Article Text

Abstract
OBJECTIVE To determine the frequency, clinical features, and radiological and bone scintigraphic changes of spondylodiscitis in patients with SAPHO (synov-itis, acne, pustulosis, hyperostosis, and osteitis).
METHODS The study was retrospective. Data from patients with the diagnostic criteria of SAPHO syndrome were analysed for clinical features, biological data (HLA B antigen), and pelvic and spine x rays. Spine computed tomography (CT) or magnetic resonance imaging (MRI) were also examined in some cases.
RESULTS 25 patients with a diagnosis of SAPHO were seen since 1985. Eight had spondylodiscitis. These included five with palmoplantar pustulosis, one with pustular psoriasis, one with psoriasis vulgaris, and one with chronic recurrent multifocal osteomyelitis without skin disease. The skin lesion occurred before the spondylodiscitis in four cases. Chest wall involvement was observed in four cases and sacroiliac joint lesions only in the case with osteomyelitis. HLA B27 was always negative and HLA B8 was found in four cases. Radiological findings consisted of erosive or sclerosing remodelling of endplates with a narrowed disc space; a reduced height of the vertebral body was also observed in some cases. These spinal lesions occurred in the three vertebral segments. Multiple sites of spondylodiscitis in the same patient were common. Bone scan showed mildly increased uptake and CT and MRI were useful for detecting signs of infection such as abscess. Enhanced signals on T2 weighted sequence or after injection of gadolinium were often observed. Follow up study of most of these patients suggests that the prognosis of spondylodiscitis in the SAPHO syndrome is favourable.
CONCLUSIONS Despite few description in the literature, spondylodiscitis in the SAPHO syndrome is common (32% in this series). These radiological findings are similar to the discovertebral changes of spondylodiscitis in ankylosing spondylitis, thus giving support to the relations between SAPHO syndrome and spondyl-arthropathies. However, this does not mean that the pathogenic mechanisms are the same in these two conditions.
- spondylodiscitis
- SAPHO syndrome
- clinical features
Statistics from Altmetric.com
Palmoplantar pustulosis is associated with a wide variety of osteoarticular disorders, including inflammatory and pseudoinfectious osteitis with hyperostosis, mainly located to the anterior chest wall.1-4 Aseptic and pseudoinfectious lesions also involve the peripheral bones and joints.5-7 Furthermore, sacroiliitis and spine lesions are observed in palmoplantar pustulosis suggesting a link to the spondyl-arthropathies.1 ,5 ,6
Psoriasis and acne have also been reported to be associated with these different bone and joint lesions.8-10 Psoriasis can be pustular and difficult to distinguish from palmoplantar pustulosis.5 For some investigators, palmoplantar pustulosis and pustular psoriasis are the same skin disease, while for others they are two distinct entities.11 These bone associated lesions have also been described in psoriasis vulgaris9 and in chronic recurrent multifocal osteomyelitis, a condition without skin involvement most often observed in children.12
In the French literature, it has been proposed that the syndrome of synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) includes rheumatic disorders associated with acne, palmoplantar pustulosis, pustular psoriasis, sternocostoclavicular hyperostosis, and chronic recurrent multifocal osteomyelitis.5 ,6
Involvement of the axial skeleton in the SAPHO syndrome includes sacroiliitis and spinal abnormalities. Syndesmophytes, hyperostosis, and erosions of the vertebral bodies are commonly observed onx ray.1 ,6 Spondylodiscitis is more rarely described.
Our aim was to evaluate the frequency, radiological changes, and course of spondylodiscitis in our SAPHO patients.
Methods
PATIENTS
A retrospective study was conducted. All the inpatients seen in our department and satisfying the previously proposed diagnostic criteria for SAPHO syndrome13 were included: osteoarticular manifestations of acne (conglobata or fulminans), hidrosadenitis suppurativa, palmoplantar pustulosis, pustular psoriasis, hyperostosis (anterior chest wall, spine, pelvis and limb), or chronic recurrent multifocal osteomyelitis with or without skin disease. The diagnosis of palmoplantar pustulosis or psoriasis required clinical confirmation by a dermatologist but not always a skin biopsy. Exclusion criteria were septic spondylodiscitis with evidence of infection, infectious palmoplantar pustulosis, psoriatic arthritis, diffuse idiopathic skeletal hyperostosis, and fluoride or retinoid therapy. Psoriasis vulgaris, if associated with spondylodiscitis, was included in this study. Data for each patient were available on clinical features, including back pain, and the results of physical examination, including the Schober test, chest expansion, and cervical spine motion.
PROCEDURES
Radiological investigations
Pelvic and spine x rays were examined. Spondylodiscitis was defined by destructive or sclerotic changes—with or without reduction of height of the vertebral body—and a narrowed disc space. A 99mtechnetium bone scan was performed in each patient. A computed tomography (CT) scan or magnetic resonance imaging (MRI), or both, were performed in seven cases to provide better definition of the spinal lesions and to show the extent of the inflammatory process.
Laboratory assessment
Data from erythrocyte sedimentation rate (ESR), C reactive protein, white cell count, and HLA B antigen determination were studied. Blood and urine cultures, serological tests for infection (salmonella agglutination test; brucella agglutination or Rose Bengal test), and a tuberculin skin test were determined if the patient was febrile. Disc space and vertebral biopsies were performed for histological examination and for culture in three cases.
Results
CLINICAL FEATURES
Between 1985 and 1996, 25 inpatients with previously defined criteria for the diagnosis of SAPHO syndrome13 were seen in our department. Fifteen had proven palmoplantar pustulosis and six had pustular psoriasis. One patient had acne conglobata, one chronic recurrent multifocal osteomyelitis, and one sternocostoclavicular hyperostosis without skin disease. One patient with psoriasis vulgaris was also included in this study. Chest wall involvement was found in 18 cases (including 11 with sternoclavicular arthritis, six with manubrio-sternal arthritis, and three with sternocosto-clavicular hyperostosis), and 10 had peripheral joint or appendicular skeleton manifestations. Fourteen patients had lesions of the axial skeleton, including five with sacroiliitis, and there were eight patients with spondylodiscitis.
These eight patients (table 1) included six females and two males (mean age 49.6 years). Five had palmoplantar pustulosis (cases 1, 4, 5, 7, and 8), one had pustular psoriasis (case 2), one had psoriasis vulgaris (case 3), and one had no skin disease (case 6). In four cases, the dermatological lesions were observed before the bone involvement (mean 5.75 years) and in three cases, bone and skin lesions occurred simultaneously. Sacroiliac involvement was only observed in the patient with chronic recurrent multifocal osteomyelitis (case 6). Other joint and bone conditions consisted of knee arthritis in one patient (case 2), anterior chest wall involvement in four patients (cases 1, 2, 7, and 8: three with sternoclavicular arthritis and one with sternocostoclavicular hyperostosis), proximal interphalangeal joint arthritis in one patient (case 1), and tibial aseptic osteomyelitis in one patient (case 7) (proven by biopsy and negative bone culture). No familial history of inflammatory bowel disease or psoriasis was found. All these patients complained of backache, with fever occurring in only one patient (case 2, 37.8°C). A reduced spine range of movement at the level of spine involvement was observed for each patient with spondylodiscitis (table 1).
Clinical features and HLA B antigens
BIOLOGICAL DATA (table 1)
Each patient admitted for spondylodiscitis had a raised ESR (range 20 to 86 mm) or C reactive protein (10 to 85 mg litre-1; normal < 8). The white cell count was raised in one patient (case 2, 15 000 mm-3; polymorphonuclear leucocytes 70%). No HLA B27 was found; one patient was HLA B27 positive and four were HLA B8 positive. No infectious cause was found in the febrile patient (case 2): blood and urine cultures remained negative and infectious serologies were also negative. Cultures of the open discovertebral biopsies (performed in cases 4, 6, and 8) for aerobic and anaerobic organisms and tuberculosis were also negative.
RADIOLOGICAL FINDINGS (table 2)
Destructive and sclerotic changes of lumbar vertebral bodies without narrowing of disc spaces were observed in the patient with chronic recurrent multifocal osteomyelitis (case 6) and this corresponded more to a spondylitis than a spondylodiscitis (fig 1). The seven other patients presented one or more examples of spondylodiscitis on x ray (one patient in the cervical spine: case 3; five patients in the thoracic spine: cases 1, 2, 5, 7, and 8; and three patients in the lumbar spine: cases 2, 4, and 8), with narrowed disc space and erosive and sclerotic remodelling in the opposite regions of the vertebral bodies (fig 2). In two patients (cases 2 and 8), destruction of the entire vertebral junction (T9-T10 and T6-T7 respectively) was observed. No infectious lesion such as abscess was shown on radiographs, neither were syndesmophytes. Bridging osteophytes were noted in two patients (cases 1 and 5) and a large hyperostosis anteriorly and laterally to L3, L4, and L5 in one patient (case 6) (fig1).
Radiological, bone scintigraphic, tomographic, and MRI features
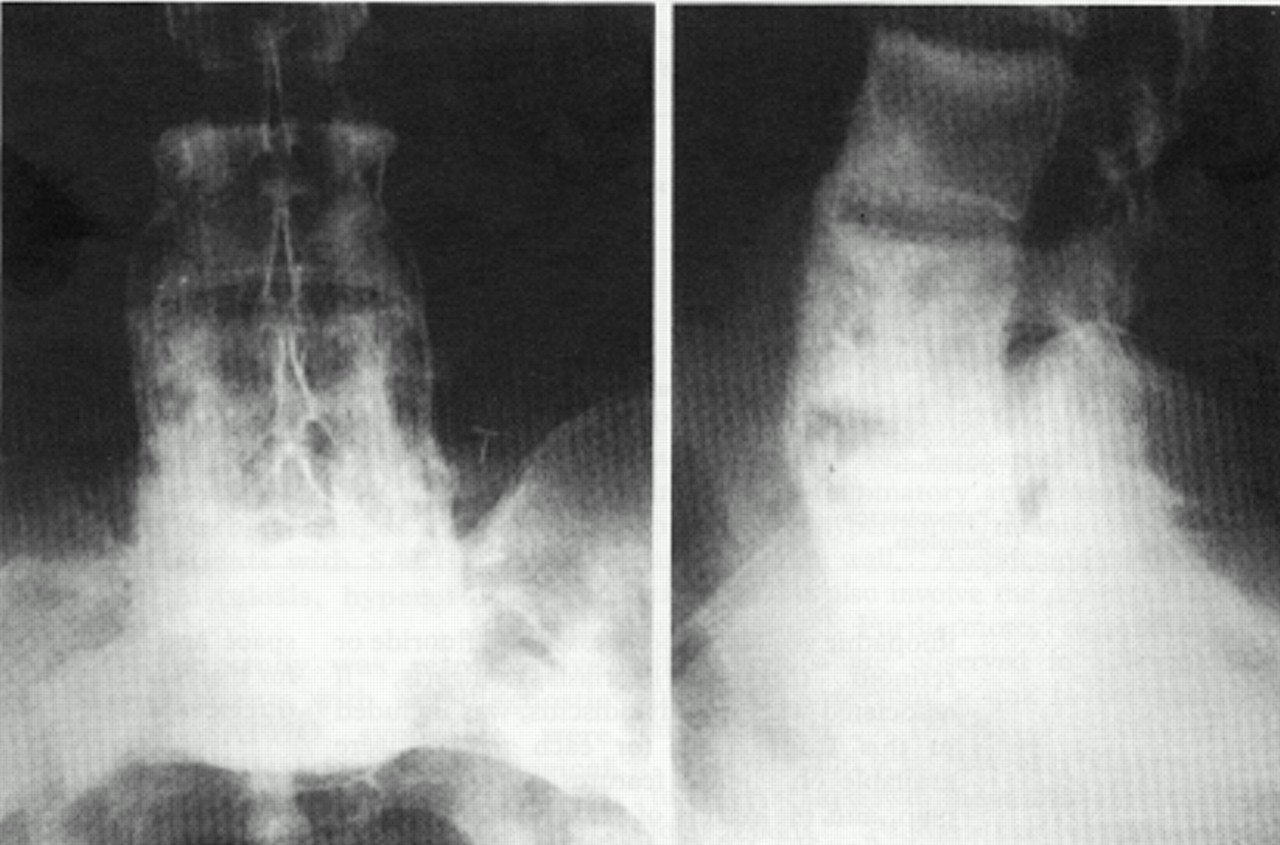
Case 6: frontal and lateral x ray views of lumbar spine: bony sclerosis and large hyperostosis extending from the anterior and lateral margins of L3, L4, and L5.

Case 5: lateral thoracic x ray: T8 and T9 erosive lesions, sclerotic remodelling of the endplates, and disc space narrowing.
BONE SCINTIGRAPHY (table 2)
Accumulation of radionuclide activity was noted in all the sites of spondylodiscitis. This was characterised by mildly increased uptake. However, in one case increased uptake revealed a new spine lesion which was not observed on x ray (case 7: T6-T7). Increased uptake was also observed at the right sacroiliac joint in case 6.
COMPUTED TOMOGRAPHY AND MAGNETIC RESONANCE IMAGING FINDINGS (table 2)
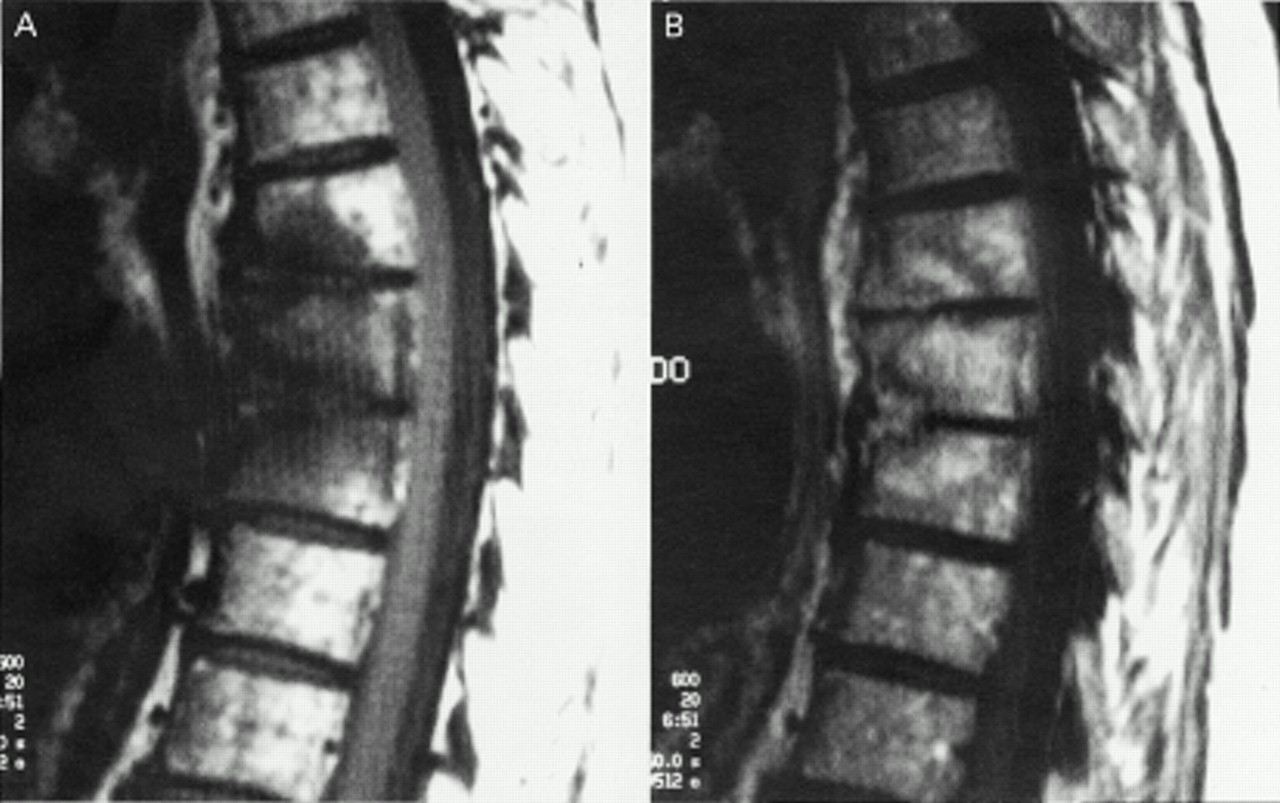
CT was performed in five patients and revealed erosive lesions in the vertebral bodies without spinal cord compression or abscess. MRI was performed at the onset of spondylodiscitis in two patients (cases 1 and 3) and showed a decreased signal intensity on T1 weighted sequence in thoracic vertebral bodies enhanced after injection of gadolinium (case 1), while the disc spaces showed no increased signal (fig 3A and B). In the case of the cervical spondylitis (case 3), similar signal abnormalities were observed in the cervical vertebral bodies. However, an intense signal was observed in the C6-C7 and C7-T1 disc spaces, corresponding to discitis associated with contiguous spondylitis (fig4A and B). No abscesses or epiduritis were seen.

Case 1: dorsal MRI. T1 weighted sequence without (A) and after injection (B) of gadolinium: decreased signal intensity in T6, T7, and T8 enhanced after injection of gadolinium. These signal abnormalities are mainly localised to the anterior portion of the discovertebral junction.

Case 3: cervical MRI. T1 (A) and T2 (B) weighted sequences: increased signal intensity in C5 and C6 vertebral bodies and considerable increased signal intensity in the C6-C7-T1 disc spaces in the T2 weighted sequence.
DISCOVERTEBRAL HISTOPATHOLOGICAL FINDINGS
Open biopsies of the disc or the vertebral body were performed in three patients (L4-L5 disc space: case 8; L4 and L5: cases 4 and 6). Neither specific lesion nor inflammatory cells were observed in the disc. Biopsy of L4 in patient 4 showed infiltration of lymphocytes and plasmacytes. Biopsy of L5 in patient 8 showed replacement of bone by fibrous tissue and the picture of chronic osteomyelitis with cellular infiltrate composed of lymphocytes and polymorphonuclear leucocytes. In some areas microabscesses were seen. Cultures of disc and bone tissue remained sterile.
FOLLOW UP STUDY
In all patients, back pain was treated with non-steroidal anti-inflammatory drugs. Seven patients (cases 1, 2, 3, 4, 6, 7, and 8) were seen again between one and eight years later. None had recurrence of backache. In two patients, spine x rays showed the same lesions as initially, with additional constructive bone lesions: osteophytes bridging the vertebral bodies (case 4) and hyperostosis bridging the lateral margin of L1 and L2 for patient 2 (fig 5); new cervical x rays were also available one year later in patient 3 and showed progression of spondylodiscitis to C5-C6 and a large hyperostosis anterior to C5, C6, C7, and T1 (fig 6). Two patients were seen five years after the onset (cases 4 and 8) and MRI showed erosive changes but no enhanced signal in the disc or the vertebral bodies on T2 weighted image. During this follow up period, we observed correction of the initially elevated inflammatory markers.

Case 2: frontal x ray view of the lumbar spine showing L1-L2 spondylodiscitis. Note the lateral hyperostosis bridging the vertebral bodies.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case 3: lateral cervical x ray showing cervical spondylitis located at C5-C6, C6-C7, and C7-T1, with narrowed disc spaces, bone sclerosis, and reduced height of the vertebral bodies. A large hyperostosis extends from anterior margin of the cervical vertebral bodies (arrow).
Discussion
The SAPHO syndrome was proposed to group together those rheumatic conditions closely associated with dermatological disorders, mainly palmoplantar pustulosis and pustular psoriasis.1 ,2 5 6 The interval between the appearance of these two conditions could be long.14 Evidence of similar bone and joint lesions in psoriasis vulgaris has also been reported.9 Thus we have also included in our series a patient with psoriasis vulgaris with vertebral lesions suggestive of spondylodiscitis.
Joint and bone involvement in the SAPHO syndrome is mainly located to the anterior chest wall and combines arthritis, aseptic oste-itis, and hyperostosis.1 ,3 ,4 ,6 ,14 The other sites of skeletal diseases in the SAPHO syndrome are peripheral as well as axial. Sacroiliitis is well described in 13-52% of cases.1 ,6Axial skeletal lesions consist of erosions, sclerotic changes, syndesmophytes, hyperostosis, and spondylodiscitis.
Published data give a frequency of 9-21.4% for the spondylodiscitis in the SAPHO syndrome1 6 15 16–17 (table 3). However, Le Loët et al 15 found no spondylodiscitis in their series of 15 cases. In a recent report by the same investigators,11 there is no comment about spondylodiscitis in 23 cases of SAPHO syndrome. Maugars et al 17 reported three cases of spondylodiscitis among 19 cases of the SAPHO syndrome (15.7%). In our own series, we found spondylodiscitis in 32%.
Frequency of spondylodiscitis in the SAPHO syndrome
These cases of spondylodiscitis are observed in the course of palmoplantar pustulosis and pustular psoriasis1 6 15–19; reports of spondylo-discitis with acne are exceptional.10 ,20 As with the other rheumatological disorders, the spondylodiscitis can occur before or after the skin disease. Most of our patients had skin lesions before the onset of spondylodiscitis. The main clinical feature is inflammatory back pain with no or mild fever. No neurological complications are described. Biological investigations show an inflammatory syndrome with mildly elevated or normal white cell count. There is no association with HLA B27 or other HLA antigen.1 ,6 However, in our series four patients were HLA B8 positive.
The radiological findings are a narrowed disc space, erosions, and sclerotic changes on the opposite region of the vertebral bodies.1 ,16 These defects are mainly localised to the central or anterior portions of the discovertebral junction. Isolated sclerotic lesions of the vertebral body are also seen20 and are generally associated with a reduced height of the vertebral body, corresponding more to a spondylitis than to a spondylodiscitis. In our series, the spondylodiscitis was observed at different spinal levels. Two or more foci of spondylodiscitis at separate sites or at the same spinal level can occur in the same patient. The spondylodiscitis is frequently associated with constructive bone lesions such as osteophytes or hyperostosis of the vertebral body. However, adjacent syndesmophytes are not described and sacroiliitis is generally not a feature. Patient 6 of our series (L3, L4, and L5 spondylitis) presented sclerotic remodelling and erosions of the right sacroiliac joint. The apophyseal joints were intact without destructive or constructive changes.
Data from bone scintigraphy, CT, and MRI are not available in published reports on the spondylodiscitis of the SAPHO syndrome. In our series we found the following:
A mild increased scintigraphic uptake in our eight patients. Of interest, areas of increased uptake may reveal an undepicted spinal lesion on x rays.
CT scans show the erosive lesions and support the likely inflammatory cause of the spondylodiscitis, as no abscesses are seen.
All the sites of spondylodiscitis are revealed by MRI, which shows enhanced signal in T2 weighted sequence (or after gadolinium injection) in the disc and vertebral bodies. Of interest in our series, some vertebrae without abnormalities on x rays or bone scintigraphy showed evidence of inflammatory involvement on MRI. Abscesses and epiduritis are also not seen on MRI. Thus MRI is useful and should be performed in cases of spondylodiscitis in the SAPHO syndrome to provide better definition of the extent of the inflammatory process.
Histopathological examination in three cases in our study showed inflammatory changes in the vertebral body but not in the disc space. This suggests that the inflammatory process starts in bone tissue and then progresses to the disc. Furthermore, these lesions are similar to those observed in ankylosing spondylitis.21
The course of the spondylodiscitis is favourable. The patients present with back pain at onset and for many weeks, but they become progressively asymptomatic. No complications (such as neurological disturbances) are described, and recurrence at the same spinal level is not mentioned in published reports. However, total destruction of the disc space can induce vertebral kyphosis (as was observed in case 8 of our series). We observed no complications, recurrences, or new localisation of spondylodiscitis in the majority of our patients. MRI, performed five years after the initial back pain in patients 4 and 8, shows no inflammatory changes but only sequelae of the spondylodiscitis. Conversely, constructive bone lesions such as osteophytes or hyperostosis may develop and bridge the vertebral bodies.
In patient 3, we observed cervical spondylitis in association with psoriasis vulgaris. Psoriasis vulgaris can be associated with the same bone and joint lesions as palmoplantar pustulosis and the pustular form of psoriasis. However, we have excluded from our study the patient diagnosed as having psoriatic arthritis. Axial involvement is well known in psoriatic arthritis.22 However, spondylodiscitis is estimated to occur in 22% of cases of psoriatic arthritis,23 though in association with other lesions such as syndesmophytes, ligamentous ossification, apophyseal joint narrowing or fusion, and subluxation at the cervical level.
Another differential diagnosis is infectious spondylodiscitis. The radiological findings are the same in inflammatory and infectious spondylodiscitis. No abscesses or epiduritis are observed in the SAPHO syndrome; conversely, multiple foci of spondylodiscitis are uncommon in infection. Furthermore, the constructive changes occur earlier in SAPHO than in infectious spondylodiscitis. While open vertebral biopsy has sometimes been required in the past to rule out infection, such biopsies could certainly now be avoided with the advent of MRI, which shows changes diagnostic of an inflammatory process.
Finally, the spondylodiscitis observed in the SAPHO syndrome and ankylosing spondylitis have clinical and radiological similarities and this supports the relation between SAPHO syndrome and spondylarthropathies. Disco-vertebral erosions and destructive changes are indeed well known in ankylosing spondylitis21 24 and occur in 1-10% of cases. These findings result from inflammatory lesions, discal herniation, and fractures and occur in early or late phases of the disease. Some investigators emphasise the inflammatory aetiology.21 However, severe discovertebral lesions are relatively uncommon in ankylosing spondylitis and are mainly located in the thoracic and lumbar segments of the spine, while other changes such as syndesmophytes, Romanus osteitis, osteoporosis, apophyseal joint sclerosis, and sacroiliitis are associated with the spondylo-discitis of ankylosing spondylitis. In addition, the similar clinical and radiological features of spondylodiscitis in SAPHO syndrome and ankylosing spondylitis do not mean that these two conditions have the same pathogenic mechanisms. In fact, HLA B27 is expressed less often in the SAPHO syndrome than in ankylosing spondylitis, and hypothetical infectious agents involved in SAPHO syndrome (Proprionibacterium acnes)4 5 are not the same than those in ankylosing spondylitis (Klebsiella pneumoniae).