Article Text

Abstract
Background and purpose The benefits of mechanical thrombectomy (MT) in basilar artery occlusions (BAO) have not been explored in recent clinical trials. We compared outcomes and procedural complications of MT in BAO with anterior circulation occlusions.
Methods Data from the Madrid Stroke Network multicenter prospective registry were analyzed, including baseline characteristics, procedure times, procedural complications, symptomatic intracranial hemorrhage (SICH), modified Rankin Scale (mRS), and mortality at 3 months.
Results Of 479 patients treated with MT, 52 (11%) had BAO. The onset to reperfusion time lapse was longer in patients with BAO (median (IQR) 385 min (320–540) vs 315 min (240–415), p<0.001), as was the duration of the procedures (100 min (40–130) vs 60 min (39–90), p=0.006). Moreover, the recanalization rate was lower (75% vs 84%, p=0.01). A trend toward more procedural complications was observed in patients with BAO (32% vs 21%, p=0.075). The frequency of SICH was 2% vs 5% (p=0.25). At 3 months, patients with BAO had a lower rate of independence (mRS 0–2) (40% vs 58%, p=0.016) and higher mortality (33% vs 12%, p<0.001). The rate of futile recanalization was 50% in BAO versus 35% in anterior circulation occlusions (p=0.05). Age and duration of the procedure were significant predictors of futile recanalization in BAO.
Conclusions MT is more laborious and shows more procedural complications in BAO than in anterior circulation strokes. The likelihood of futile recanalization is higher in BAO and is associated with greater age and longer procedure duration. A refinement of endovascular procedures for BAO might help optimize the results.
- Stroke
- Thrombectomy
- Complication
- Intervention
Statistics from Altmetric.com
Introduction
Basilar artery occlusion (BAO) is a devastating form of stroke that carries a high rate of mortality and severe disability, especially if recanalization does not occur.1 ,2 Recanalization is the best predictor of a good outcome among patients with BAO. However, the available data indicate that successful recanalization increases the probability of survival but not necessarily a recovery free of disability, given that studies show a high rate of futile recanalization.3 ,4 BAO is hardly represented in randomized clinical trials (RCTs) on reperfusion therapies and most data regarding safety and efficacy of these treatments are obtained from cohort studies. Low to moderate recanalization rates and poor outcomes have been reported for BAO treated with IV or IA thrombolysis,1 ,5 whereas mechanical thrombectomy (MT) appears to be safe and to increase recanalization.3 ,4 Data from the International Multicenter Registry for Mechanical Recanalization Procedures in Acute Stroke (ENDOSTROKE) suggest that the use of stent retrievers in BAO occlusions is a predictor of recanalization, but recanalization was not a predictor of good outcome.6 Patients with BAO were not included in the most recent RCT of endovascular treatment with stent retrievers that demonstrated efficacy of MT in strokes due to anterior circulation occlusions,7–11 thus the efficacy of MT using stent retrievers in BAO strokes is yet to be ascertained. The phase III RCT Basilar Artery International Cooperation Study (BASICS) initiated in 2011 is planned to finish in 2017.12 Meanwhile, guidelines for endovascular therapy in acute ischemic stroke suggest that, if there are no contraindications, performing MT in basilar thrombosis within the first 6 hours might be reasonable.13 ,14
We therefore analyzed data from the Madrid Stroke Network Registry to investigate the effect of MT, performed according to current recommendations, for BAO strokes in clinical practice and to ascertain whether outcomes for these patients were comparable to those for anterior circulation strokes.
Materials and methods
Study settings, population and treatment protocols
We analyzed data from the prospective registry of the Northeast node of the Madrid Stroke Network, which includes all patients diagnosed with large vessel occlusion (LVO) stroke considered for MT. The Madrid Stroke Network is a collaborative system of care composed of 14 community hospitals, 3 primary stroke centers, and 7 comprehensive stroke centers. MT is provided 24/7 to the population of the Autonomous Community of Madrid via two collaborative nodes (Northeast and Southwest) consisting of three comprehensive stroke centers each, one working as an on-call MT center in a weekly rotating shift. Each node covers half the geographic area and half the population of the region (ie, approximately 3.2 million inhabitants per node) to provide endovascular treatment for every suitable patient. Patients identified by emergency services as suffering a stroke are transferred to the nearest stroke center. If the nearest stroke center is not the one on call for MT, the candidate patient is secondarily transferred once the diagnosis and first-line treatment are performed. The characteristics and operating protocols of the Madrid Stroke Network are published elsewhere.15 ,16
The criteria for MT according to the consensus protocol of the Madrid Stroke Network17 are: (1) acute ischemic stroke due to intracranial LVO confirmed by CT angiography; (2) moderate to severe neurological deficit; (3) time elapsed from stroke onset ≤8 hours for anterior circulation strokes and, in cases of BAO, ≤12 hours in maximum deficit from the start or ≤24 hours for fluctuating or progressing stroke; (4) IV thrombolysis (IVT) failure (persistence of the LVO on CT angiography or transcranial Doppler monitoring and neurological deficit) within the therapeutic window for an endovascular procedure or contraindication for IVT. Initially, our protocols established a waiting period of 30 min after the start of IVT to initiate the endovascular procedures. After publication of the pivotal RCT on MT,5–9 ,13 ,14 protocols for endovascular treatment were initiated as soon as LVO was confirmed and immediately after the start of IVT in patients receiving bridging thrombolysis, and the time from symptom onset to groin puncture was set at <6 hours. If the exact time of symptom onset was not known, it was considered to be the latest time the patient was asymptomatic. When the calculated time from symptom onset among these patients was >6 hours, they were considered for endovascular treatment if they showed a favorable radiological pattern with signs of little damage on CT perfusion (small core of infarct in cerebral blood volume maps and a large region of hypoperfused tissue likely to be salvageable) or MRI (no extensive lesion in FLAIR sequence).
The main exclusion criteria included clinical conditions or comorbidities that might increase procedure risks; a previous condition of dependency for daily living activities; severe established lesions observed on neuroimaging; and a demonstration of a non-favorable mismatch pattern using CT or MRI among those patients with an undefined time from symptom onset.
Patient consent
All patients or their relatives (in case of patient incapacity) provided informed consent prior to inclusion in the MT protocol, which specifically included consent for inclusion of their clinical data in a registry. The registry was approved by the La Paz University Hospital Ethics Committee for Clinical Research and authorization was obtained for its use for investigational purposes. The study was conducted according to the recommendations of the Helsinki Declaration and the Good Clinical Practice guidelines.
Study variables
The following variables recorded in the registry were considered in the present study: demographics, vascular risk factors, and clinical severity at admission according to the National Institute of Health Stroke Scale (NIHSS). The NIHSS score might not accurately reflect clinical severity in posterior circulation stroke, and the score was frequently unavailable for patients with BAO who arrived at the emergency room intubated. Thus, severity on admission was also recorded according to two categories: NIHSS score <15 (mild or moderate strokes) or NIHSS score ≥15 or intubation (severe strokes).18 Other variables registered included the location and angiographic pattern (modified Thrombolysis in Cerebral Ischemia (mTICI) score)19 of vessel occlusion diagnosed initially by CT angiography and digital subtraction angiography in patients undergoing endovascular treatment; treatment or not with IVT; time to IVT and the reason for exclusion when applicable; time from symptom onset to arrival at the hospital for endovascular treatment; time from symptom onset to arterial puncture (OTP); time from door to puncture (DTP); and time from symptom onset to recanalization (OTR), when applicable. Successful recanalization was considered to be a mTICI pattern 2b or 3. The duration and complications of the procedures were also recorded.
Outcome variables included NIHSS at 24 hours or at 7 days or discharge, and at 3 months if available; modified Rankin Scale (mRS) at 3 months; mortality, timing and cause of death; and occurrence of symptomatic cerebral hemorrhage defined according to Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) criteria20 as parenchymal hemorrhage associated with a neurological deterioration of ≥4 points from the lowest NIHSS from baseline or leading to death. Independence was considered to be a mRS score ≤2. Recanalization was considered to be futile when it resulted in death or dependency at 3 months (ie, mRS >2).
Patients considered for endovascular treatment but who were ultimately excluded were also recorded, as were the reasons for exclusion.
Data analyses
For the purposes of the study, patients with isolated vertebral artery (VA) or posterior cerebral artery (PCA) occlusion were excluded from the analysis. Patients lost to follow-up were not considered in the final analysis of outcomes.
Comparisons were made between patients with anterior circulation occlusions, such as intracranial carotid artery (ICA)/T or L occlusion, M1 segment or M2 segment of the middle cerebral artery, and patients with BAO who underwent MT.
Data were expressed as median and IQRs or as mean±SD for continuous variables, or as absolute and relative frequencies for categorical variables. Univariate comparisons between BAO and anterior circulation occlusions regarding baseline characteristic procedures and outcomes were made using Pearson's χ2 test or Fisher's exact test for categorical variables, and the Mann-Whitney U test or Student's t-test for continuous measures, when appropriate. Univariate and multivariate logistic regression analyses using a backward stepwise method to describe the optimal prognostic model were performed to analyze potential prognostic factors. Variables considered in the models were those that have demonstrated prognostic value in the literature and those that were significant in the univariate comparisons between BAO and anterior circulation occlusions. Statistical significance was set at p<0.05. All analyses were performed with the Stata/SE V.12.1 statistical package (StataCorp LP, USA).
Results
Between 1 February 2012 and 31 January 2016, 603 patients were registered. Nineteen patients were excluded from the study because the site of occlusion was not recorded. There were five patients with VA occlusion and six patients with PCA occlusion. Of 573 patients with confirmed LVO (508 (89%) in the anterior circulation and 65 (11%) BAO) who initially fulfilled the criteria for MT, 13 patients with BAO and 81 with anterior circulation strokes were excluded from MT. The reasons for not performing MT were vessel recanalization or significant improvement (spontaneous or after IVT) in all patients with BAO, whereas in patients with anterior circulation occlusions the reasons were recanalization or improvement in 29 (36% of the exclusions), significant worsening with radiological signs of a severe lesion on CT scan in 38 (47.5%), development of a cerebral hemorrhage after IVT in 2 (2.5%), advanced age in 3 (4%), and other not specified in 9 (10%).
The final sample for analysis consisted of 479 patients (52 (11%) BAO and 427 (89%) anterior circulation occlusions): 100 (21%) intracranial ICA/T or L occlusion, 244 (51%) M1, 40 (8%) M2, and 43 (9%) tandem occlusion (cervical ICA+M1 or M2 occlusion). There were 18 patients (4%) lost to follow-up at 3 months, all in the anterior circulation occlusion group.
Demographics, risk factors, and baseline characteristics of patients segregated with respect to the arterial territory occluded (BAO vs anterior circulation occlusions) are shown in table 1.
Demographics, risk factors, baseline characteristics, etiology, treatments applied, and duration of endovascular procedures in basilar artery occlusion compared with anterior circulation occlusion strokes
Patients with BAO were younger and were more frequently men. The median baseline NIHSS score appeared to be lower among patients with BAO, but this observation might have been biased due to the high number of patients with BAO who were intubated on arrival (15%) and for whom the NIHSS score was not recorded. Patients with anterior circulation strokes showed a higher frequency of atrial fibrillation. A cardiac source of embolism (namely, atrial fibrillation) was the main etiology of stroke in both study groups, but it was more frequent in anterior circulation strokes. There were no other differences in the baseline characteristics or risk factors.
Onset to treatment times, whether IVT or MT, were longer among patients with BAO. This is probably related to a longer delay in arriving at the treating hospital and because a longer OTP time was initially allowed in our treatment protocol, given in-hospital delays (DTP) did not differ (table 1). In 99 patients (25%) with anterior circulation occlusions and in 17 (39%) with BAO, the endovascular procedure was initiated beyond 6 hours. Median (IQR) OTP in these patients was 500 (410–720) min in anterior circulation occlusions and 660 (495–955) min in BAO.
An endovascular procedure was not possible in nine cases (2%) of anterior circulation occlusions and in three (6%) of BAO (p=0.13) due to technical difficulties, mainly related to the vascular approach. A stent was placed in five (1.5%) middle cerebral arteries (M1 segment) and in five (10%) basilar arteries due to persistent stenosis or occlusion. Among these, one BAO and one M1 occlusion were due to atherosclerosis, one BAO and three M1 occlusions were embolisms of cardiac origin, and the rest were codified as undetermined etiology. Complete recanalization after stenting was achieved only in two BAO and three M1 occlusions.
The duration of endovascular procedures was longer in BAO, indicating a more laborious and time-consuming endovascular approach to BAO. Median (IQR) duration of the procedure was longer in cases of stent placement (140 (135–325) min vs 66 (40–119) min, p=0.005 in BAO; 110 (90–148) min vs 60 (39–90) min, p=0.07 in anterior circulation strokes). Procedures were shorter in cardioembolism than in atherosclerotic disease (67 (40–105) min vs 130 (105–140) min, p=0.055 in BAO; 55 (35–76) min vs 75 (55–110) min, p<0.001 in anterior circulation occlusions). Also, complete recanalization was more frequently achieved in patients with cardioembolic stroke (87% vs 77%, p=0.048).
A trend toward a higher frequency of complications associated with the procedures, mainly vasospasm and arterial perforation, was seen in BAO (table 2). None of the complications related to procedures resulted in a worsening of the clinical condition or in death. The need for stenting was not associated with a higher rate of complications except for the development of groin hematoma which occurred in 2 (18%) versus 11 (2%) cases (p=0.033), all in patients with anterior circulation occlusions. There was no difference in the rate of complications depending on stroke etiology.
Complications related to procedures and outcomes in basilar artery occlusion and anterior circulation occlusion strokes
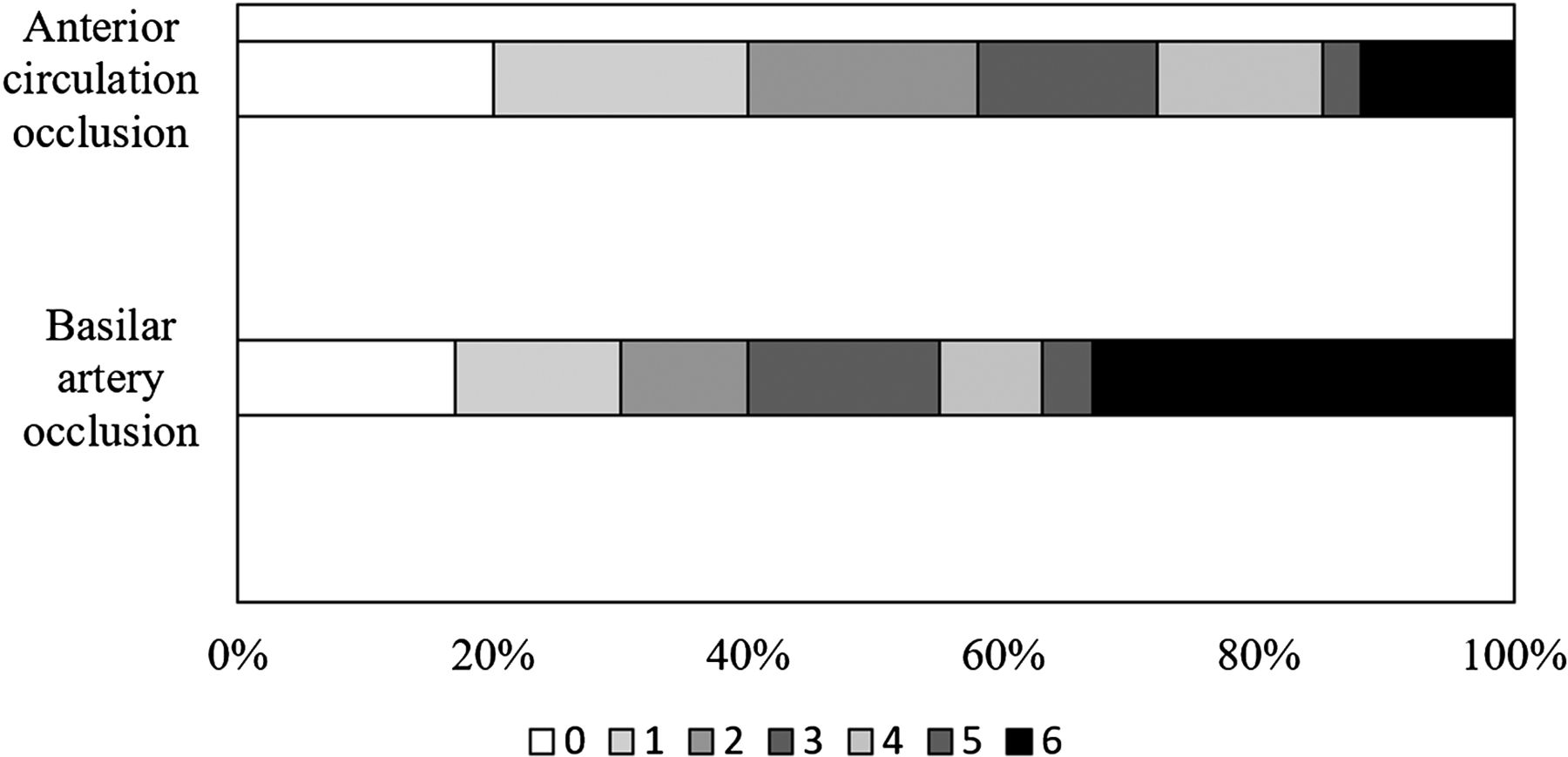
A comparison of recanalization rates and outcomes between patients with BAO and anterior circulation occlusion strokes is shown in table 2. There was a trend toward higher recanalization rates after MT in anterior circulation occlusions and the time from symptom OTR was shorter compared with BAO. This difference reflects the longer delay from OTP and the higher complexity of the procedures, including the need for stenting, in those with BAO. Early clinical outcomes were similar in both groups, but mortality was higher and the independence rate lower in patients with BAO. The shift analysis of the mRS score showed better outcomes for patients with anterior circulation occlusions (p=0.012; figure 1).

{kind=link}
Modified Rankin Scale (mRS) scores at 3 months in patients with basilar artery occlusions (BAO) and those with anterior circulation occlusion stroke. There was a significant shift in the distribution of the mRS toward a poorer outcome in BAO.
Comparisons of outcomes between BAO and anterior circulation occlusion strokes were made in the group of patients treated within 6 hours from symptom onset. Also, among these patients, those with BAO had worse outcomes, with a lower rate of independence (41% vs 61%, p=0.04) and higher mortality (33% vs 12%, p=0.002). However, outcomes did not differ between patients with BAO treated before and after 6 hours. The rate of independence was 41% in both groups while mortality was 29% vs 33% (p=0.79).
Confirmed recanalization improved the likelihood of a good outcome in both groups. More patients with effective recanalization achieved independence (mRS 0–2) in BAO (21/42 (50%) vs 2/13 (15%), p=0.027) and in anterior circulation occlusion strokes (224/343 (65%) vs 14/67 (21%), p<0.001). The OR (95% CI) for independence in patients with confirmed vessel recanalization was 5.5 (1.08 to 27.89) versus 7.12 (3.79 to 13.37). Mortality was also reduced if recanalization was achieved; however, in our series the reduction was not significant in the BAO group (12/42 (29%) vs 6/13 (46%), p=0.23) whereas in the anterior circulation stroke group it was 32/345 (9%) vs 16/67 (24%), p=0.001 (OR (95% CI) 0.46 (0.13 to 1.68) vs 0.33 (0.17 to 0.64)).
Futile recanalization was more frequent in patients with BAO (50% vs 35%, p=0.05), which might explain the poorer outcomes among this group. The multivariate analysis to define factors associated with futile recanalization in patients treated with MT segregated with respect to occlusion site is shown in table 3.
Univariate and multivariate logistic regression analysis of predictive factors of futile recanalization
Greater age, higher baseline NIHSS score, a longer duration of procedures and a longer delay to recanalization were associated with increased odds of futile recanalization in patients with anterior circulation stroke. In patients with BAO, however, only age and procedure duration remained significant prognostic factors for futile recanalization after adjusting for confounders.
Discussion
The analysis of this prospective registry from the Madrid Stroke Network shows that patients with BAO treated with MT according to the protocols in current clinical recommendations for management of LVO in anterior circulation12 ,13 have a lower recanalization rate and lower odds for a good outcome. The symptomatic intracranial hemorrhage rate did not differ between groups. MT appears to be more laborious and time consuming for BAO than for anterior circulation occlusions, with a tendency toward a higher frequency of complications associated with the procedures. These difficulties, together with a longer time from onset to initiation of treatments among patients with BAO, might explain the greater delays to recanalization in our series.
In accordance with previous data,3 ,4 ,6 our study suggests a higher rate of futility of MT in BAO compared with anterior circulation occlusions. Despite the higher rate of futility in patients with BAO, achievement of recanalization after treatment in our series was associated with a higher probability of a good outcome. Given the higher recanalization rate provided by MT, which has also been shown in previous publications,1 ,3 our study supports the recommendation to treat patients with BAO with MT using stent retrievers as an adjunct to standard treatment.
Recognition of factors associated with futile recanalization in BAO strokes might help increase the efficacy of MT in these patients. Factors such as clinical severity on admission, the need for mechanical ventilation, poor collateral status, a history of atrial fibrillation or previous stroke, and an extensive lesion on baseline MRI or CT have been identified as prognostic factors in BAO strokes and predictors of futile recanalization after MT in previous studies,3 ,4 ,6 although some cases of reversal of diffusion-weighted imaging lesions and favorable outcomes after MT have been described.21 Patients with an extensive lesion on baseline neuroimaging were excluded from treatment in our series and we did not record collateral status in posterior strokes. The variables included in the predictive models of futile recanalization in our study were those with known prognostic value and those that were significant in the univariate comparisons so that we could identify potential reasons for poorer outcomes despite recanalization with BAO. The need for intracranial stent placement was not included in the analysis as an independent variable because it was related to longer duration of procedures. A previous history of atrial fibrillation rather than any cardiac source of embolism was included in the multivariate analysis, since atrial fibrillation is a recognized prognostic factor and was the main cause of embolic heart disease among patients in the study. Severity on admission according to NIHSS score, greater age, a longer time to reperfusion and a longer procedure duration were associated with futile recanalization in anterior circulation occlusion strokes. Only age and procedure duration remained as independent predictors of futile recanalization in BAO.
We did not find a relationship between the onset to reperfusion time and the odds of futile recanalization; this might be explained by the fact that most patients were treated within 6 hours from symptom onset, which is rather short compared with other studies on MT in posterior circulation strokes. Previous data on the association of time to recanalization with outcome are heterogeneous. Although BASICS showed a stepwise decrease of the likelihood of a good outcome with longer time from onset to treatment,5 other studies did not.6
We also found no relationship between clinical severity on admission and the risk of futile recanalization in BAO. Severity on admission is an important predictor of outcome and has been advocated as one of the primary factors associated with a poor outcome in patients with BAO. The fact that severity on admission did not predict futility of recanalization in our study should encourage the indication of MT for these patients, despite the severity of their clinical condition, if they meet the criteria for treatment and do not have any the exclusion criteria.
Our study has some limitations. First, it is an observational study in which there is no control group to compare the effectiveness of MT in terms of outcomes. Patients who were not treated with MT received standard treatment with IVT and were excluded from MT because they achieved recanalization or significant improvement. Second, the small number of patients might preclude the identification of prognostic factors associated with treatment.
Conclusions
Patients with BAO strokes benefit from recanalization when MT is performed according to current protocols in clinical recommendations for the management of LVO in the anterior circulation. Endovascular procedures appear to be more laborious and to have a higher rate of associated complications in BAO. The rate of futile recanalization is also higher, with age and the duration of the procedures being the primary associated factors. A refinement of procedures through technical improvements and skills training might help to optimize the results of MT in BAO. The safety and efficacy of MT in BAO will become clearer in the near future when the results of ongoing RCTs are known.
Acknowledgments
Editorial assistance was provided by Juliette Siegfried and her team at ServingMed.com.
References
Footnotes
Contributors All authors have made substantial contributions to the design of the work; acquisition, analysis, or interpretation of data; drafting the work or revising it critically for important intellectual content. All authors have approved the final version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MAdL: overall responsibility for the manuscript, study concept and design, data acquisition, statistical analyses and interpretation, drafting the manuscript, final critical review of the manuscript. MMK: data acquisition, drafting the manuscript. ÁX-C, AC-C, AG-P, PM-S, GZ-W, AdF, FD-O, GR-A, JV, JM, AG-N and ED-T: data acquisition, revision of the manuscript. AF-P, JLC, JCM, RF, EB-R, EF and BM: radiological data acquisition, revision of the manuscript. BF: overall responsibility for the manuscript, study concept and design, data acquisition, final critical review of the manuscript.
Competing interests None declared.
Ethics approval Ethics approval was obtained from the ethics committee of University Hospital La Paz.
Provenance and peer review Not commissioned; externally peer reviewed.