other patients (patient Nos 1, 2, and 16) who had EVD insertion and failed EVD weaning, the aneurysms were initially treated by coiling, and shunts were placed between post-bleeding days 15 and 20, after the vasospasm period. PED treatments for these three patients were carried out as planned procedures 1–2 weeks after VPS placement.
Periprocedural complications, radiographic outcome, and follow-up data are summarized in table 3. Twenty-three patients (88.5%) had postprocedural angiography at a mean of 5.9 months (range 0.5–16.8 months) after PED placement: 18 aneurysms (78.3%) had complete occlusion, three (13.0%) had residual filling at the neck, and two had residual filling at the aneurysm dome (8.7%). Specifically, all eight patients with blister aneurysms had follow-up DSA, and all had complete occlusion of the aneurysm. Two patients required additional aneurysm treatment: one with a giant recurrent saccular ICA aneurysm (patient No 14, table 1) had residual filling of the aneurysm dome 5 months after PED placement and underwent microsurgical bypass and parent vessel sacrifice, and the other (patient No 16, table 1) with a fusiform vertebral artery aneurysm needed a second PED placement 6 months after the initial embolization procedure. Of note, patient No 14 had been previously treated with an Enterprise stent (Codman & Shurtleff Inc, Raynham, Massachusetts, USA), which could decrease the effectiveness of PED treatment.1 ,7
Periprocedural neurological complications and clinical outcome
Periprocedural neurological complications occurred in five patients (19.2%). One patient (patient No 19, table 1) had an asymptomatic EVD tract hemorrhage after PED aneurysm treatment, and another (patient No 10) developed in-stent thrombosis during the procedure, which resolved after administration of an eptifibatide bolus, and this patient suffered no clinical complications as a result. There were three (11.5%) inhospital deaths. Patient No 22 developed diffuse brainstem ischemia on the same day after uneventful PED placement for a fusiform basilar trunk aneurysm, and care was withdrawn. Patient No 23 died of re-hemorrhage on day 1 after PED treatment. The embolization procedure for this patient was complicated by in-stent thrombosis, which resolved after microcatheter infusion of intra-arterial tissue plasminogen activator. Patient No 12 presented with non-responsiveness and diffuse SAH from a large dissecting aneurysm at the A1 segment of the anterior cerebral artery. Endovascular treatment was performed uneventfully, but the family eventually decided to withdraw care after no improvement of neurological status.
Clinical follow-up was available for a mean of 10.1 months (range 2–21 months for the remaining 23 patients). During the follow-up period, adverse events occurred in two cases, both of whom were asymptomatic and needed no intervention. Patient No 17 was found to have asymptomatic in-stent stenosis during follow-up DSA and was monitored with serial non-invasive imaging, and patient No 21 had a silent right thalamic stroke and antiplatelet therapy was continued. Four patients developed hydrocephalus unrelated to PED treatment and required VPS placement. These procedures were performed either before delayed PED treatment or at least 6 weeks after PED placement to avoid operating with dual antiplatelet therapies. The mRS score was 0–2 for 20 patients (76.9%) at the latest clinical follow-up visit. Three patients (patient Nos 14, 15 and 26, table 1) had fair outcome (mRS score of 3 or 4), and three patients were deceased (mRS score of 6). Statistical analyses showed that no particular demographic or clinical factor, including age, HH grade, or adjunctive coil usage, was significantly associated with a favorable clinical outcome or the development of periprocedural complications.
Discussion
Flow diversion via the PED has become an important tool for intracranial aneurysm management, and its utility in treating large, wide necked, and anatomically challenging aneurysms has been well documented.3–8 ,13–15 Endoluminal therapy with a flow diversion device, such as the PED, can lead to better neck reconstruction and a lower rate of recanalization, features that are greatly beneficial for the treatment of ruptured aneurysms. However, similar to other intracranial stents, the utilization of flow diversion stents requires dual antiplatelet therapy, which can increase the risk of hemorrhage for other procedures that may be necessary for the overall management of SAH. Additionally, PED treatment does not result in immediate aneurysm occlusion or complete dome protection (albeit with decreased flow into the aneurysm sac, there is likely partial dome protection after PED deployment); and in the immediate periprocedural phase, the risk of re-hemorrhage is theoretically higher because the patient is subjected to dual antiplatelet therapy and anticoagulation for microcatheter manipulation. These concerns may contribute to a general sense of reluctance to use PEDs in the setting of SAH. However, there are a small number of ruptured aneurysms that are morphologically challenging for either approach (eg, blister-type aneurysms), and PED utilization may confer an advantage in such scenarios. These cases are rare, and our series represents the largest collection across five different US centers and therefore provides a platform to evaluate the safety profile and efficacy of the application of PEDs in the setting of SAH.
Key results and interpretation
In this retrospective observational study, we aimed to assess the safety and efficacy of utilizing PEDs to treat ruptured intracranial aneurysms that were anatomically challenging for both clipping and coiling. We evaluated 26 patients with aneurysmal SAH who were treated with PEDs at five US centers and found that 18 aneurysms were completely occluded at a mean follow-up of 5.9 months (69.2%) and 20 patients (76.9%) had a favorable outcome (mRS of 0–2) with a mean follow-up of 10.1 months. There were three inhospital deaths, two of which were treatment related (one re-hemorrhage and one brainstem ischemic stroke), and two other neurological complications. These findings are consistent with reports from several other groups. Cruz et al9 reported on a series of 20 patients who presented with SAH and were treated with PED at four Canadian centers and reported occlusion rates of 75% and 94% at 6 and 12 months, respectively; 15 patients (75%) were independent (Glasgow Outcome Scale score of 4 or 5) at a median follow-up of 179 days. There were three periprocedural deaths, with one resulting from re-hemorrhage after treatment, as well as three other technical complications. The authors also noted one case of treatment failure in which the aneurysm grew despite placement of the one PED, which necessitated the placement of two more overlapping devices 8 days after the initial intervention. McAuliffe and Wenderoth11 described a smaller series of 11 SAH patients with PED treatment and reported an occlusion rate of 72.7% at 6 months and favorable outcome (mRS of 0–2) in eight patients (72.7%). Two patients died due to re-hemorrhage; neurological complications occurred in two other patients during the periprocedural phase, but none during the follow-up. In addition, de Barros Faria et al10 studied 23 patients with intracranial dissecting aneurysms, 12 of whom presented with acute SAH, and reported an occlusion rate of 69.5% and favorable outcome (Glasgow Outcome Scale score of 4 or 5) in 17 patients (74%).
Generalizability
These results collectively suggest that flow diversion via a PED can be utilized safely for the treatment of patients with selective ruptured aneurysms considered challenging by conventional microsurgical or endovascular therapies, and can result in clinical outcomes similar to those associated with conventional endovascular therapies.16 Moreover, the occlusion rate of approximately 70% after PED treatment across multiple studies compares favorably with the reported total occlusion rates of coiled saccular aneurysms in the current literature.17 Considering that follow-up angiography in our series was performed at a mean of 5.9 months, the long term occlusion rate will likely be higher.7 In particular, all eight cases of blister aneurysms had post-treatment angiograms, all of which showed complete obliteration, indicating that flow diversion via PED was an especially effective method for the treatment of these challenging lesions.
With respect to the re-rupture rate after PED deployment, the risk of treatment failure or re-hemorrhage was 3.8% (one of 26 cases) in our series, 10% in the study of Cruz et al9 (two of 20 cases, including one case of post-PED aneurysm enlargement requiring retreatment), 18.2% (two of 11) in McAuliffe and Wenderoth's study,11 and 0% in the study of de Barros Faria et al.10 In fact, four of the five treatment failure cases described in our and previous studies involved PED placement without adjunctive coiling, and we believe that such a risk could be reduced by using coils in conjunction with PEDs. Coiling and flow diversion should be considered complementary, rather than competitive techniques, and using adjunctive coils in aneurysms with reasonable dome size (ie, not blister-type) can provide immediate dome protection. When coils were used, the goal was to loosely pack the aneurysm dome to promote thrombosis, rather than to achieve dense packing of the aneurysm. Moreover, although the risk of hemorrhage during EVD or VPS placement was thought to be substantial in studies of stent assisted coiling for ruptured aneurysms,18 ,19 only one case of asymptomatic EVD track hemorrhage was encountered in our study, probably because all VPS procedures were performed either before PED treatment or in a delayed fashion when Plavix could be temporarily discontinued.
Another possible technical complication associated with Pipeline embolization is device migration or foreshortening,20 which can be catastrophic if the aneurysm neck becomes exposed. Although this complication did not occur in our series, McTaggart et al21 reported a case of PED retraction in the setting of severe post-SAH vasospasm in a patient with a ruptured dissecting posterior inferior cerebellar artery aneurysm, and the placement of a second PED was also complicated by vasospasm. This case highlights the important of accurate device placement with anticipation of possible device migration and vigilant angiographic surveillance, especially during the vasospasm period.
Limitations
Several limitations need to be considered while interpreting these results. We conducted a multicenter, retrospective, observational study, and therefore there is inherent selection bias associated with the study. We observed a low rate of hemorrhagic complications during other intracranial procedures, such as EVD or VPS placement, which could be due to the small sample size. Furthermore, the relatively recent adoption of PED in clinical use and the short follow-up period in our study imply that the long term durability of the treatment, especially for ruptured aneurysms, is unclear. Nevertheless, our data, as well as the results from other investigators, have demonstrated that the PED is a safe and effective form of treatment for ruptured intracranial aneurysms that are challenging for both conventional microsurgical and endovascular techniques.
Conclusion
The PED can be utilized safely and effectively for ruptured aneurysms that are difficult to treat by conventional clipping or coiling. Blister aneurysms may be particularly effectively treated using flow diversion. Judicious use of coils and vigilant angiographic surveillance may reduce periprocedural complications. Larger scale studies with long term angiographic and clinical follow-up are needed to further elucidate the durability of PED treatment for ruptured aneurysms and afford opportunities for outcome improvement.
Acknowledgments
We thank Paul H Dressel BFA for preparation of the illustrations and Debra J Zimmer for editorial assistance.
References
Footnotes
Contributors NL, AJR, and AHS are responsible for concepts and design. All authors contributed intellectually. All authors acquired, analyzed, and interpreted the data. Statistical analysis was performed by NL and AMB. The manuscript was prepared by NL and AMB. All authors reviewed and made critical revisions to the manuscript.
Competing interests ASA: research grants from Stryker Neurovascular, Terumo MicroVention, Codman Neurovascular, Covidien, and Siemens AG. EIL: shareholder/ownership interests in Intratech Medical Ltd, Mynx/Access Closure, and Blockade Medical LLC; principal investigator for Covidien US SWIFT PRIME Trials; other financial support include Abbott for carotid training for physicians. KML: personal fees from Stryker. DKL: consultant for Covidien and Stryker; shareholder/ownership in Penumbra and Blockade Medical; advisory board for Siemens; principal investigator for Liberty Trial (Penumbra). JM: consultant for Lazarus Effect, Medina Medical, Pulsar Vascular, Reverse Medical, and Edge Therapeutics; investor in Blockade Medical and Medina Medical; advisory board for Codman Neurovascular; grants–NIH 1U01NS086492-01 and NIH 1R01NS078828-01A1. AJR: consulting fees from Stryker, MicroVention, and Covidien/ev3 but has not received any fees or honoraria for any product discussed in this manuscript. AHS: research grants (not related to present study) from National Institutes of Health (co-investigator: NINDS 1R01NS064592-01A1 and NIBIB 5 RO1EB002873-07), University at Buffalo (Research Development Award); financial interests in Hotspur, Intratech Medical, StimSox, Valor Medical, Blockade Medical, and Lazarus Effect; consultant for Codman & Shurtleff Inc, Concentric Medical, Covidien Vascular Therapies, GuidePoint Global Consulting, Penumbra, Stryker Neurovascular, and Pulsar Vascular; speakers’ bureaus for Codman & Shurtleff and Genentech; National Steering Committees for Penumbra 3D Separator Trial, Covidien SWIFT PRIME Trial, and MicroVention FRED Trial; advisory board for Codman & Shurtleff and Covidien Vascular Therapies; honoraria from Abbott Vascular and Codman & Shurtleff Inc for training other neurointerventionalists in carotid stenting and for training physicians in endovascular stenting for aneurysms. KVS: consultant/speakers’ bureau/honoraria, research grant from ev3 and Toshiba; other financial relationship with Abbott Vascular, Boston Scientific, Medtronic, and Zimmer. EV: consultant for Cordis, Codman, Micrus, MicroVention, and Stryker.
Ethics approval Institutional review board approvals were obtained as necessary by each participating center (Capital Health, Rush University, University at Buffalo, University of Tennessee, and Vanderbilt University Medical Center) on the basis of the volume of cases included in this study. Each center followed an institutional review board approved protocol.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data may be available on a per request basis. Requests should be directed to the corresponding author.