Article Text

Abstract
Spinal epidural arteriovenous fistulas (SEDAVFs) are rare complex lesions often presenting with protean clinical manifestations secondary to compressive symptoms or congestive myelopathy. The imaging manifestations of SEDAVFs on MR angiography/MRI include high T2 signal in the spinal cord, vascular engorgement of the epidural space, and prominent intradural vascular flow voids. Given the complexity of these lesions, they are best characterized anatomically on catheter angiography where careful inspection of arterial feeders and venous drainage patterns can be performed. The imaging hallmark of an SEDAVF on angiography is the presence of a dilated epidural venous pouch through which spinal and paraspinal veins are secondarily opacified. In the lower thoracic and lumbar spine, SEDAVFs are usually located in the ventral epidural space and fed mainly by the anteriorly coursing epidural arteries. In the cervical and upper thoracic spine, SEDAVFs and their feeding arteries are more typically located laterally in the spinal canal. Current treatment options include transarterial or transvenous endovascular embolization with liquid embolic agents or coils, and surgical resection/disconnection of the fistula. Further research is needed to better characterize how and why these lesions form and to identify the best treatment modalities.
- Arteriovenous Malformation
- Epidural
- Fistula
- Spine
Statistics from Altmetric.com
Introduction
Spinal epidural arteriovenous fistulas (SEDAVFs) are a rare type of spinal arteriovenous fistula which occurs between branches of the paraspinal or paravertebral arterial system and the epidural venous plexus.1–3 These lesions can present with compressive symptoms or congestive myelopathy,1 ,2 and can be difficult to distinguish from the more common and better described spinal dural arteriovenous fistulas (SDAVF). In this review, we describe the anatomy, physiology, clinical presentation, imaging, and treatment options for SEDAVFs.
Anatomy and angioarchitecture
Arterial anatomy
SEDAVFs typically form in the anterior or lateral epidural space at the retrocorporeal arcade located just posterior to the vertebral body.4–7 In the thoracic and lumbar spine, intercostal and segmental arteries arising off of the aorta give off a dorsal somatic branch which traverses through the neural foramen to supply the epidural arterial arcade; a network of vessels that runs continuously up and down the spinal epidural space with a rich anastomotic supply. Ventral somatic branches which arise from the main segmental artery supply the vertebral body itself.4–6
Because of the rich arterial supply to the epidural arterial arcade, SEDAVFs often have multiple feeding arteries. Arterial supplies reported in the literature include dorsal and ventral somatic branches from the intercostal and lumbar segmental arteries for lesions located in the thoracic and lumbar spine; the lateral sacral artery for lesions located in the sacrum; and branches of the ascending/deep cervical arteries and vertebral arteries for SEDAVFs and vertebral–vertebral arteriovenous fistulas (VVAVFs) in the cervical spine.8 ,9 The feeding arteries typically drain into a shunted ventral epidural venous pouch.8 ,9 Because the radiculomedullary and radiculopial arteries can have a common origin with a feeder to an SEDAVF, close inspection of spinal angiograms prior to intervention is essential.
Venous anatomy
The epidural venous plexus is a valveless arcade of veins that extends from the skull base to the sacrum and drains into the foraminal and paraspinal venous. This serves as a source of venous drainage for the spinal cord and vertebrae, and facilitates CSF drainage.8 ,9 Spinal bridging veins, which connect the epidural venous plexus to the perimedullary veins, serve as a conduit between the extradural and intradural venous systems. These bridging veins have a reflux impeding mechanism which under normal physiologic circumstances inhibits reflux of blood from the epidural venous plexus into the perimedullary veins due to narrowing and zigzagging of the bridging vein when it crosses the dura.7 There is also a posterior venous plexus but this is usually not well appreciated angiographically and is usually not involved in any pathological processes.4–6
It is important to note that the lower thoracic and lumbar spines have a large ventral epidural space. Therefore, epidural arteriovenous fistulas (AVFs) at these locations are usually located in the ventral epidural space and fed mainly by the anterior epidural arteries showing a medial course. However, in the cervical spines and upper thoracic spine, the ventral epidural space is located more laterally due to a thick and large posterior longitudinal ligament. Therefore, epidural AVFs of the cervical and upper thoracic spine are usually located laterally in the spinal canal, and their feeding arteries are also located laterally in the canal.
The epidural venous plexus has multiple efferent draining veins depending on the level. At the cervical level, the plexus drains into the suboccipital venous system. At the thoracic level, the veins drain into the azygous and hemiazygous systems. At the lumbar level, the plexus drains into the ascending lumbar, iliac, and azygous veins. There is also some direct drainage into the left renal vein and inferior vena cava. The sacral epidural plexus drains into the lateral sacral veins.8 ,9
Classification
SEDAVFs are typically classified by their venous drainage patterns.10 SEDAVFs with intradural/perimedullary drainage are associated with myelopathy secondary to venous congestion of the spinal cord and have clinical characteristics indistinguishable from the more common SDAVF (figures 1 and 2). SEDAVFs with pure extradural/paravertebral drainage are not associated with congestive myelopathies, but rather can cause symptoms through compression and mass effect due to engorgement of the epidural venous plexus (figure 3). In some cases, lesions with pure extradural/paravertebral drainage can present as incidental findings as they are characterized by epidural venous plexus engorgement but lack of radiographic or clinical mass effect.10 ,11 Some lesions have combined perimedullary and paravertebral venous drainage.

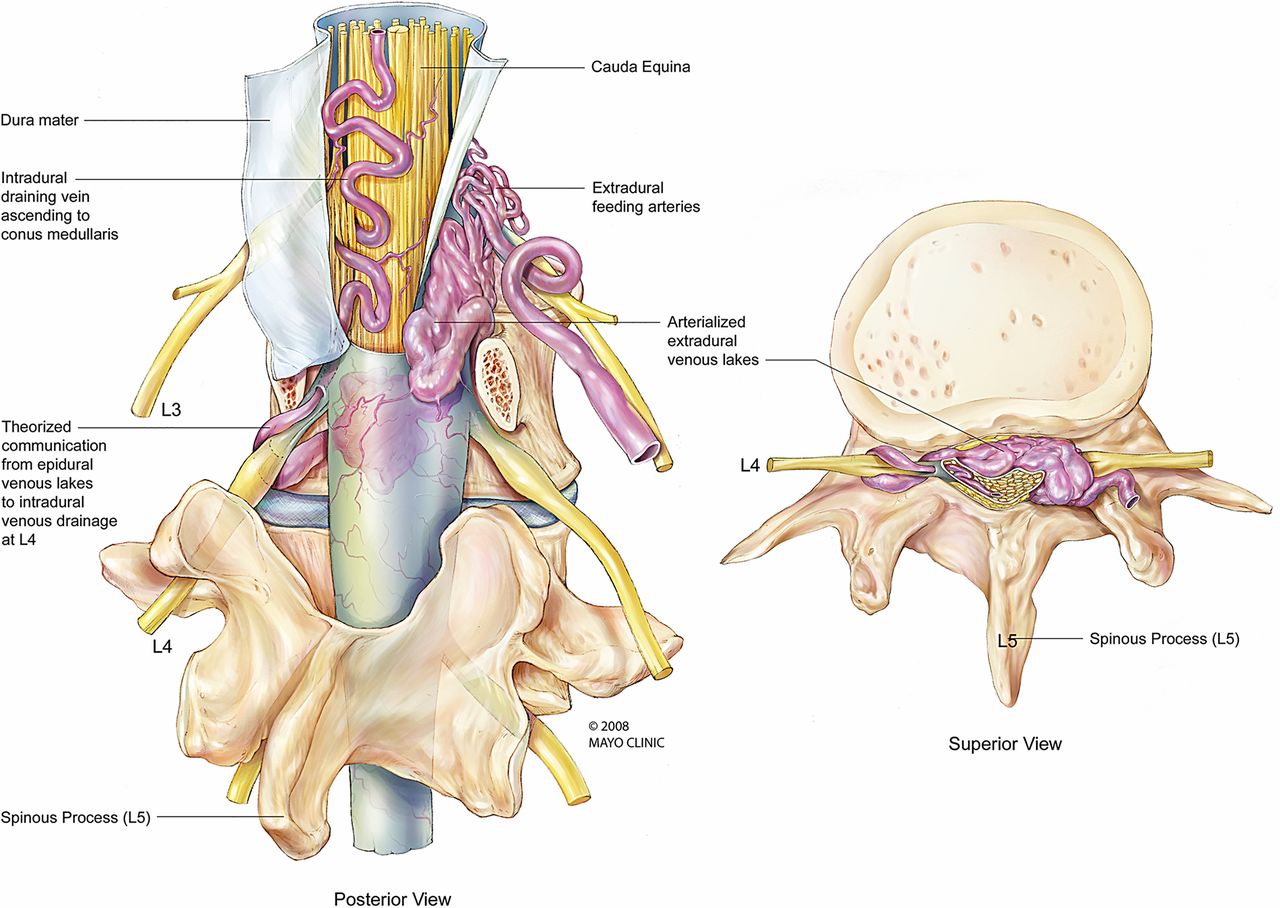
Graphic representation of a spinal epidural arteriovenous fistula.

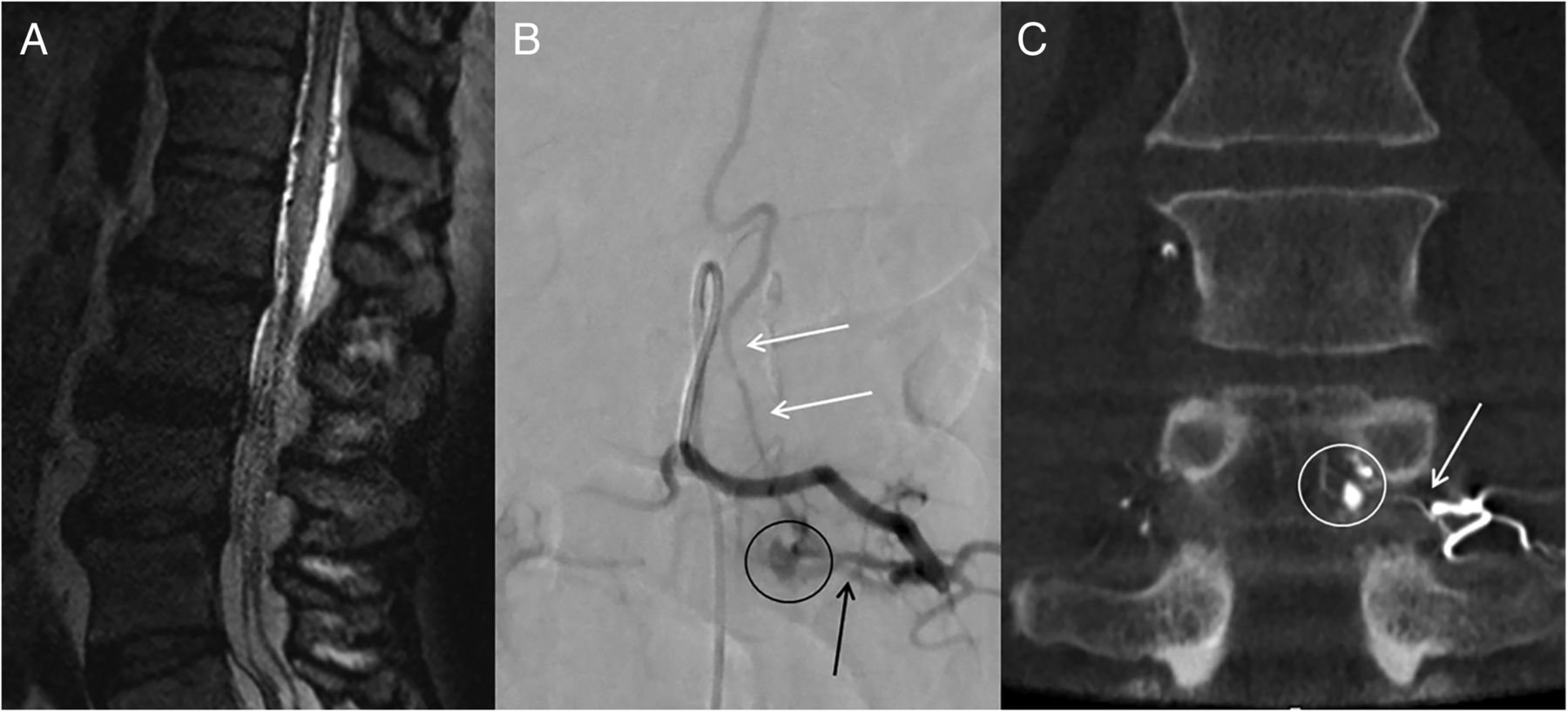
Spinal epidural arteriovenous fistula with intradural venous drainage in a patient status post-laminectomy. The patient had a prior history of L3 laminectomy. He presented with new myelopathic symptoms about 1 year following his surgery. (A) MRI demonstrates multiple intradural flow voids and high T2 signal in the conus. (B) Conventional spinal angiographic images following injection of the left L3 segmental artery in anteroposterior and lateral views demonstrates a medially coursing artery (black arrow) connecting with a venous pouch in the epidural space (black circle). The intradural draining vein is seen coursing up the spinal canal (white arrows). (C) Flat panel CT images demonstrate the medially coursing artery (white arrow) with the venous pouch in the epidural space representing the site of the fistula (white circle).

Spinal epidural arteriovenous fistula with pure epidural venous drainage. The patient presented with symptoms of a progressive thoracic myelopathy. (A) T2 weighted MRI images demonstrate a flow void in this lesion (white arrow) and high T2 signal in the cord at this level. (B) Conventional spinal angiogram following injection of the left T5 intercostal artery demonstrates a large arteriovenous fistula in the epidural space with no evidence of intradural spinal venous drainage.
It is important to highlight the differences in angioarchitecture between SDAVFs and SEDAVFs. In SEDAVFs, the arteriovenous shunt lies in the epidural space and the intradural draining vein arises from a venous pouch whereas in the SDAVF the arteriovenous shunt lies within the dura of the nerve root sleeve and drains directly into an intradural vein without filling of the epidural space.11 The fistulous radicular vein typically drains in a retrograde fashion into the longitudinal venous network of the spinal cord through a radiculomedullary vein.3 ,7 ,12
Included in the spectrum of SEDAVFs are extracranial vertebrovertebral fistulae. VVAVFs represent abnormal high flow shunts between the extracranial vertebral artery or one of its branches and the adjacent vertebral veins. While occasionally there is retrograde drainage from the vertebral vein to the epidural venous plexus, this is sometimes considered a different entity from SEDAVF due to the fact that the fistulous connection is not in the epidural space but rather the paravertebral venous plexus.13 These rare lesions are most commonly caused by trauma but can be congenital or spontaneous/idiopathic as in the case of connective tissue disorders such as neurofibromatosis type 1, Marfan's syndrome, fibromuscular dysplasia, or Ehlers–Danlos.13
Pathogenesis
The pathogenesis of SEDAVFs remains unclear. Many reports suggest an association between SEDAVFs and prior surgery or trauma14 (figure 2). However, one systematic review including 101 cases found that only 10% of patients had a prior history of spinal surgery.3 Connective tissue diseases such as fibromuscular dysplasia, neurofibromatosis type 1, Marfan's syndrome and Ehlers–Danlos syndromes are often seen in the setting of VVAVFs.3 However, the majority of SEDAVFs and VVAVFs are likely idiopathic. Surgery is considered a culprit in some cases as mechanical injury of one of the small epidural arteries can induce a small arteriovenous fistula. It has also been proposed that surgical interruption of the epidural venous drainage can result in venous thrombosis and subsequent abnormal recanalization, a mechanism similar to acquired cranial dural AVFs.15 ,16
Clinical manifestations
Only a limited number of cases of SEDAVF are reported in the literature. Unlike SDAVFs, the male:female ratio of SEDAVF patients is 1:1.3 According to one large systematic review, patients with SEDAVFs tend to be younger than those with SDAVFs (mean age 46 years).3 SEDAVFs of the lumbosacral spine are typically seen in older patients with a male predilection while a majority of cervical SEDAVFs are found in women.3
A prospective clinical diagnosis of SEDAVFs is all but impossible due to the protean clinical manifestations of these lesions. The clinical manifestations of these lesions depend solely on the venous drainage pattern.10 The two main causes of neurological deficits associated with these lesions are mass effect and medullary venous hypertension. Rarely, these lesions can present with epidural or intradural hemorrhage.3 ,15 ,17–25 In some cases these lesions are completely asymptomatic.
SEDAVFs with intradural venous drainage are generally diagnosed in patients around the sixth decade of life. These lesions are seen mainly in the thoracolumbar and lumbar regions, a distribution similar to dural AVFs.3 ,10 The reason that these lesions are seen mainly in the lower spinal region may be attributable to a rich vascular network between the intradural and extradural venous systems in this region26 and to the possible association with trauma and surgery, both of which are more common in the lower thoracic and lumbar area. These lesions typically present with myelopathy, sensory and motor radiculopathy, and sphincter malfunction. Transient worsening of symptoms with Valsalva (which increases the intradural congestion) is not uncommon. Similar to SDAVFs, the onset of these symptoms is often slow and progressive.3 ,10 Venous hypertension and congestion result in vasogenic edema and are reversible, whereas venous infarction results in cytotoxic edema and is irreversible. Thus early diagnosis and treatment are essential to achieve a favorable outcome in such cases because venous congestion results in irreversible venous infarction within a short period.27
SEDAVFs without intradural venous drainage are diagnosed in patients around the third decade of life and often result in mass effect resulting in myelopathy secondary to an enlarged extradural venous plexus or radiculopathy from extradural nerve root compression.3 ,10 These lesions can be seen at all spinal levels but are most commonly present at the cervical and upper thoracic spinal levels. These lesions are typically fed by vertebral, ascending cervical, and deep cervical arteries, and exhibit high flow.26
The clinical manifestations of VVAVFs are related to reduction of arterial flow in the region distal to the fistula and include vertebrobasilar insufficiency and spinal cord ischemia. If there is venous hypertension, VVAVFs can open into a radicular vein and lead to medullary venous hypertension which can result in myelopathy or hemorrhage. Large epidural and extradural venous lakes can result in compressive symptoms, including radiculopathy and compressive myelopathy.
Imaging
MRI appearance
SEDAVFs in the thoracolumbar and sacral region are generally indistinguishable from SDAVFs on cross sectional imaging. On MRI, lesions with perimedullary venous drainage typically present as a conglomerate of dilated intradural vessels with flow voids on T2 weighted images which enhance with contrast. In the presence of a sacral SEDAVF with intradural drainage, flow voids along the spinal cord may not be prominent. However, close inspection often reveals a prominent and dilated vein ascending from the sacrum to the conus (figure 4). Intramedullary enhancement or pial enhancement of the cord surface can also be seen.26 ,28 T2 weighted images also demonstrate increased signal and swelling of the spinal cord which is secondary to chronic venous congestion.
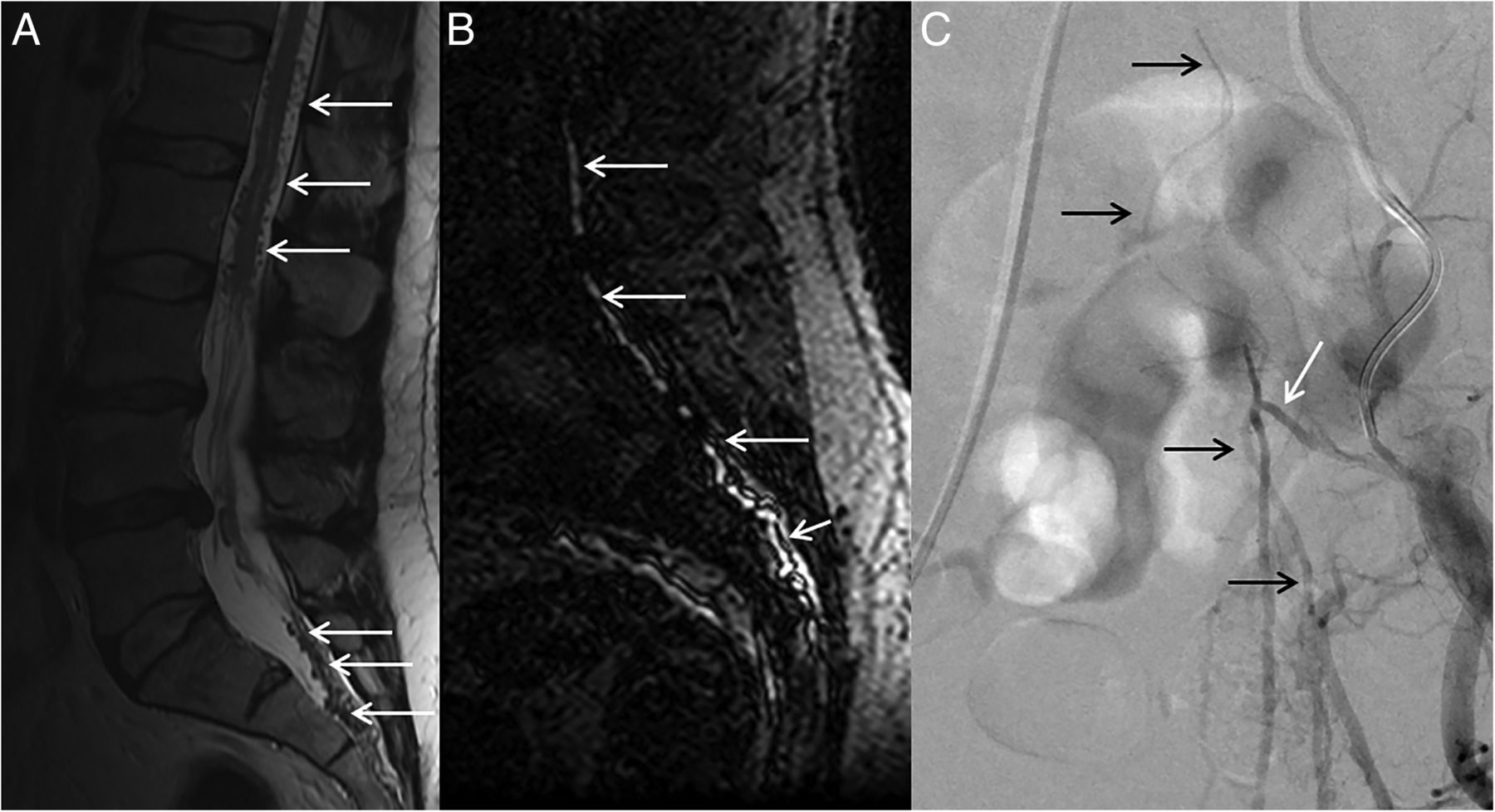
Sacral epidural arteriovenous fistula. (A) T2 weighted MRI demonstrates high T2 signal in the conus with multiple intradural flow voids (white arrows). (B) Spinal MR angiography demonstrates a large dilated intradural vein (white arrows). (C) Left iliac angiogram demonstrates a dilated intradural vein coursing up and down the spinal canal (black arrow). The feeding artery enters at the left S4 neural foramina (white arrow) and there is a small fistulous connection.
SEDAVFs with intradural venous drainage are sometimes distinguished from an SDAVF by the presence of a dilated extradural venous varix. Lesions without intradural venous drainage typically demonstrate normal signal intensity of the spinal cord on MR imaging with lack of intradural flow voids or enhancing vessels. These lesions can sometimes be identified on cross sectional images by the presence of epidural thickening and the presence of a large venous varix.28
MR angiography
The primary utility of MR angiography (MRA) is for treatment planning and post-treatment follow-up. In general, it is extremely difficult to distinguish an SEDAVF from an SDAVF on MRA, but MRA can at least provide important clues regarding location that can allow for rapid identification of the fistula on conventional angiography. The MRA appearance of SEDAVFs with intradural venous drainage is similar to that of SDVAFs. The best MRA techniques available to diagnose these lesions are three-dimensional (3D) contrast enhanced MRA (CE-MRA) and 4D time resolved MRA (TR-MRA). 3D-CE MRA typically uses double or triple doses of gadolinium.28 Images are typically obtained in three phases: one phase without contrast for subtraction followed by arterial and venous phases. The major drawback of this imaging technique is the lack of high temporal resolution which can limit understanding of venous drainage patterns and make it difficult to differentiate arteries from veins.28 Studies using 3D-MRA demonstrate a sensitivity of about 90–95% in identifying spinal fistulas. In 70–80% of cases the level of the fistula can be identified, thus facilitating spinal angiography.28
Four-dimensional imaging with time resolved imaging of contrast kinetics (TRICKS) is increasingly used in the diagnosis of spinal arteriovenous malformations.29 This imaging modality allows for fast time resolved imaging, allowing for assessment of fistula hemodynamics with high spatial resolution and signal to noise ratio. Multiphase imaging with TRICKS has been shown to provide increased accuracy in not only identifying spinal arteriovenous malformations, but also in localizing the arterial feeders and venous drainage patterns. There are a few reports of the use of TRICKS and other 4D techniques in the assessment of SEDAVFs which have demonstrated promising results. Imaging with TRICKS is superior to 3D-CE-MRA in identifying the presence and location of spinal fistulae.29
CT and CTA
CT angiography (CTA) can be a useful tool in the detection of SEDAVFs in patients who are unable to tolerate MR imaging but is limited by high radiation doses. Similar to MRA, primary utility of CTA is for treatment planning and post-treatment follow-up. Similar to MRI, SEDAVFs with intradural venous drainage can potentially be differentiated from SDAVFs by the presence of a large venous pouch or engorgement of the epidural venous plexus. The sensitivity of CTA in identifying spinal arteriovenous fistulae in general is 80–100%, depending on the series. The ability of CTA in characterizing SEDAVFs has not been systematically studied however. One recently published study used 4D-CTA with a 320 row area detector in evaluating a small series of spinal fistulae and found that this technique was successful in localizing the one SEDAVF in their series and in characterizing the flow direction of perimedullary venous drainage.30
Angiographic appearance
Digital subtraction angiography (DSA) remains the gold standard in the diagnosis and evaluation of SEDAVFs.8 ,9 ,31 DSA offers a dynamic evaluation of the fistula, allowing one to parse out the angioarchitecture of the lesion, including arterial feeders, the appearance of the nidus/venous pouch, and the venous drainage patterns. Evaluation of these lesions requires meticulous spinal angiography with selective injection of all segmental vessels, the internal iliac arteries, vertebral arteries, deep cervical arteries, and costocervical arteries. This is particularly important for planning of transarterial embolization as these lesions can have multiple arterial feeders, and arteries distant to the nidus may supply the fistula. Conventional spinal angiography is also the most sensitive and specific modality for identifying vessels supplying the anterior and posterior spinal arteries.8 ,9 ,31
Three-dimensional rotational angiography is often used in imaging of SEDAVFs as it can provide detailed anatomic information with separation of the arteriovenous system. Images are typically performed within 5 s and provide excellent detail. Recently, cone beam CT has been introduced as an adjunct to spinal angiography and has proven to be extremely useful in the characterization of these lesions. Cone beam CT allows for a better understanding of the relationship between the SEDAVF and the spinal canal, spinal cord, nerve roots, and surrounding soft tissue structures.11 When performing a cone beam CT, a 3D-CT reconstruction is produced from 2D projectional images through rotation of the C arm around the patient. The scan is typically performed over the course of 20–30 s while hand injecting 30–40 mL of dilute contrast through the feeding pedicle.11 One of the limitations of this modality is the long scanning time and difficulty in differentiating arteries from veins in the AV shunt.
The imaging hallmark of an SEDAVF on angiography is the presence of a dilated epidural venous pouch through which spinal and paraspinal veins are secondarily opacified (figures 2, 3, and 5). Another angiographic clue to the presence of an SEDAVF rather than an SDAVF is the medial course of the feeding artery and a more anteromedial location of the site of the fistula if it is located in the lower thoracic or lumbar spine and lateral location if the fistula is located in the upper thoracic or cervical spine. This is a reflection of the location of the epidural venous plexus at these locations.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
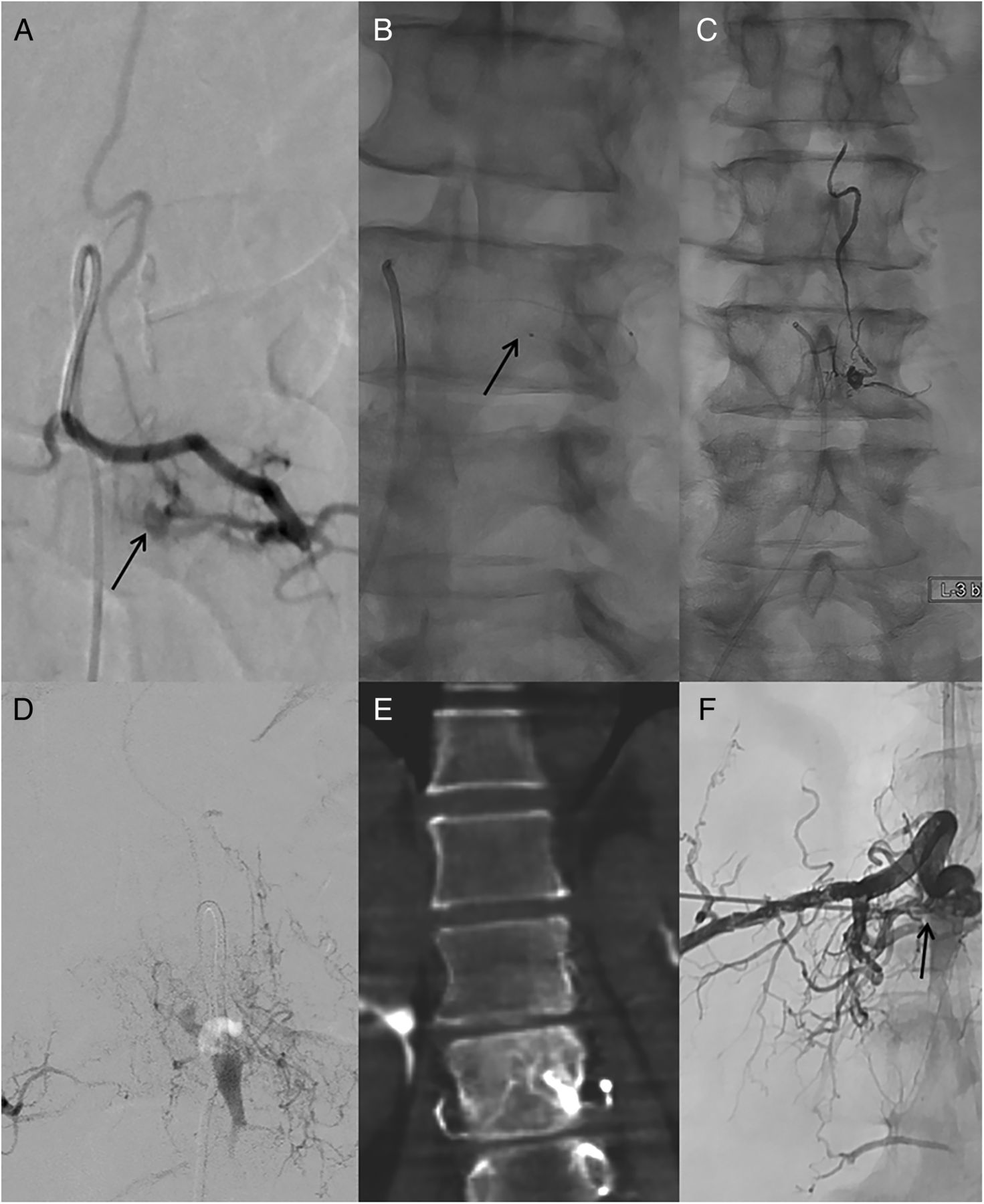
Image guided treatment of spinal epidural arteriovenous fistulas. (A) Left L3 injection in an epidural arteriovenous fistula. The point of the fistula is marked by the black arrow. (B) The tip of the microcatheter is located just proximal to the fistulous pouch (black arrow). (C) Following injection of Onyx, there is Onyx filling of the fistulous pouch as well as the draining intradural vein and feeding artery. (D–F) Example of a fistula treated with both endovascular and direct percutaneous puncture of the venous pouch. (D) Injection of the feeding artery demonstrates a persistent venous pouch despite prior Onyx embolization. (E) Flat panel CT demonstrated the dilated venous pouch. (F) Direct puncture of the venous pouch under fluoroscopic guidance was performed followed by Onyx injection (black arrow).
VVAVFs are angiographically distinct from SEDAVFs of the thoracic, lumbar, and sacral spine. VVAVFs can manifest as either a small hole in the vertebral artery communicating directly with the vertebral veins or as a direct fistulous connection between a vertebral artery branch and the vertebral veins. VVAVFs in the lower cervical spine are often supplied by ascending and deep cervical branches and drain directly into the epidural space.
Treatment
Surgical and endovascular treatments are the primary treatment modalities for SEDAVFs. The therapeutic goal in treating epidural AVFs is to obliterate the fistulous communication between the feeding artery and the draining vein as well as the proximal venous drainage by means of surgery or endovascular embolization.2 ,32 Currently, endovascular treatment is the favored method of treatment, with about two-thirds of studies and case reports reporting the use of endovascular treatment.3 In their systematic review of endovascular and surgical management of SEDAVFs, Huang et al3 reported initial occlusion rates of 55% with endovascular treatment which increased to 92% on follow-up following staged treatments. Transarterial embolization was the primary means of treatment in their series. Clinical improvement rates were 91% with endovascular treatment, with only 3% reporting worsening of symptoms. With surgical treatment, Huang et al reported complete occlusion rates of 74% on initial treatment and 87% on follow-up after final treatment attempts. Clinical improvement rates with surgery were 84%, with only 9% of patients reporting worsening of symptoms.3
Endovascular treatment of SEDAVFs with intradural venous drainage is focused on occlusion of the venous pouch along with the proximal intradural draining vein (figure 5). Failure to obliterate the pouch and draining vein can result in recanalization due to de novo recruitment of additional arterial feeders.5 This is particularly true for cervical fistulae. Transarterial embolization is often difficult to perform when the feeding arteries are small or tortuous. The primary complication of transarterial embolization is inadvertent embolization of the radiculomedullary artery. Thus careful examination of the arterial distribution at a few levels above and below the actual connection is paramount. It is also important to consider that the lack of angiographic visualization of the vascular cord supply does not exclude the possibility of the vascular supply from the same pedicle feeding the SEDAVF. Small posterior spinal arteries ascending with the corresponding nerve root are often present at many segments even though they may not necessarily be visualized.
In the setting of large venous pouches, embolization can be difficult due to the large amount of embolic material required to achieve complete obliteration. This is a particular problem in the treatment of SEDAVFs with pure extradural venous drainage where symptom onset often occurs once the venous pouch has become large enough to produce mass effect.
The primary embolic agents used to treat SEDAVFs are Onyx and n-Butyl cyanoacrylate (n-BCA) glue.2 ,11 ,33–35 Each material has advantages and disadvantages, and there are no data to support the superiority of one embolic agent over the other.4 In our practice, Onyx is the primary embolic agent used for treatment of spinal fistulas. During transarterial embolization, Onyx is able to permeate to the venous side of the AVF and can also fill other arterial feeding vessels in a retrograde fashion, thus facilitating complete closure of the AVF.2 ,11 ,33–35 In addition, Onyx can be delivered more slowly than n-BCA, allowing for a more controlled injection. The superior penetration of the fistula with Onyx when compared with glue allows one to avoid distal catheterization which can prove to be quite challenging in very small, tortuous, and distal vessels. Lastly, Onyx is non-thrombogenic and cohesive which allows for better packing of the epidural venous pouch without the risk of thrombus formation and embolization. One drawback of liquid embolic agents is the risk of proximal reflux which can compromise the normal vasculature, including the radiculomedullary artery.
Transvenous embolization of SEDAVFs has also been reported in about 10% of reported cases.3 In addition to intradural perimedullary veins, the draining veins of SEDAVFs include veins of the azygous venous system which contains valves and metameric connections to the paraspinal longitudinal veins thus complicating transvenous embolization. Transvenous embolization has been reported to be more effective than transarterial embolization in the setting of multiple arterial feeders. One unique approach to transvenous embolization was reported by Ramanathan et al who performed direct percutaneous embolization of an epidural venous pouch with n-BCA glue. Such an approach obviates the need for catheterization of the azygous venous system which can be technically difficult2 (figure 5).
In general, transarterial embolization of high and mid cervical SEDAVFs and VVAVFs is more difficult than other locations as these fistulae are usually fed by small and short branches of the vertebral artery. Furthermore, these lesions are generally more complex and can be fed by pial arteries or be associated with perimedullary AVFs. In such cases, strategies focused on avoiding reflux of embolic agents into the vertebral artery or radiculomedullary arteries are key. Coil embolization is sometimes chosen over the use of a liquid embolic agent due to the risk of reflux of embolic agent into the vertebral or anterior spinal artery and has been shown to be effective in some cases.36 ,37 In cases where the VVAVF is a direct fistulous connection between the vertebral artery and vein, transvenous embolization focusing on the venous portion of the fistula is sometimes performed due to the risk of stroke from thrombosis of the vertebral artery.
Surgical treatment is generally reserved for lesions that are difficult to treat with endovascular management or after failed endovascular treatment. Surgical treatment typically consists of direct ligation and interruption of the fistula at the site of the shunt and draining vein.38 Surgical treatment is often preferred when the fistula is close to the anterior spinal artery or in the setting of multiple arterial feeders to a high flow fistula, which can make transarterial embolization more difficult. One advantage of surgical treatment is the opportunity to perform both decompression and ligation, thus reducing the SEDAVF associated mass effect. This treatment strategy is particularly useful in lesions without intradural venous drainage.
In lesions with intradural venous drainage, surgical treatment typically consists of obliteration of both the epidural venous lake and the intradural draining vein. However, in one recently published series of four patients, Niizuma et al reported complete obliteration of three of four SEDAVFs treated with disconnection of the intradural draining vein without manipulation of the venous lake itself. In the one unsuccessful case of isolated draining vein ligation, there were multiple intradural draining veins, suggesting that the fistula was more complex.39 Surgical treatment is not always straightforward due to the often anterior location of these lesions which can make adequate exposure from a posterolateral approach difficult.
Conclusions
SEDAVFs are rare and complex lesions often presenting with protean clinical manifestations secondary to compressive symptoms or congestive myelopathy. Given the complexity of these lesions, SEDAVFs are best characterized anatomically on catheter angiography where careful inspection of arterial feeders and venous drainage patterns can be performed. Current treatment options include endovascular embolization with liquid embolic agents or coils, and surgical resection/disconnection of the fistula. Further research is needed to better characterize how and why these lesions form and to identify the best treatment modalities.
References
Footnotes
Contributors RY, WB, DMN and GL participated in drafting the article and revising it critically for important intellectual content. These authors made substantial contributions to conception and design, acquisition of the data, and analysis and interpretation of the data. All authors provided final approval of the version to be published.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.