Article Text

Abstract
Introduction Flow diverters (FDs) are increasingly used in the treatment of wide-necked aneurysms.
Objective To examine the hypothesis that intentional FD compaction might improve aneurysm occlusion rates.
Methods Bilateral wide-necked carotid aneurysms were created in 12 dogs. Endovascular treatment was performed 1 month later, using Pipeline embolization devices deployed with compaction across the aneurysm neck (n=12). Group 1a consisted of aneurysms treated with a single compacted FD (n=8), while group 1b aneurysms required two compacted FDs (n=4). Control aneurysms were treated with a single non-compacted FD (group 3; n=6), or not treated (group 4; n=4). Angiographic results were compared at 3 months. Pathology specimens were photographed and the neointimal coverage of devices scored using an ordinal grading system.
Results Twenty-two of 24 aneurysms were patent at 1 month. Deployment with compaction was successful in eight cases (group 1a aneurysms). The compaction maneuver led to immediate FD prolapse into the aneurysm in four cases, rescued by deploying a second, telescoping FD (forming group 1b aneurysms). One compacted device later migrated distally, leaving the aneurysm untreated. Angiographic results differed significantly between groups (p=0.0002). At 3 months, aneurysms successfully treated with a single compacted FD were more often occluded at 3 months (7/7) than aneurysms flow-diverted without compaction (2/6; p=0.021). All aneurysms treated with two compacted FDs were occluded, while all untreated aneurysms remained patent. There were no parent vessel stenoses.
Conclusions Compaction of FDs can improve angiographic occlusion of experimental wide-necked aneurysms.
- Aneurysm
- Angiography
- Flow Diverter
Statistics from Altmetric.com
Introduction
Flow diverting devices are increasingly used to treat aneurysms.1 Compared with stents, flow diverters (FDs) have a lower porosity and a higher pore density metallic mesh. FDs aim to redirect flow patterns, to induce aneurysm thrombosis, and to repair the defect in the wall of the parent vessel, by providing an endoluminal scaffold at the level of the aneurysm ostium on which neointima can form.2 Constructs of lower porosity and higher pore density have been shown to improve the efficacy of experimental aneurysm occlusion.3 ,4
Recently, device delivery technique has been shown to affect the amount of metallic coverage, with the potential to improve treatment results.5 Compacting the device over an aneurysm ostium, but ensuring the device is not compacted over branch origins, may improve aneurysm occlusion rates and reduce risks of branch occlusion.6–8 This technique might obviate the need for re-treatment with additional FDs, by obtaining with one device the amount of metallic coverage which would otherwise only be possible with overlapping multiple devices.9
Canine aneurysm models have previously been shown to be challenging tests for flow diversion, particularly when the aneurysms have wide necks.3 ,9 ,10–11 We sought to use an animal model to explore whether we could improve aneurysm occlusion rates by intentionally compacting FDs during deployment.
Methods
Surgical aneurysm creation
Protocols for animal experimentation were approved by the Institutional Animal Care Committee in accordance with guidelines of the Canadian Council on Animal Care. All procedures were performed in 7–15 kg canines under general anesthesia. Using a modification of the seminal work of German and Black,12 in 12 animals, through a midline vertical cervical incision, the left external jugular vein was harvested, inverted to remove valves, and placed in heparinized saline until vein pouch creation. On each carotid artery, temporary clips were applied, and an arteriotomy created on the lateral aspect of the carotid artery. The harvested external jugular vein was divided in half, a linear venotomy of appropriate size fashioned, and the vein attached to the carotid artery in a side-to side anastomosis using a continuous 7.0 Prolene suture (Ethicon, Cincinnati, Ohio, USA). The ends of the veins were secured, and temporary clips were removed. Any bleeding sites were repaired, and the procedure was then repeated on the contralateral carotid artery. The incision was closed in multiple layers over a separately tunneled drain, which was typically left for 24–48 h.
Endovascular treatment
Endovascular treatment was performed at least 4 weeks after surgical aneurysm construction, through a coaxial microcatheter system introduced by a percutaneous transfemoral approach. Guiding catheters used were Envoy 5F (Cordis Neurovascular, Fremont, California, USA), through which a Marksman microcatheter (Covidien/Medtronic, Minneapolis, Minnesota, USA) was placed. FDs were Pipeline embolization devices (PEDs; gifts from Covidien) 3.5–3.75 mm in diameter, 30–35 mm in length. The size of FD was selected according to the diameter of the proximal landing zone of the recipient vessel (3.5–4 mm in this model). After partial deployment, leaving at least 10 mm of distal landing zone, the FDs were delivered using compaction: the FD was intentionally compacted over the aneurysm ostium by pushing on the delivery wire, keeping forward pressure on the delivery microcatheter (n=12). In five aneurysms, excessive compaction led to prolapse of FDs into the aneurysm fundus. The four cases where this occurred during treatment were salvaged using a second FD, deployed with compaction again, inside the first FD in a telescoping fashion. The fifth case prolapsed distally in a delayed fashion, and could not be salvaged. Aneurysms treated with a single compacted FD constitute group 1a aneurysms (n=8); aneurysms treated with an additional layer of compacted metal coverage constitute group 1b aneurysms (n=4). Control flow-diverted aneurysms were treated without compaction (n=6): by simple unsheathing of the FD, by stabilizing the pusher wire and pulling on the delivery microcatheter, as summarized by Ma et al.7 The amount of FD compaction used during the delivery of FDs was crudely estimated post hoc in animals treated with a single device by a compaction index (measured length of the deployed FD/nominal FD length). Group 4 comprised untreated control aneurysms (n=4). Treatment groups are presented in figure 1. The characteristics of aneurysms, FDs, and treatments are summarized in table 1.
Aneurysm and flow diverter characteristics and treatment outcomes

Schematic representation of treatment of the wide-necked aneurysms. (A) Group 1a: single flow diverter (FD), compacted. (B) Group 1b, double FDs, compacted (rescue maneuver when devices prolapsed acutely). (C) Group 3, single FD, non-compacted. (D) Group 4, untreated controls.
Antiplatelet regimen
Animals were treated with daily acetylsalicylic acid (ASA) 325 mg and clopidogrel 75 mg for 4 days before flow diversion, according to previous experience.13 Clopidogrel therapy was discontinued 10 days after PED implantation, while ASA was continued until sacrifice. Control animals received the same course of antiplatelet drugs.
Angiography
Transfemoral angiography was performed in all animals immediately before and after PED deployment, and immediately before sacrifice. To prevent femoral hematomas on dual antiplatelet therapy, all punctured femoral arteries were surgically exposed through a small linear incision and ligated, a routine procedure that is well-tolerated by the animals. Angiographic results were scored using an ordinal system modified from Kamran et al.14 A score of 0 indicated no change in aneurysm volume with treatment, 1 residual contrast filling more than 50% of the pretreatment aneurysm volume, 2 residual contrast filling <50% of the pretreatment aneurysm volume, 3 residual filling confined to the neck region, and 4 no residual filling (complete occlusion). Aneurysm occlusion rates were further dichotomized into failure (scores of 0, 1, 2) or success (scores of 3, 4). The parent vessels were carefully checked for the presence of stenoses.
Sacrifice, photography, pathology
Euthanasia by barbiturate overdose was performed at 12 weeks. After fixation in 10% formalin, the carotid artery aneurysm construct was opened longitudinally and photographed using a computerized imaging system (Vision PE, Clemex Technologies, Montreal, Canada).
The degree of neointimal coverage of the device(s) was scored independently by two observers according to a semiquantitative scale using centiles of neointimal coverage, from 0% to 100% (in 10% increments), conceived as the ratio of the FD surface covered with mature neointimal tissue and divided by the total area, as described by Darsaut et al.11 ,13 In cases of disagreement, a final score was decided in a consensus session.
Fixed selected aneurysms, together with a biopsied samples of the tissue covering the free segment of the FD overlying the aneurysm ostium, were stained with hematoxylin phloxine saffron and Movat's pentachrome and studied under the microscope, to look for the presence of neointimal tissue covering the device, and for the presence of organized thrombus inside the sac of aneurysms.
Statistics
We did not perform a formal sample size calculation according to a predetermined hypothesis, but we estimated from previous work that 12 animals (24 aneurysms) would enable us to explore the technique of compaction and show a large difference between pertinent groups (compacted vs non-compacted), reserving four aneurysms as untreated controls, and six as controls treated with flow diversion without compaction. Aneurysms dimensions were compared between groups using t tests. Mann–Whitney U tests for ordinal data were used to compare the compaction index and the neointimal scores of the groups treated with a single FD. The Freeman–Halton extension of the Fisher exact probability test was used to compare angiographic results between the four groups, followed by a single 2×2 comparison between the two groups of interest (aneurysms treated with a single compacted (group 1) or non-compacted FD (group 3). The threshold for significance was set at p=0.05.
Results
At angiography, 2/24 (8%) surgically created aneurysms were occluded before treatment. These aneurysms were excluded from subsequent analyses. Aneurysm dimensions are presented in table 1. There were no significant differences in aneurysm dimensions between the groups.
Deploying FDs with a compaction maneuver was trickier than we initially expected. The main difficulties in this relatively straight model were related to device shortening with compaction, and the resulting unpredictability of the location of the proximal landing zone. The wide necks of experimental aneurysms could be satisfactorily covered in seven cases, but compaction of the device was excessive and resulted in prolapse of the FD into the aneurysm in four cases. A second telescoping device was used in these four cases, deployed once more with compaction. Another aneurysm, treated with a compacted FD, was found at follow-up angiography to no longer be covered with the device at all; the FD had migrated distally to the maxillary artery.
By comparison, unsheathing of the device without compaction permitted complete coverage of the aneurysm ostium with a single FD without complication in all cases. The extent of device compaction during deployment, calculated using a compaction index (nominal FD length/measured length of deployed device), was significantly different between groups 1a and 3; (p<0.05, Mann–Whitney U test).
Angiographic results
Angiographic results differed significantly between groups (p=0.0002). Group 1a aneurysms treated with a single, compacted FD, were more likely to be occluded at 3 months (7/7 aneurysms), than group 3 aneurysms (2/6; p=0.021). Representative cases comparing angiographic results of compacted and non-compacted FDs are shown in figure 2. All four group 1b aneurysms treated with two compacted FDs were occluded by 3 months, while all four untreated group 4 aneurysms remained widely patent. No parent vessel stenosis was noted within any arteries treated with one or two FDs.

(A) Group 3 aneurysm before treatment (A1) with single non-compacted flow diverter (FD) (A2), showing a large residual aneurysm at 3 months (A3). (B) Group 1a aneurysm before treatment (B1) with a single FD compacted at (*)(B2), leading to complete aneurysm occlusion at 3 months (B3). Note that the same size FD was used in both cases (3.5×35 mm).
Macroscopic photography
There was a significant difference in the neointimal scores between groups (p=0.039). Compacted single FDs were covered with thick neointima, with three cases showing complete closure of the aneurysm ostium (figure 3C). The other four cases showed almost complete neointimal coverage.
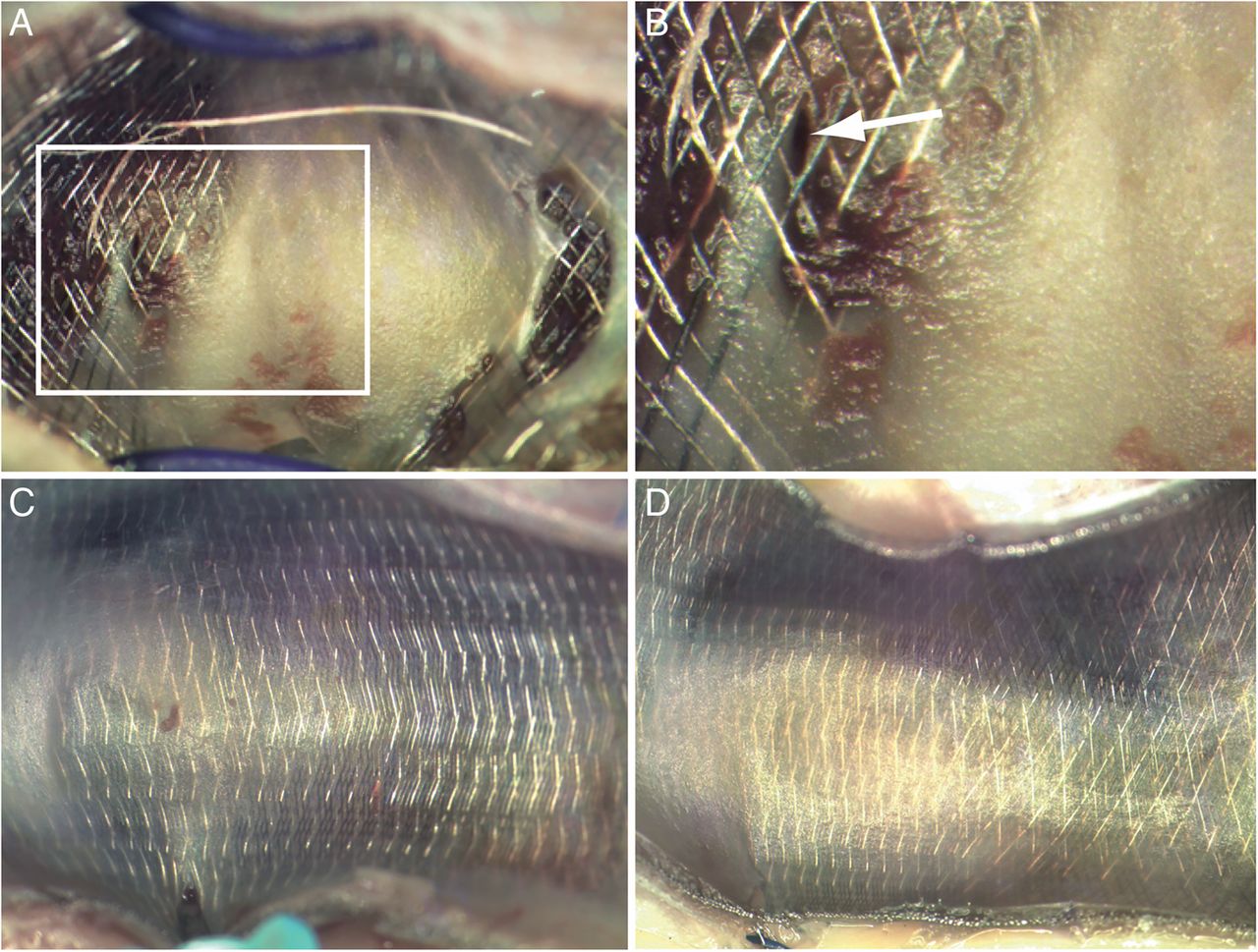
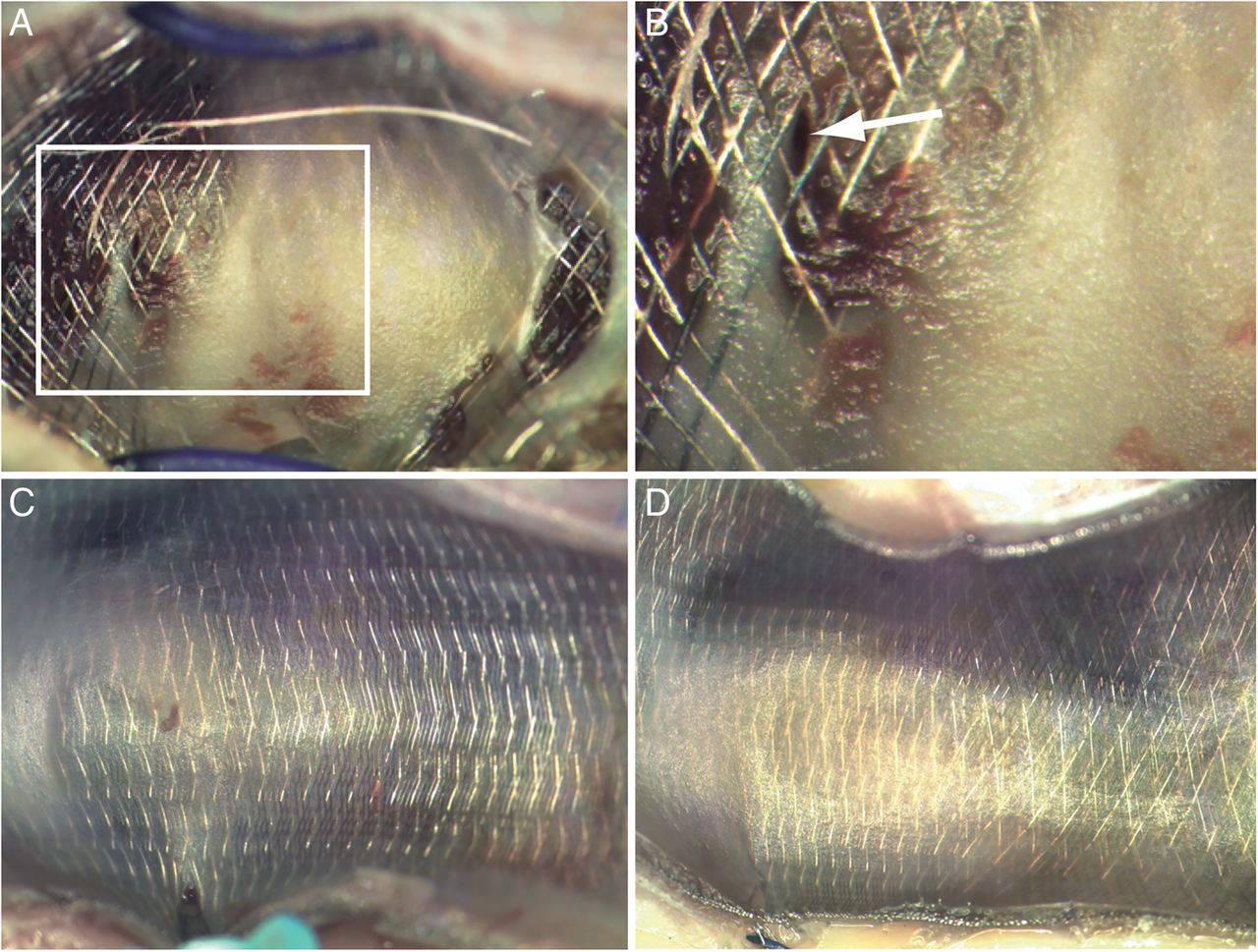
En face views of flow diverters (FDs) covering the aneurysm ostia. (A) Non-compacted FD showing incomplete neointimal coverage with apertures in the distal transition zone (B). (C) Compacted FD showing complete neointimal coverage, which also occurred when two overlapping FDs were used (D).
Aneurysms treated with non-compacted FDs showed leaks or apertures through the neointima covering the FD mesh in all cases, with only three of six cases showing near-complete coverage (90%). Three cases had large areas of bare FD struts, with adherent red material (figure 3A, B), usually located in the distal transition zone of the device. Residual aneurysms were partially filled with thrombus of varying ages. Aneurysms treated with two telescoping compacted FDs (figure 3D) showed complete coverage with thick neointima in three of four cases, with almost complete coverage of the aneurysm ostium in the fourth case. Aneurysms were completely occluded and filled with connective tissue.
The deployed PEDs were well apposed to the parent artery in all cases, without neointimal hyperplasia around the terminal ends of the devices (figure 4).

(A) Three-month angiography showing no significant parent vessel stenosis (arrow: small residual aneurysm filling). (B) and (C) show mature tissue coverage over the ends of the device without neointimal proliferation.
Microscopic pathology
When the aneurysm was completely occluded by the FD, the fundus was filled with organized thrombus, and the FD spanning the neck was covered with neointima (figure 5A). Incompletely occluded aneurysms (figure 5B, C) were characterized by the presence of thrombus, in varying stages of organization. Residual aneurysms were fed by endothelial cell-lined crevices, which occasionally were found to exit the confines of the neointima-covered FD (figure 5C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Microscopic pathology (hematoxylin phloxine saffron) of (A) organized thrombus inside completely occluded aneurysm, (B) thrombus in various stages of organization, (C) patent residual aneurysm cavity (*), (D) endothelial-lined channel (**) outside the confines of the flow diverter struts (*), which are well-covered with neointima.
Discussion
The salient feature of this study is the demonstration that technical differences in FD deployment can affect the angiographic results. Intentional compaction of the device along the long axis can reduce the size of leaks or holes in the neointima covering the FD and increase the likelihood of aneurysm occlusion. This work confirms in an in vivo model the potential importance of deployment technique in the outcome of aneurysms treatment, as has been suggested with computational fluid dynamics and bench-top studies.5 ,8 ,15
Leaks or holes through the neointimal coverage over the aneurysm ostium were found in persistent aneurysms when the device was not compacted. These leaks were predictably located at the site of the more porous distal transition zone of the device.15 Device compaction helps to increase the metallic coverage of the aneurysm ostium, and increasing metallic density is known to be associated with increasing neointima formation.3 Although compaction maneuvers over the aneurysm ostia may increase strut density, this same maneuver may also increase the ischemic risks to branches jailed by a compacted device.
Excessive compaction was associated with device prolapse. A second device was required to salvage four aneurysms in the compacted group. The application of forward pressure required to compact the devices may also increase the likelihood of delayed stent ‘creep’,16 which might have been responsible for the distal FD migration seen in one case.
Prolapse of FDs during deployment can be a difficult complication to manage,17 particularly when distal wire access is lost and the proximal landing zone has fallen into the aneurysm. Maintaining distal wire access in the event of prolapse is crucially important, as this permits placement of an additional device to create a multi-device construct. Although additional metal coverage provided by using two overlapping FDs may favor aneurysm occlusion, it may also increase the risk of ischemia in vessels jailed by the devices.
Limitations
The number of animals and aneurysms was small. We chose a model allowing the construction of two aneurysms per animal. The study was designed as an exploration and the sample size was not predetermined according to a precise hypothesis; groups were defined in a post hoc fashion in order to make meaningful comparisons. For example, immediate failures were rescued by forming group 1b, composed of aneurysms treated with two FDs, which could no longer be compared with other lesions treated with a single device. Such a strategy may spuriously increase the statistical significance of findings, but it is in line with a philosophy of assuring the experimental efficiency while minimizing the number of animals used to make meaningful comparisons. Because the model does not feature a branch jailed by the FD, we were unable to study the effect of device compaction on branch occlusion. Although the rate of persistent aneurysms was lower than we have historically observed, strictly speaking results cannot be compared because the models differed.3
Devices cannot be uniformly compacted throughout deployment. The ‘compaction index’ we used was a convenient tool to compare means between two groups. It provided only a global measurement, not taking account of heterogeneities in porosity that are known to occur along the length of the same device.15
Animal models certainly differ from human aneurysms, and extrapolation of these data to clinical applications should be cautious. The canine wide-necked aneurysms can mimic some, but certainly not all, of the challenges in treating clinically encountered aneurysms. The absence of a proximal carotid siphon in canines may make it easier to achieve device compaction in an animal than in a human.
The animal model we chose may be more challenging than other available models, such as the rabbit elastase models, which typically have smaller aneurysms with smaller necks.18 The choice of a wide-necked aneurysm model may explain why a second device was required to completely cover the aneurysm neck in some cases. Re-sheathable Pipeline devices were not available at the time of this work; whether re-sheathability would permit compaction without increasing risks of malpositioning remains to be studied. Choice of longer devices, with larger landing zones, may be necessary if compaction maneuvers are contemplated.
Conclusion
Compaction of FDs across wide-necked canine aneurysms improves angiographic aneurysm occlusion rates at 3 months. Excessive compaction may increase risks of device mal-positioning.
References
Footnotes
Contributors Conception and design: TD, JR, IS, J-CG; collection and assembly of data, data analysis and interpretation, manuscript writing: TD, JR, J-CG, IS, GG; final approval of manuscript: TD, JR.
Funding This work was supported by a grant from the Heart and Stroke Foundation of Alberta (GIA-0200296) to TD. The authors also thank Covidien (Medtronic) for providing free of charge the flow diverters used in this study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Animal studies Principles of laboratory animal care (NIH publication No 86-23, revised 1985) were followed, as well as the guidelines of the Canadian Council on Animal Care. The protocol for animal experimentation was approved by the Institutional Animal Care Committee of our institution (CIPA).