Article Text

Abstract
Purpose We present the preliminary angiographic and clinical results of the combined utilization of an AXS Catalyst 5 (Cat5) distal access catheter and a Surpass flow diverter (SFD) for the endovascular treatment of intracranial aneurysms.
Materials and methods Interventional neuroradiology case records were evaluated retrospectively to identify patients treated with an SFD in combination with Cat5. Demographic data, technical success, location of the catheter tip, aneurysm occlusion rate, and procedure-related morbidity and mortality were noted.
Results The analysis yielded 24 patients with 25 aneurysms with a mean age of 52.3±19.7 years. The mean aneurysm diameter was 15.7±8.8 mm. Twenty-one were anterior circulation (seven supraclinoid, one middle cerebral, one anterior choroidal and 12 petrocavernous) and four were posterior circulation (three basilar tip, one posterior inferior cerebellar) aneurysms. Only two of these aneurysms were re-treatments for recurrences. For SFD deployment, the distal tip of Cat5 was placed intradurally and at, or distal to, M1 segment in 88% and 48% of patients, respectively. Aneurysms were bypassed with Cat5 in 80% of the procedures. In one patient, flow diversion was abandoned totally due to arterial tortuosity. With the exclusion of this patient, the technical success rate was 91.7%. There was no permanent procedure-related morbidity or mortality. Of the 22 aneurysms treated successfully with the Surpass device, 20 had imaging follow-up at 6.3±3.8 months and 95% were totally occluded.
Conclusion The Cat5 catheter, which was manufactured for the navigation of large-bore stent-like devices, is a useful adjunct to the Surpass device and allowed us to deploy the device safely.
- catheter
- aneurysm
- artery
Statistics from Altmetric.com
Introduction
Endovascular treatment (EVT) of intracranial aneurysms with flow diverters very frequently necessitates durable and stable coaxial or triaxial catheter systems that include a combination of a guiding sheath and an intermediate catheter (INC).1 The ideal INC must be flexible and safe enough to navigate distal intracranial vasculature, minimizing the risks of perforation and dissection. Consequent to the continuous development of catheter technology, new 5 Fr or 6 Fr intermediate catheters have been introduced, which can be safely navigated within intracranial arterial segments and even distal to the circle of Willis.2 3 These catheters have enabled the utilization of flow diverters, which have a lower pore density and can be deployed through 3F (inner diameter of 0.027 inches) microcatheters.4 The Surpass flow diverter (SFD, Stryker, Neurovascular, Fremont, CA) is a newer flow diverter that was manufactured to achieve higher pore density when deployed across a wide range of arterial diameters.5 The wire size of the Surpass device is similar to the Pipeline device (Medtronic Neurovascular, Irvine, CA) and is about 30 microns6 but the number of wires are higher (48 to 96, whereas in the Pipeline it is 48) to keep the pore density at 20 to 32 pores per millimeter square as compared with 8 to 28 in the Pipeline device. The high pore density allows for a higher aneurysm occlusion rate,7 but the tradeoff for better efficacy is the larger profile of the delivery system.8 The delivery catheter profile for the Surpass is 3.7 inches, so it is harder to navigate intracranially with respect to the Pipeline device which is deployed through the Marksman catheter (Medtronic, Dublin, Ireland) that has a maximum outer diameter of 3.2 inches. AXS Catalyst 5 (Cat5; Stryker, Freemont, CA, USA) was developed specifically for SFD, and it is recommended that the aneurysm is bypassed with the INC to ensure a high technical success rate of SFD deployment. Here, we present the preliminary results regarding the technique of distal navigation of this intermediate catheter.
Materials and methods
A retrospective analysis of our patient records identified patients with intracranial aneurysms who were treated by the combined utilization of the Cat5 and the Surpass flow diverter. Aneurysm size and morphology, patient characteristics, procedure-related morbidity/mortality, location of the catheter tip, and outcomes at follow-up were retrospectively evaluated from patient records. Written informed consent was obtained from all patients and the Institutional Review Board (IRB) approved the study. One tablet (75 mg) of clopidogrel and 300 mg aspirin were administered to all patients except one, who was treated emergently, 5 to 10 days before the endovascular procedure. On the day of the procedure, point-of-care platelet function testing was performed before the procedure in these patients and the treatment was performed if PRU (P2Y12 reaction unit) levels were below 200. Dual antiplatelet therapy was discontinued after the 6-month DSA follow-up and patients were maintained on a life-long aspirin regimen. All procedures were performed via a standard transfemoral approach under general anesthesia. Patients were heparinized with an intravenous bolus of 100 U heparin/kg and activated clotting time was maintained at 2 to 2.5 times the baseline value. A 6-Fr guiding sheath and a Cat5 were used coaxially and the target artery was catheterized. Cat 5 with a 132 cm length was not available in our country and therefore, only Cat 5 with a length of 115 cm was utilized in all cases in this series. Six-Fr 80 cm-long sheaths (Neuron 88, Penumbra, Alameda, CA) were used for all of the procedures except in a procedure performed through a left vertebral approach (a 6F, 65 cm by Destination, Terumo, Tokyo, Japan was used) and in two other procedures in which 6F, 90 cm sheaths were used to provide more support against the tortuous arch. In one of the latter cases, the 6F sheath had to be placed within a shorter, 70 cm 8F sheath (Flexor, Cook Medical, Bloomington, IN) due to tortuosity. The Cat5 was then advanced over a 2.7 to 3.3F microcatheter with the help of a microguidewire and the aneurysm was bypassed with it. These microcatheters included Neuroslider 27 (Acandis, Pforzheim, Germany), Neuroslider 21 (Acandis, Pforzheim, Germany), Renegade Hi-Flo (Boston Scientific Corporation, Natick, MA), Vasco 21 (Balt, Montmorency, France), Vasco 25 (Balt, Montmorency, France), Vasco 28 (Balt, Montmorency, France), and Excelsior XT 27 (Stryker Neurovascular, Fremont, CA). Once the tip of the Cat5 was at the desired location intracranially, the microcatheter and microguidewire were removed. The Surpass delivery system was directly navigated within the Cat5 across the neck of the aneurysm. The catheter was pulled back proximally and the flow diverter was deployed with a gentle forward push on the inner delivery catheter (online supplementary figure 1). During deployment, we tried to obtain wall apposition by unsheating the device while applying gentle steady forward pressure on the delivery catheter. Since the delivery system moves quite easily over the 0.014 inch microguidewire and there is no distally moving ‘delivery wire’ – a property unique to Surpass – this can be done confidently. In case of severe arterial tortuosity, we advanced the inner catheter so that the tip of the flow diverter was just at the tip of the outer catheter. We then pulled the Cat 5 slightly to uncover the tip of the delivery catheter and started to deploy the device. Once the device contacted the arterial wall circumferentially, we pulled Cat5 further back and completed the deployment. This was done to minimize the friction between the innermost catheter and the delivery catheter. After device deployment, if there was any suspicion about the wall apposition in the middle or proximal segments of the flow diverter, we re-accessed the flow diverter over the coaxial system, first with the outer catheter and then Cat5. This was performed to enhance wall apposition and to preclude the need for a wire exchange procedure in case we also decided to perform angioplasty within the device (which was eventually performed in one-third of the cases). If there was only distal malapposition at the distal tip of the device so that the flow diverter remains unapposed in the innermost aspect of an arterial curve, we directly proceeded with stenting to eliminate the risk of fishmouthing by ‘pinning’ the distal end with the stent. Again, this was performed through the delivery system that is already in place and an exchange maneuver was not needed. Since we believe that wall apposition is one of the most critical factors in minimizing the thromboembolic complications and maximizing the efficiency of flow diversion, we are not reluctant in taking additional steps to improve apposition, which we thoroughly check at the end of the procedure with a flat panel CT with and without intraarterial injection of the diluted contrast medium. Following the implantation of the Surpass device, angiograms were obtained to assess the flow stagnation within the aneurysms and to check the ipsilateral intracranial circulation. Adjunct devices such as intracranial balloons or stents or coils were utilized through Cat5 or the aneurysm was coiled through a jailed microcatheter via a second access catheter as deemed necessary by the operator. All patients were called back for clinical and imaging follow-up with CT angiography (CTA) or magnetic resonance angiography (MRA) 6 to 12 weeks after the procedure, for a cerebral DSA evaluation 6 months after the procedure and for noninvasive angiographic imaging 1 year after the procedure.
Supplementary file 2
Results
There were 24 patients (16 females and eight males) with a mean age of 52.3±19.7 years (range 16 to 84 years) with 24 unruptured aneurysms and one acutely presenting iatrogenic internal carotid artery pseudo-aneurysm. The mean aneurysm diameter was 15.7±8.8 mm (range 2.5 to 32 mm). There were four and 21 aneurysms located on the posterior and anterior circulations, respectively – patient demographics and aneurysm characteristics are shown in online supplementary table 1. We were able to deploy the Surpass device in 22 of the 25 aneurysms, yielding a success rate of 88%. When a patient with an abandoned flow diversion procedure is excluded (described below), the technical success rate was 91.7%. In 23 patients, a single device was used, in one patient, the first flow diverter foreshortened more than we expected and a second device had to be used to be able to cover the whole length of the fusiform aneurysm. The distal tip of the Cat5 was placed intradurally (at or beyond the ophthalmic artery origin) in 88% of patients and at, or distal to, M1 segment in 48% of patients. Figure 1 and online supplementary figure 2 show two examples that demonstrate the navigability of Cat5 in tortuous arterial anatomy. The most commonly utilized microcatheters for Cat5 navigation were Vasco 28 and Neuroslider 27 (six cases each). These were followed by Renegade Hi-Flo (four cases), Vasco 21 (three cases), Excelsior XT 27 (two cases), Neuroslider 21, and Vasco 25 (one case each) microcatheters. In two cases Cat5 was directly navigated over the 0.035 inch glidewire. In two other cases, we were not successful in reaching the target arterial segment with the first microcatheter. Consequently, one Vasco 28 had to be replaced with an Excelsior XT 27 and one Renegade Hi-Flo catheter had to be replaced by a Rebar 27 (Covidien, Irvine, CA) both of which navigated successfully. The aneurysms were bypassed with Cat5 in 80% (20 of 25) of aneurysms and Cat5 could be placed at the level of the aneurysm neck (‘across the neck’) in one aneurysm (4%). In one of the four patients in whom the aneurysm was not bypassed, flow diversion was abandoned, whereas in two other basilar tip aneurysms, the vascular anatomy was straight beyond the V4 segment and there was no need to navigate Cat5 distally. In the last of these four patients (a patient who presented acutely with an iatrogenic ICA blowout), bypass of the arterial wall defect was deemed to be too risky with Cat5 and a bypass was not attempted. In the case with aborted flow diversion, it was not possible to navigate the Cat5 across the neck of the giant, partially clotted basilar tip aneurysm. Neither the Surpass device nor a Headway 27 (MicroVention, Tustin, CA) or Vasco 21 (Balt, Montmorency, France) or Prowler Select Plus (Codman & Shurtleff, Inc., Raynham, MA) microcatheter was able to bypass the aneurysm. Finally, we were able to navigate an SL-10 microcatheter (Boston Scientific Corporation, Natick, MA) distal to the aneurysm, an Atlas stent (Stryker, Fremont, CA) and a Leo baby stent (Balt, Montmorency, France) were deployed telescopically and the aneurysm was coiled with stent assistance (online supplementary figure 3). In the second patient with technical failure (patient with an MCA aneurysm), we were able to reach the aneurysm with the Cat5, but its distal tip repeatedly got caught at the junction of the aneurysm and the efferent artery. We were not able to navigate the Surpass device directly across the aneurysm neck since it also got stuck at the same point. A Derivo embolization device (Acandis GmbH & Co. KG, Pforzheim, Germany) was utilized for flow diversion. The images of this patient are provided as online supplementary figure 2. In the third patient with a technical failure, there was a recanalized supraclinoid ICA aneurysm, which we were able to bypass with Cat5: however, as the Surpass device was pushed distally, the INC kicked back and distal access was lost. This patient was then treated by placement of a scaffolding Leo stent (Balt Extrusion, Montmorency, France) and deployment of a Silk (Balt Extrusion, Montmorency, France) device within the stent. Aside from the a tiny dissection as noted in figure 1, we did not observe angiographic signs of endothelial injury such as dissections, occlusions, or vasospasm secondary to the navigation of Cat5. The mean follow-up duration for aneurysms successfully treated with the Surpass device was 6.3±3.8 months (range 10 days to 13 months). The last modality that was used at follow-up was CTA for two aneurysms, MRA for two aneurysms, and DSA for 16 aneurysms. Seventeen out of these 22 aneurysms had a DSA during follow-up: in three cases a 6-month DSA is pending, in one case DSA is deferred due to pregnancy, and in one case a 84-year-old patient preferred to be followed by CTA. Aneurysm characteristics, patient demographics, position of the Cat5, and outcomes at follow-up are summarized in online supplementary table 1. For this group, the occlusion rate at follow-up was 95% (19/20 of the aneurysms treated with flow diversion using the Surpass device that underwent imaging follow-up).There was no procedure-related permanent morbidity or mortality in this series. Technical complications occurred in two patients. In the patient with the MCA aneurysm who was treated with another flow diverter as described above, a focal subarachnoid hemorrhage localized in the distal Sylvain fissure was noted incidentally on the routine flat-detector CT obtained at the end of the procedure. The patient awakened from general anesthesia at baseline neurologic state without any significant symptoms and was managed conservatively. The second technical complication was a small intimal flap of the proximal internal carotid artery, which we noticed during embolization in a patient with a giant cavernous aneurysm and significant proximal arterial tortuosity. The procedure was continued and finished as intended. A Leo stent was deployed at the site of the injury on the way out of the carotid artery at the end of the procedure. During clinical follow-up, there were two significant events. The patient treated for an exsanguinating iatrogenic internal carotid aneurysm expired later, secondary to diffuse carcinomatous involvement of the skull base. The pseudoaneurysm had developed during the transsphenoidal resection of this lesion. A 16-year-old girl with a supra-clinoid ICA aneurysm, which was occluded at the fifth month angiogram, had a transient scotoma ipsilateral to the Surpass device, which had been deployed across the ophthalmic artery. The symptoms resolved spontaneously within minutes. As for the imaging follow-up, fishmouthing and significant parent artery stenosis were detected at the 1-year follow-up angiogram in a patient with a supraclinoid ICA aneurysm, but the aneurysm was occluded and the patient did not report having a stroke during this time. Otherwise, there were no significant imaging findings in the remaining patients.
Supplementary file 1
Supplementary file 3
Supplementary file 4

{kind=link}
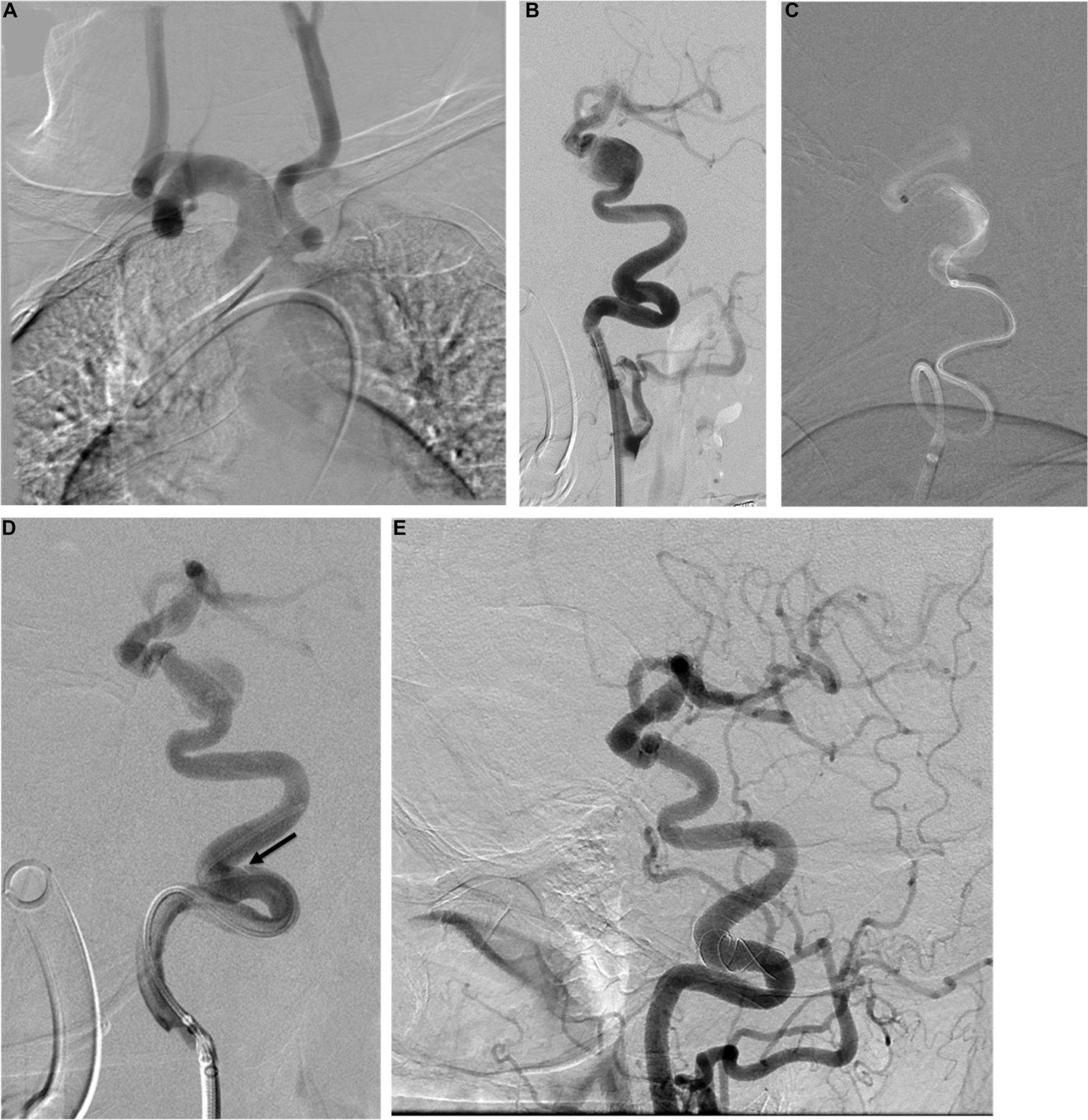
(A)Tortuosity of the supraaortic arteries on left oblique projection and (B) left internal carotid artery in lateral projection in a patient with partially clotted giant cavernous aneurysm. (C) The Cat5 catheter was used to bypass the aneurysm. (D) Postprocedure angiogram shows a small intimal flap (arrow). This was treated by placement of a Leo stent. (E) Follow-up angiogram reveals no evidence of residual aneurysm filling or restenosis.
Discussion
INCs are critical components of the triaxial systems commonly used in the EVT of cerebral aneurysms. They are also invaluable for the treatment of acute ischemic stroke. Ideally, an INC should be very flexible and navigable while providing maximum support for catheters or stent-like devices. However, INCs used for acute stroke treatment and embolization tend to be on either side of the spectrum, i.e., those used for stroke tend to be more flexible and those used for embolization are designed to be sturdier. Nevertheless, INCs manufactured for support have been utilized for acute stroke treatment based on their ability to provide very distal access.9 A new generation of INC, the AXS Cat5, has been developed to provide maximal support while maintaining the ability to provide very distal access.4 The Cat5 was specifically manufactured to enable intracranial navigation of the Surpass device. This catheter is less flexible but sturdier than the AXS Catalyst6 INC that was produced by the same vendor for stroke treatment only. Its outer surface is made of nylon and has hydrophilic coating, while the inner surface is made of polytetrafluoroethylene (PTFE). The shaft consists of a nitinol and polymer fiber. It is a 115-cm or 132-cm catheter with variable stiffness that is distributed over 12 zones along the working length. Although this catheter was specifically produced as an adjunct to the Surpass device, the only report on this guiding catheter relates to its use with the smaller caliber Pipeline device (PED; Medtronic, Minneapolis, MN).4 The inner diameter of Cat5 is 0.058 inches.4 The proximal outer diameter of 5.6 Fr (1.86 mm) and distal outer diameter of 5.3 Fr (1.76 mm) allows for contrast material injection through a 6 Fr guiding sheath. The Surpass flow diverter stent, a relatively new flow diverter with high mesh density, is difficult to deliver via standard INCs because of the stiffness of the approximately 4 F delivery catheter. With the combined utilization of the Cat5 and the Surpass, the delivery of this flow diverter was possible in 92% of patients treatable by flow diverters in this series (22 out of 24 patients, in one patient flow diverter placement was not possible). This is similar to the 95% technical success rate obtained by Colby et al using the Navien INC (Covidien Vascular Therapies, Mansfield, MA) and the Pipeline flow diverter.2 Notably, the technical success rate with the combination of the Cat5 and the Pipeline device by the same authors was 100%, suggesting better navigability and/or support by this catheter.4 The major difference between the series reported by Colby et al and the current series is the way the Cat5 was utilized. Colby et al used the INC in the traditional way, i.e., leaving it proximal to the aneurysm. We, on the other hand, wanted to make use of the flexibility of the Cat5, therefore, we bypassed the aneurysms with the Cat5 in 80% aneurysms. Consequently, in the present study, the distal tip of the Cat5 was placed intradurally in 88% of patients and at, or distal to, M1 segment in 48% of patients, compared with its placement intradurally in 19% and at, or distal to, M1 segment in 1% of patients treated by Colby et al. Although our technical success rate in the deployment of the Surpass device was lower than in previous studies,5 10 11 this failure rate can be explained by extreme arterial tortuosity in the failed cases, as demonstrated in online supplementary figure 2, 3, and by the fact that flow diversion was not possible at all in one of the three failed cases. Coupled with the fact that we had no permanent morbidity or mortality in our series, compared with morbidity and mortality rates between 3% and 27% in previous publications, this discrepancy may be a result of the fact that we refrained from forcing the Surpass device across the aneurysm neck, thus resulting in a slightly lower success rate while potentially precluding hemorrhagic complications. The mean aneurysm size of approximately 16 mm in our cohort is larger than in previous reports on the Surpass, and by itself is actually a risk for a higher complication rate.12 Our results also compare very favorably with those of Colby et al and hence imply the safety of the Surpass device when combined with intradural placement of the Cat5. The justification of the efforts for the technically demanding navigation of the Surpass device includes the high aneurysm occlusion rates obtained with this high mesh density device, as demonstrated in previous studies.5 10 The higher rate of occlusion in our series possibly result from both the higher mesh density of Surpass and our efforts in maximizing wall apposition of flow diverters. In addition, Surpass deployment was not associated with some of the reported drawbacks of Pipeline placement, namely, a distinct step-off between the delivery microcatheter and INC, the need for advanced maneuvers to deploy the device, or the recapture of a twisted device.4 Absence of any significant foreshortening is another advantage for fusiform or very wide-neck aneurysms.11 Finally INC access distal to the aneurysm for flow diverter deployment (the so-called ‘Shepherd technique’) has been advocated to prevent device torsion and device prolapse into the aneurysm.13 Although we treated wide-neck and fusiform large/giant aneurysms in this series, we did not encounter any device torsion or prolapse because Cat5 enabled easy access distal to the aneurysms and the Surpass device has been more resistant to both of these technical problems in general. There were several limitations in the current study. First, although very distal access is becoming widely utilized in acute ischemic stroke treatment without a major increase in hemorrhagic complications, a larger sample size is necessary to draw firmer conclusions on the wide applicability of such access for flow diversion. Second, our low threshold for switching to another device may have slightly overrated the technical failure rate and underrated the complication rate with this approach. This study also suffers from the drawbacks of its single-center retrospective design, including, but not limited to, the absence of a control group, precluding us from definitely proving the safety of this technique. The recently introduced Offset catheter (AXS Offset Delivery Assist Catheter, Stryker, Fremont, CA) is claimed to enhance the navigation and safety of 5F distal access catheters, specifically the Cat5, distally in the intracranial circulation. Unfortunately this catheter is not available in our country and was not used in this series. Nevertheless, the combined utilization of the Cat5 and the Surpass device had a relatively high safety profile for intracranial aneurysm treatment. Finally, the lack of randomization and lack of a control group were other major limitations.
In conclusion, we have demonstrated that the Cat5 catheter, which was manufactured for the navigation of large-bore stent-like devices, is a useful adjunct to the Surpass device and allowed us to deploy the device safely.
References
Footnotes
Contributors All of the authors made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; and final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Hacettepe University Ethical Committee.
Provenance and peer review Not commissioned; externally peer reviewed.