Article Text

Abstract
A patient with a giant symptomatic vertebrobasilar aneurysm was treated by endoscopic third ventriculostomy for obstructive hydrocephalus followed by treatment of the aneurysm by flow diversion using a Pipeline Embolization Device. After an uneventful procedure and initial periprocedural period, the patient experienced an unexpected fatal subarachnoid hemorrhage 1 week later. Autopsy demonstrated extensive subarachnoid hemorrhage and aneurysm rupture (linear whole wall rupture). The patent Pipeline Embolization Device was in its intended location, as was the persistent coil occlusion of the distal left vertebral artery. The aneurysm appeared to rupture in a linear manner and contained a thick large expansile clot that seemed to disrupt or rupture the thin aneurysm wall directly opposite the basilar artery/Pipeline Embolization Device. We feel the pattern of aneurysm rupture in our patient supports the idea that the combination of flow diversion and the resulting growing intra-aneurysmal thrombus can create a mechanical force with the potential to cause aneurysm rupture.
- Aneurysm
- Flow Diverter
- Hemorrhage
- Complication
- Hydrocephalus
Statistics from Altmetric.com
Background
Giant symptomatic vertebrobasilar aneurysms are difficult to treat. We present a case of a patient with a giant symptomatic vertebrobasilar aneurysm treated with flow diversion. The patient tolerated the procedure well without new symptoms but died suddenly on post-procedure day 7. We present the anatomical and pathological findings, review previously reported cases and mechanisms for rupture, and discuss potential causes for aneurysm rupture following flow diversion.
Case presentation
An elderly man presented with a 6-month history of progressive gait ataxia, dizziness, and headache with bilateral hyperreflexia and a Romberg's sign on examination. Imaging revealed a giant vertebrobasilar aneurysm with brainstem compression and obstructive hydrocephalus (figure 1). The patient underwent an endoscopic third ventriculostomy for treatment of obstructive hydrocephalus without complications (figure 2), and 1 month later he underwent endovascular treatment of the aneurysm by placement of a Pipeline Embolization Device (PED; ev3/Covidien, Irvine, California, USA) from the basilar artery to the right vertebral artery and coil occlusion of the contralateral left vertebral artery, preserving the origin of the anterior spinal artery (figure 3).
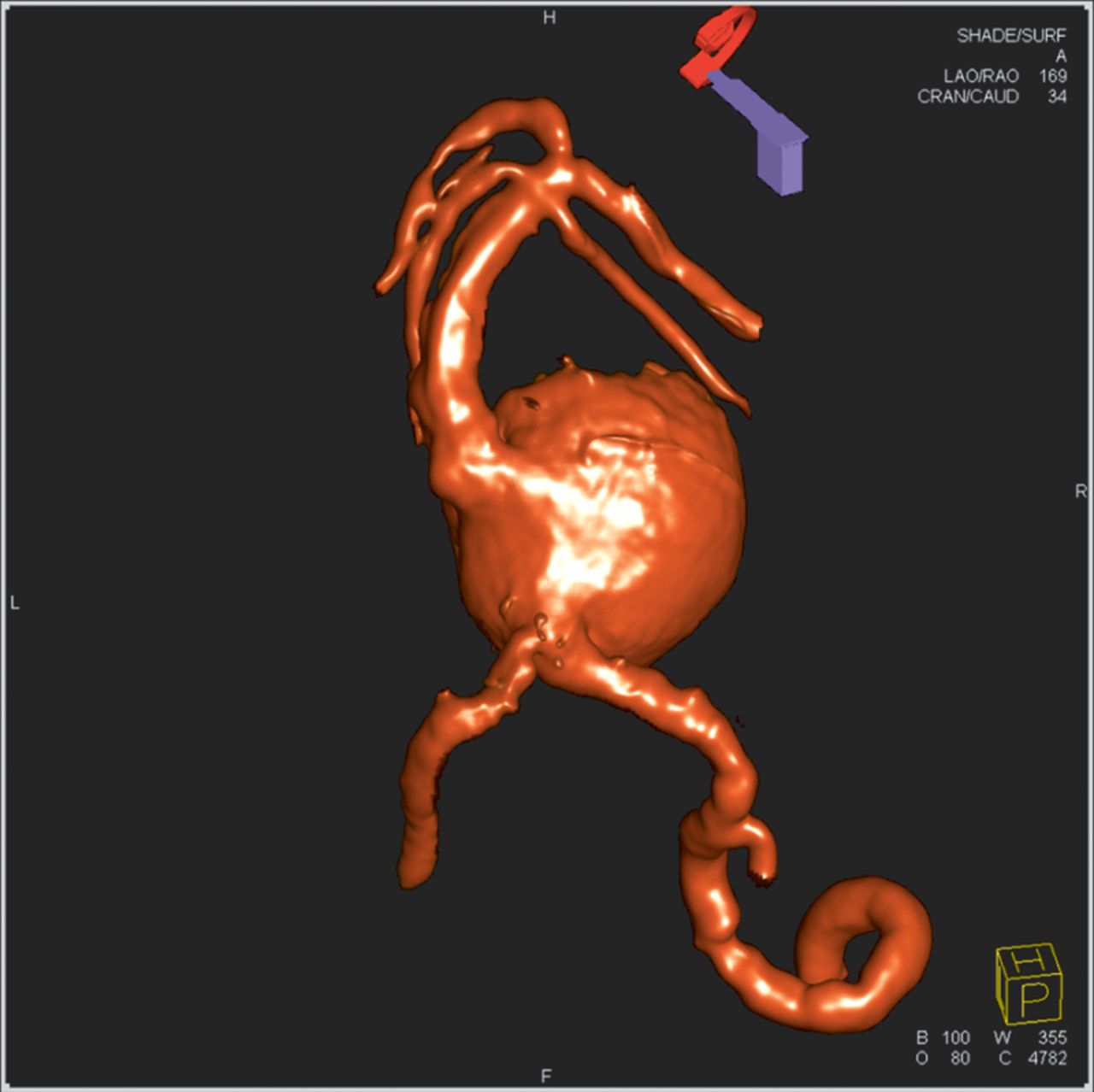
Three-dimensional reconstructed rotational angiogram demonstrating a 2.7 cm×2.7 cm×2.5 cm vertebrobasilar aneurysm.
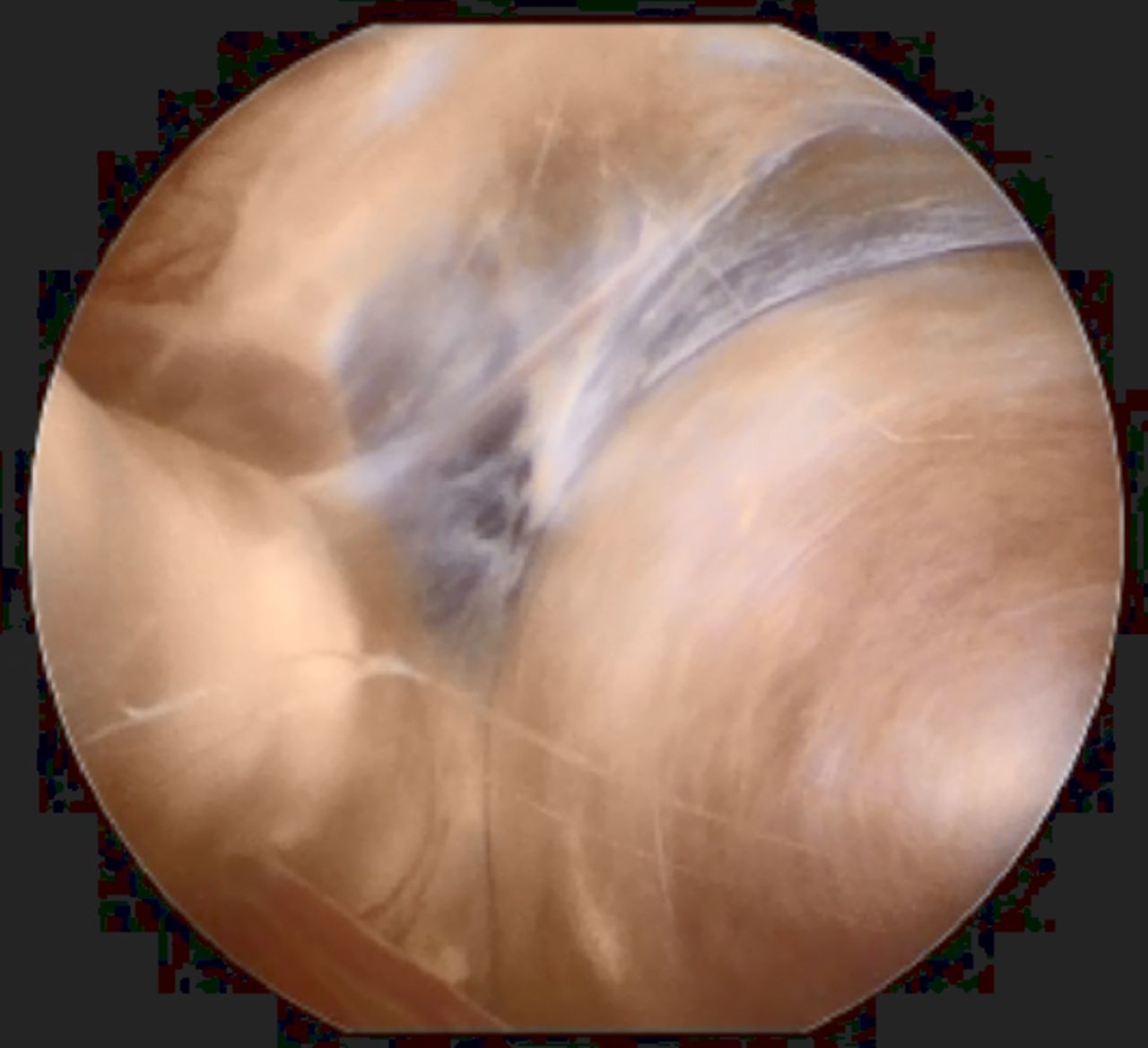
Endoscopic view of the vertebrobasilar aneurysm in the prepontine cistern following endoscopic third ventriculostomy for treatment of obstructive hydrocephalus.

Dilute contrast dynaCT reconstructed image following Pipeline Embolization Device placement for treatment of giant vertebrobasilar aneurysm and coil occlusion of the contralateral distal vertebral artery.
Outcome and follow-up
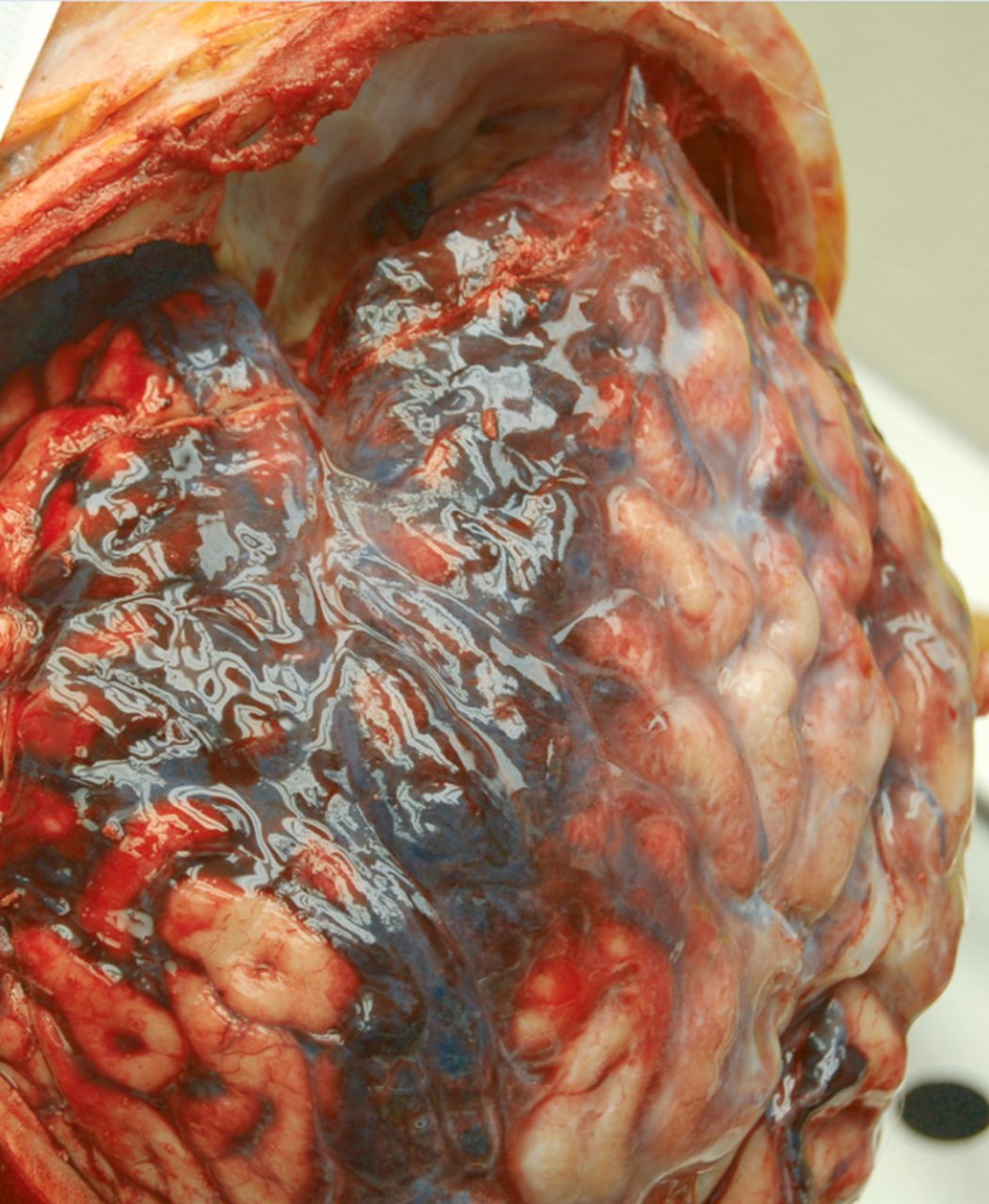
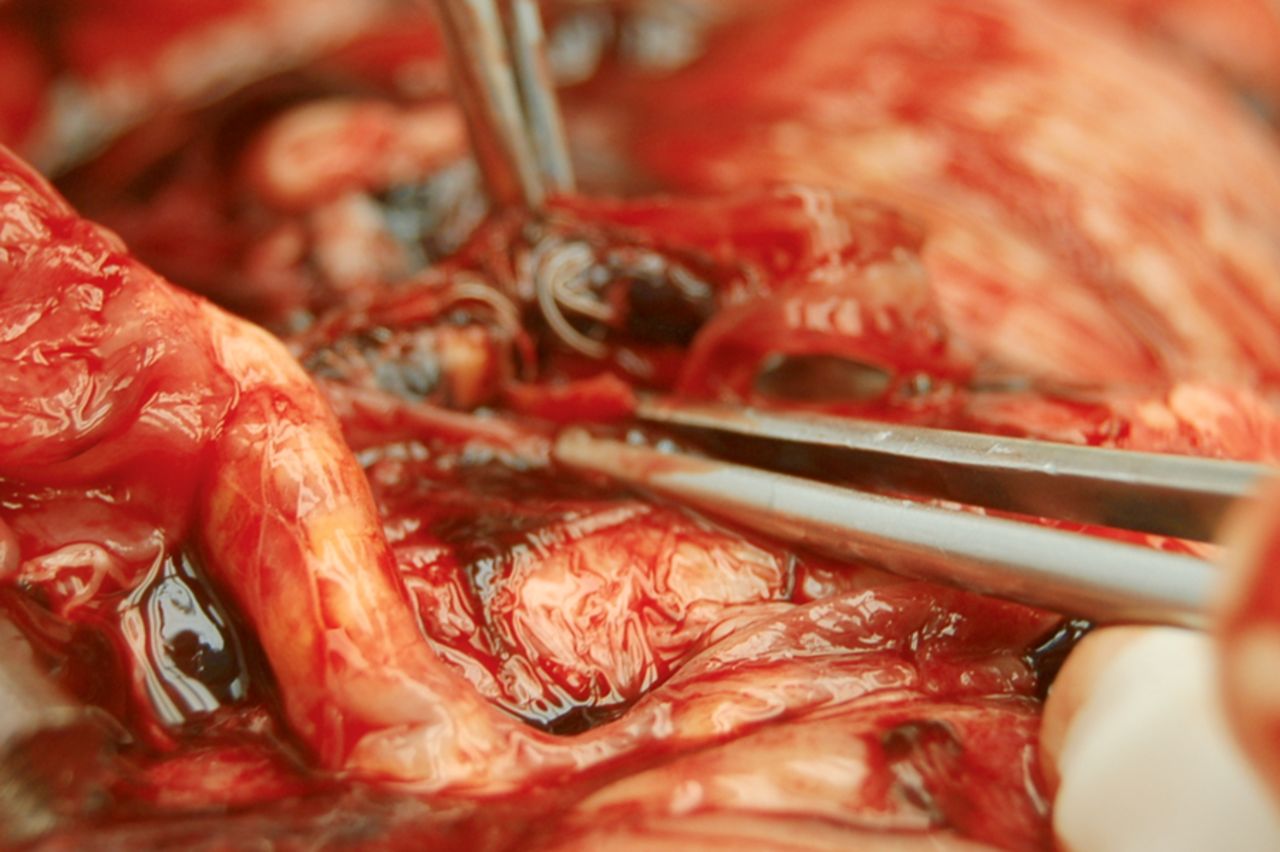
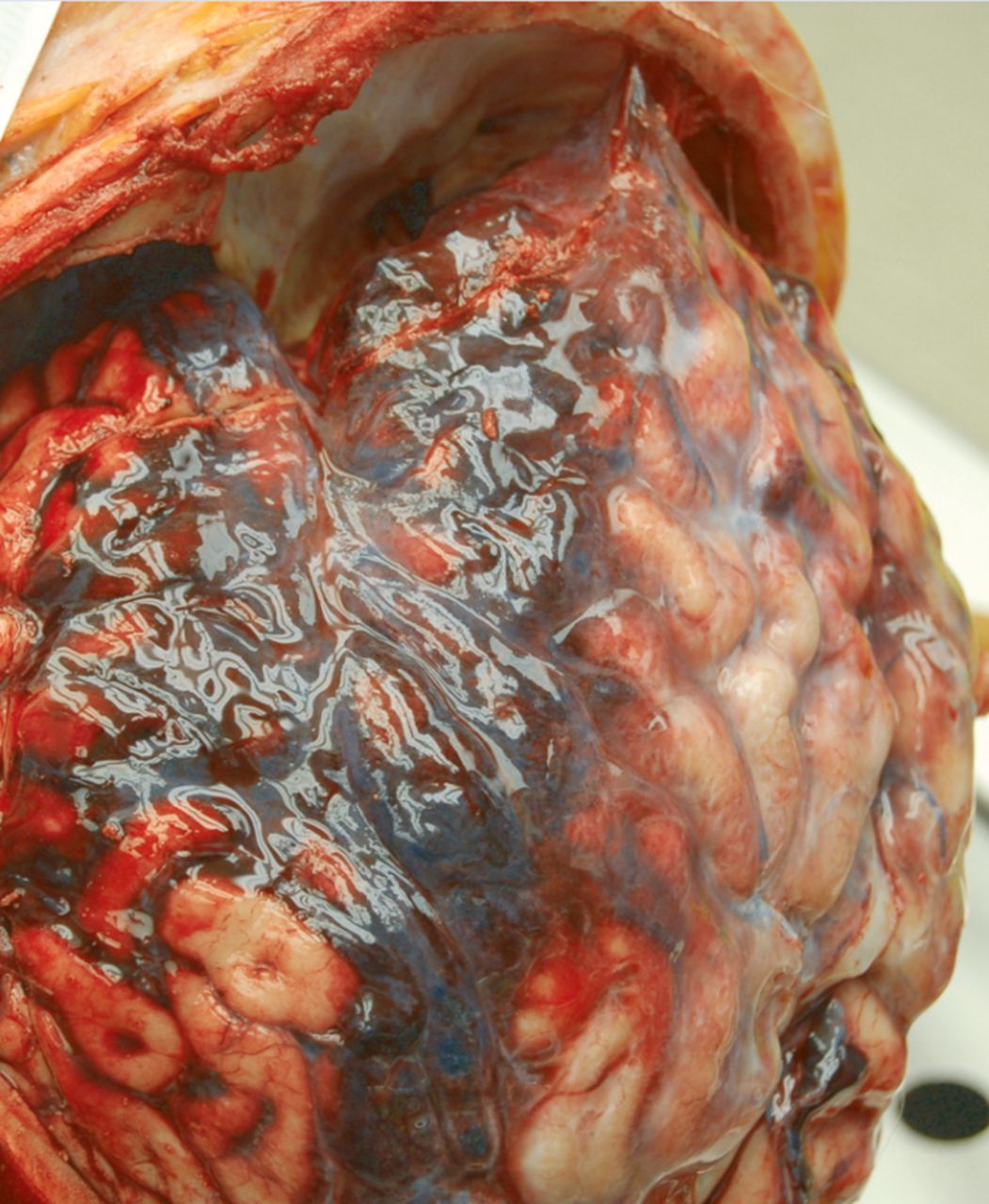
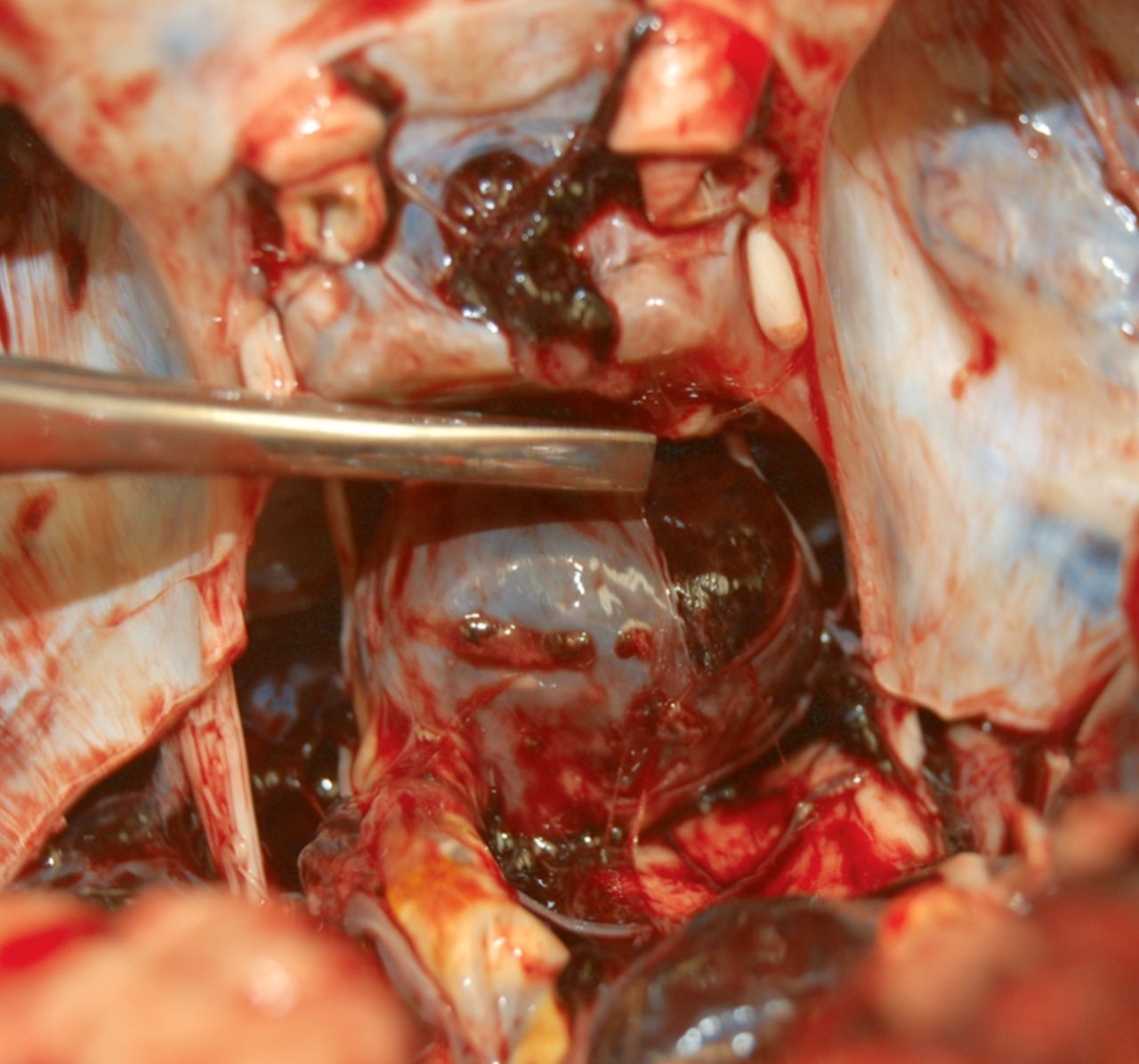
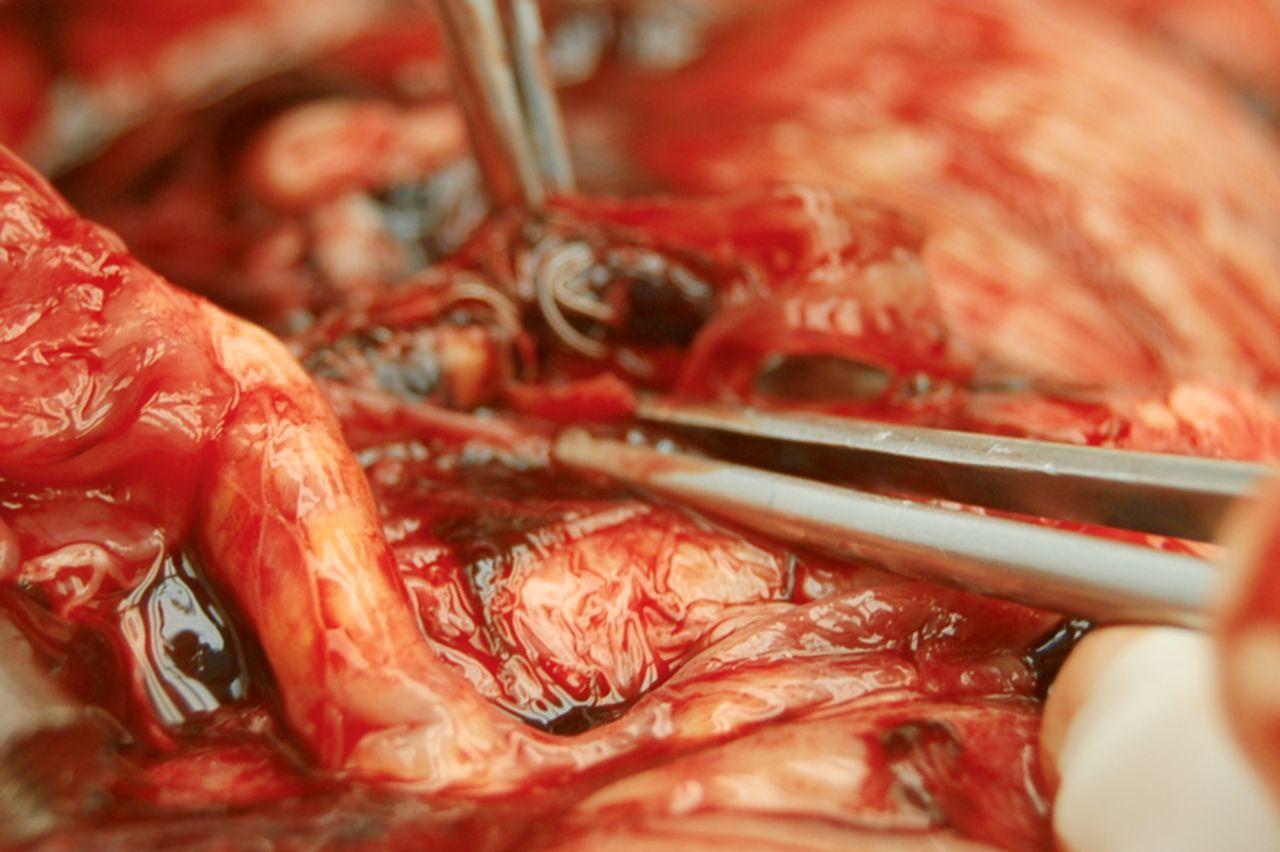
One week after endovascular treatment the patient died suddenly. From the time of his procedure until his death, the patient was maintained on oral steroids and therapeutic dual antiplatelet therapy. Autopsy demonstrated subarachnoid hemorrhage (figure 4) and aneurysm rupture (figure 5). The patent PED was in its intended location (figures 6 and 7), as was the persistent coil occlusion of the distal left vertebral artery (figure 8). The aneurysm was filled with organised thrombus and had ruptured in a linear tear (figure 5).
Autopsy specimen showing extensive subarachnoid hemorrhage in the left sylvian fissure (a subarachnoid hemorrhage in the right sylvian fissure and basal cisterns is not shown).

Autopsy specimen showing aneurysm rupture (linear whole wall rupture) and a thick large expansile clot within the aneurysm.

Autopsy specimen following removal of thrombus/clot showing the Pipeline Embolization Device in place (basilar artery to right vertebral artery).

Pipeline Embolization Device was removed and was patent.
Autopsy specimen showing distal left vertebral artery was occluded as intended.
Discussion
Ruptures following placement of flow diverters for large and giant aneurysms have been previously reported. Chow et al1 reported a case of spontaneous rupture of a posterior inferior cerebellar artery aneurysm following flow diversion treatment. Hampton et al2 also reported a subacute fatal aneurysm rupture 5 days after PED placement. Kan et al3 reported four cases of post-procedural aneurysm rupture. In their series, the basilar trunk artery aneurysms ruptured on postoperative day 1 and approximately 2 months after PED placement. Fischer et al4 reported a large paraclinoid aneurysm that ruptured following PED placement on postoperative day 3.
Subacute or delayed aneurysm rupture following flow diversion therapy is not specific to PED and has also been described following placement of the Silk flow diverter (Balt Extrusion, Montmorency, France).5 ,6 Kulcsar et al5 presented a multicenter European series of patients with 13 cases of aneurysm rupture following Silk placement (10 anterior circulation and 3 basilar artery aneurysms). Most ruptures (10 of 13) took place in the subacute phase (mean 16 days; range 2–48), and three were delayed 3–5 months following treatment.
Multiple theories have been proposed to explain aneurysm rupture following flow diversion therapy. Aneurysm ‘healing’ (or cicatrization) following flow diversion is a dynamic process. After flow diversion there is still some blood flow into the aneurysm. Slowing of this flow results in thrombosis within the aneurysm, which is a necessary part of the cicatrization process.2 ,5
Mural thrombus formation within the aneurysm can result in inflammatory changes in the aneurysm wall and is a known source of protease secretion which can weaken an aneurysm wall.2 ,3 ,5 In abdominal aortic aneurysms, the size of the intra-aneurysmal thrombus correlates with the amount of protease activity. This suggests that a larger thrombus has a larger inflammatory effect.7 So-called ‘mural destabilization’ resulting from this inflammatory interaction is a putative cause of delayed aneurysm rupture.4 If aneurysm wall destabilization occurs before cicatrization, small changes in intra-aneurysmal pressure could potentially result in rupture.2 ,3 ,5
Steroids may aid in reducing the inflammatory response within an aneurysm and adjunctive coil embolization of an aneurysm prior to or at the same time as flow diversion therapy might help to stabilize thrombus formation and reduce aneurysm rupture.2 This use of steroids is unproven.2 Advocacy for the use of coils to ‘stabilize’ an intra-aneurysmal thrombus could be taken from the fact that there were no ruptures in the Pipeline for the Intracranial Treatment of Aneurysms (PITA) trial8 and nearly half of the cases had adjunctive coil embolized; however, adjunctive coiling does not eliminate aneurysm rupture following flow diversion. Kan et al3 reported two cases of ruptured aneurysms following PED treatment with adjunctive coiling and Fischer et al4 also reported a case.
Reports of early ruptures following flow diversion occurring on the same day of treatment and on post-procedure days 1–3 are probably not attributable to an inflammatory or mural destabilization process since this is likely to take days to weeks to occur.3–5 ,9 In contrast, one putative factor that might contribute to early rupture is an enhanced ‘inflow jet’.5
Using computational hemodynamic analysis to evaluate cases of ruptured aneurysms, Cebral et al9 determined that flow diversion can also cause an increase in resistance across the flow diverter device due to autoregulation maintenance of flow downstream. Aneurysms that encompass a large portion of the parent artery are more likely to result in this.9
Hampton et al2 postulated that jailing branch vessels may contribute to aneurysm rupture following flow diversion therapy. In our patient the autopsy demonstrated that there were no significant perforating arteries included within the construct (figure 6).
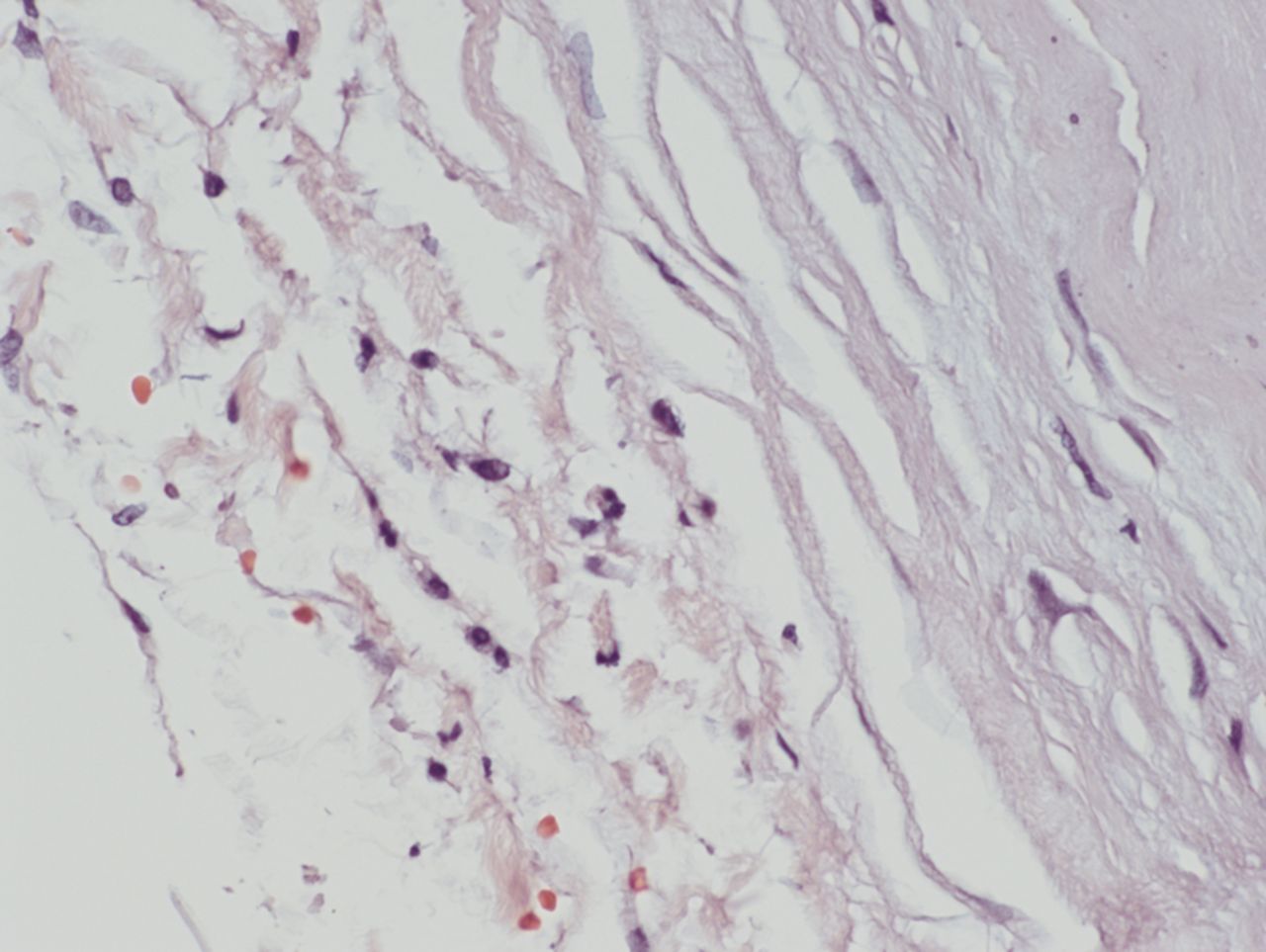
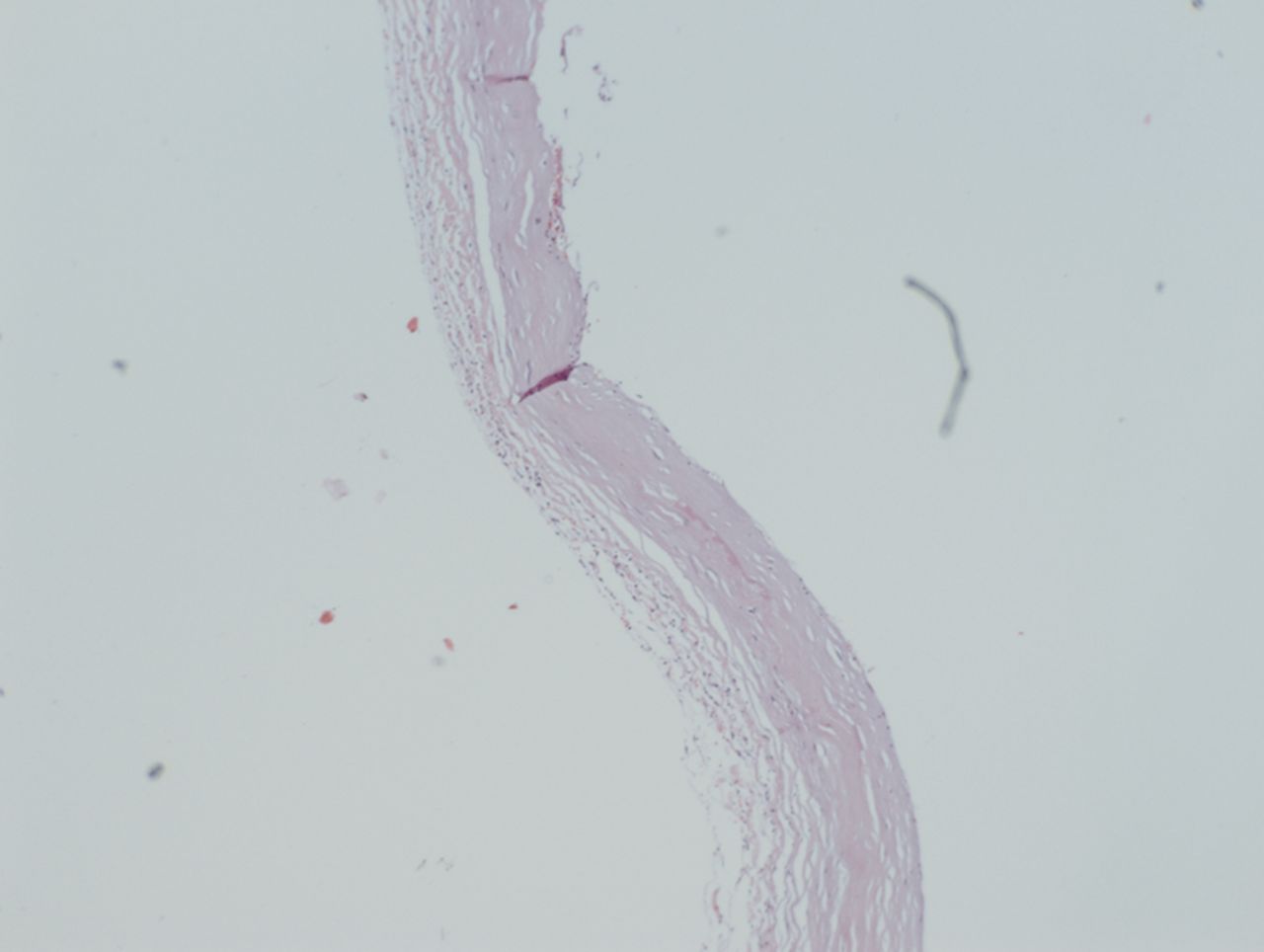
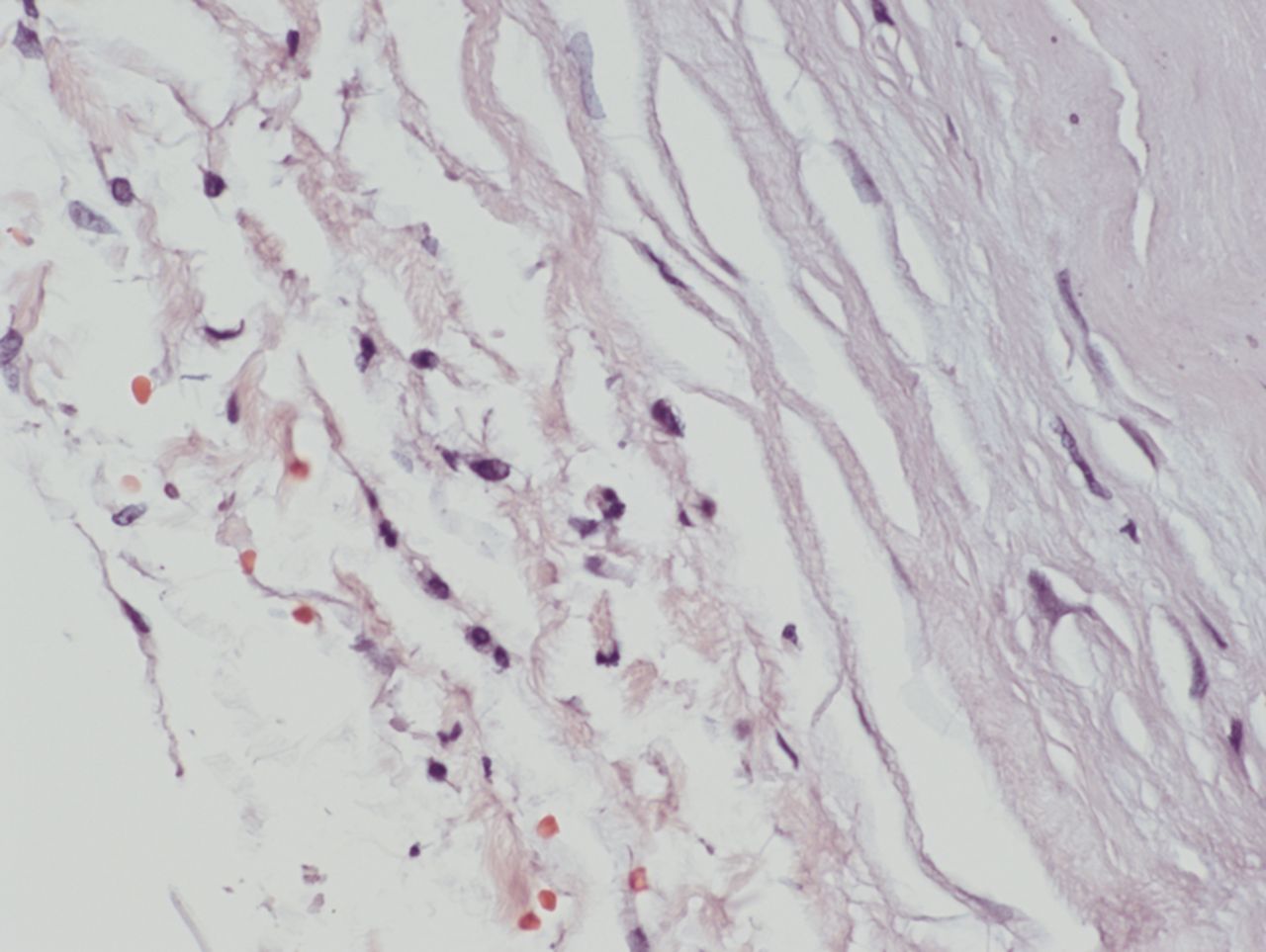
It is interesting to compare the preoperative and endoscopic images of the aneurysm in our patient with the location of rupture of the aneurysm (figures 2 and 5). The site of aneurysm rupture was directly opposite the PED and parent vessel (figure 5). On endoscopic view, the ‘Murphey's teat’ or pointed peak of the aneurysm is clearly seen, pointing superiorly. On autopsy, the rupture site had a linear appearance as if the thrombus outgrew the aneurysm and split the aneurysm wall. Histopathological examination showed that the wall of the aneurysm was extremely thin and microfissures were seen (figure 9). However, no inflammatory cells were seen within the wall and adjacent thrombus (figure 10).

Histological specimen of aneurysm wall showing thinned wall with microfissures.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Magnified histological specimen of aneurysm wall showing thinned wall with no evidence of inflammatory cells.
The cause of aneurysm rupture following flow diversion is probably multifactorial. Histopathological evaluation of our patient's aneurysm wall at the site of rupture revealed no significant inflammatory response. While there was some contrast filling of the aneurysm following PED placement, there was no angiographic high inflow jet. There was no evidence of a treatment-associated complication (eg, wire perforation or new dissection) to explain the aneurysm rupture. The pattern of aneurysm rupture in our patient supports the idea that flow diversion can result in aneurysm rupture through mechanical stretching.
Key messages
Flow diversion of large and giant intracranial aneurysms has been associated with subacute and delayed aneurysm rupture in both the anterior and posterior circulation.
The anatomical and histopathological specimens from this case support a potential mechanical aetiology for aneurysm rupture.
Future studies should evaluate the role (mechanical stress) that flow diversion exerts on an aneurysm wall in the hope that we may compensate for this in some way and thereby avoid post-treatment ruptures.
Acknowledgments
The authors wish to thank Andrew J Gienapp for assistance with technical and copy editing and preparation of the manuscript and figures for publishing.
Footnotes
Republished with permission from BMJ Case Reports Published 29 October 2014; doi:10.1136/bcr-2014-011325
Competing interests ASA served as a consultant for Covidien, Johnson and Johnson, Siemens, Stryker, and Terumo and received grants from Siemens and Terumo outside the submitted work.
Patient consent None.
Provenance and peer review Not commissioned; externally peer reviewed.