Article Text

Abstract
Hypoxic–ischaemic brain injury is common and usually due to cardiac arrest or profound hypotension. The clinical pattern and outcome depend on the severity of the initial insult, the effectiveness of immediate resuscitation and transfer, and the post-resuscitation management on the intensive care unit. Clinical assessment is difficult and so often these days compromised by sedation, neuromuscular blockade, ventilation, hypothermia and inotropic management. Investigations can add valuable information, in particular brain MRI shows characteristic patterns depending on the severity of the injury and the timing of imaging. EEG patterns may also suggest the possibility of a good outcome. There is no entirely reliable algorithm of clinical signs or investigations which allow a definitive prognosis but the combination of careful repeated observations and appropriate ancillary investigations allows the neurologist to give an informed and accurate opinion of the likely outcome, and to advise on management. Overall, the prognosis is extremely poor and only a quarter of patients survive to hospital discharge, and often even then with severe neurological or cognitive deficits.
Statistics from Altmetric.com
Introduction
Neurologists are frequently asked to assess patients on intensive care units (ICUs) who have sustained hypoxic–ischaemic brain injury as a consequence of cardiac arrest or hypoxia during surgery or critical illness. Intensivists expect not only a prognosis for meaningful functional recovery but also guidance on management and, often, a contribution to communication with relatives. Although the assessment remains primarily clinical, it also requires the use of ancillary investigation. But, even so, it remains beset by the limitations in the sensitivity and specificity of both the clinical and investigational tests, which is made even more difficult by the use of ever more sophisticated techniques of sedation, ventilation, hypothermia, neuromuscular blockade and haemodynamic management. This means that the traditional clinical indicators of prognosis, including brainstem reflexes and limb responses to noxious stimuli, are of less value than they once were.

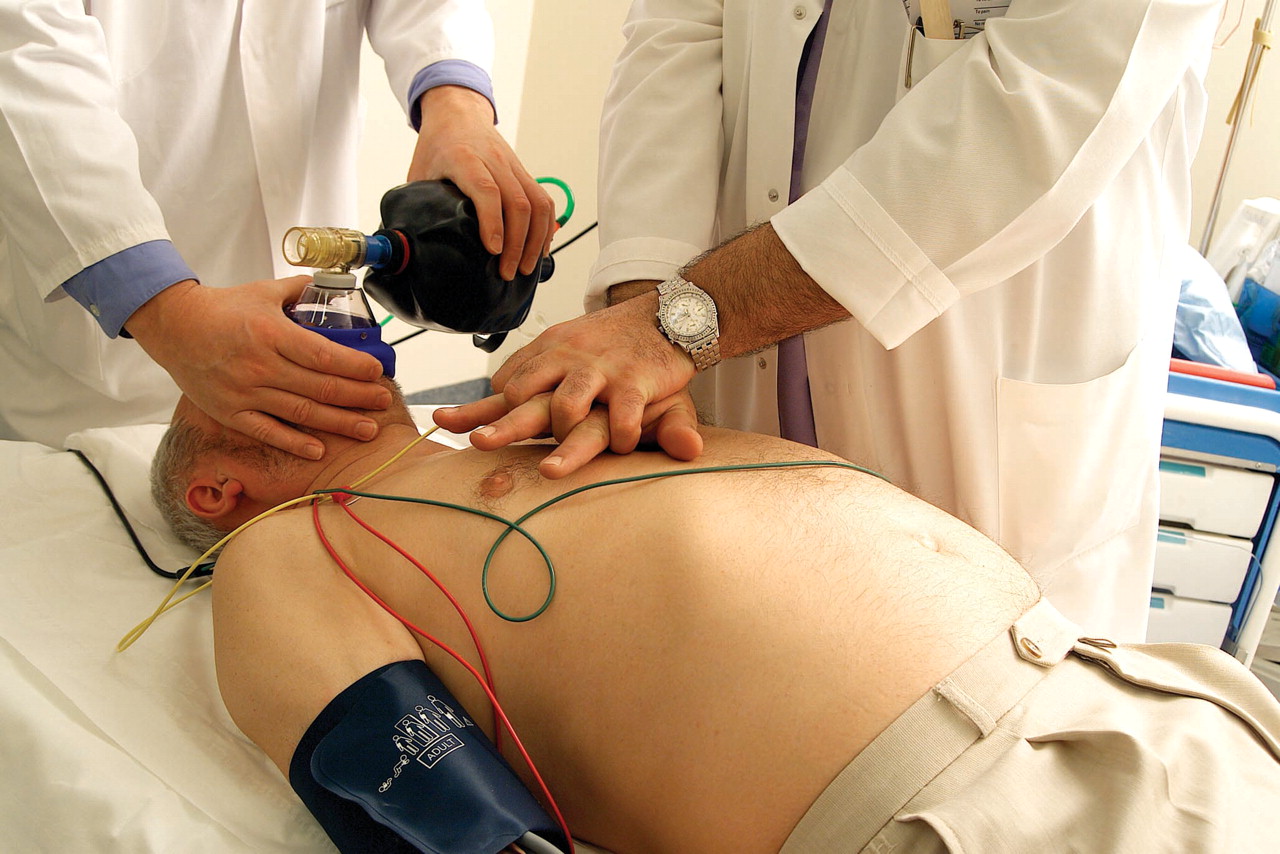
Resuscitation. Doctors performing cardiopulmonary resuscitation (CPR) on an unconscious man, following a cardiac arrest. The doctor on the right is giving heart massage (cardiac compression). Each downward compression on the chest squeezes blood out of the heart and around the body. The other doctor is using an Ambu bag to push air into the patient's lungs, maintaining oxygenation of the blood and stimulating natural breathing.
Credit: AJ PHOTO / SCIENCE PHOTO LIBRARY
The cost of inpatient care for hypoxic–ischaemic brain injury is enormous, both in the ICU and afterwards for survivors. There is therefore an urgent need for improved ways of reliably assessing prognosis in the early stages of ICU care and identifying those patients with a potentially favourable outcome and those where further efforts would be fruitless.1 The outlook for meaningful recovery of function is poor despite recent developments in resuscitation and intensive care. For example, of patients who have an in-hospital arrest, less than 40% even achieve successful restoration of spontaneous circulation, and <30% of patients admitted to the ICU survive to hospital discharge.2 The cause of death is neurological injury in two-thirds of patients and cardiac or multiorgan failure in one-third.3 But some survivors can do surprisingly well, many leaving hospital after ventricular fibrillation arrest with no or minimal cognitive impairment.4 5
Pathophysiology
Brain injury can occur as a consequence of a reduction in either cerebral blood flow (CBF) or oxygen supply, or both, which can follow cardiac arrest or other acute events which cause severe cardiopulmonary compromise. Although ischaemia and hypoxia cause pathologically and clinically distinct patterns of brain injury they usually coexist.
Although ischaemia and hypoxia cause pathologically and clinically distinct patterns of brain injury they usually coexist
Ischaemia describes a reduction in blood supply leading to decreased oxygen delivery but, unlike hypoxia alone, there is also limited or no removal of damaging cellular metabolites (eg, lactate, H+, glutamate) which contributes to severe brain injury.
Hypoxia refers to a reduction of either oxygen supply or utilisation. It may develop as a direct consequence of reduced oxygen supply, reduced ambient oxygen pO2, low haemoglobin or impaired tissue utilisation following poisoning of the mitochondrial cytochrome enzymes (eg, due to cyanide). Following isolated hypoxia there is an increase in CBF which allows continuing delivery of glucose to, and clearance of toxic metabolites from the brain. Therefore, hypoxia in isolation, even if prolonged, does not necessarily cause severe brain injury, provided the systemic circulation is preserved.
Causes of hypoxic–ischaemic brain injury
Cardiac arrest is the commonest cause of hypoxic–ischaemic brain injury, usually due to arrhythmias, but it may also follow respiratory arrest or hypotension due to shock or hypovolaemia (table 1). The initial arrhythmia is ventricular tachycardia or ventricular fibrillation in approximately 50% and asystole or pulseless electrical activity in the remainder. However, the longer the rescue time the more risk of asystole.
Causes of hypoxic–ischaemic brain injury
Traditional clinical indicators of prognosis, including brainstem reflexes and limb responses to noxious stimuli, are of less value than they once were.
Isolated hypoxic brain injury is usually caused by asphyxia (table 2). However, in all of these situations ischaemia or hypoperfusion may coexist due to constriction of the carotid vasculature or secondary myocardial depression. It is therefore difficult to characterise the neurological deficit which results from isolated hypoxic brain injury.
Causes of hypoxic brain injury
Cardiac arrest
Cardiac arrest is usually due to arrhythmias but may follow respiratory arrest or hypotension due to shock or hypovolaemia. The long term outcome depends critically on the cause of the arrest and the peri-arrest management. The most important prognostic factors6 7 are listed in table 3.
Factors affecting the prognosis following cardiac arrest
Intensive care management following cardiac arrest or profound hypotension
After successful resuscitation there is a brief period of brain hyperaemia followed by reduced CBF (no-reflow)8 9 as a result of microvascular thrombotic occlusion leading, inter alia, to failure of autoregulation. It is therefore important to maintain a relatively high mean arterial blood pressure (80–100 mm Hg) with crystalloid infusion or vasopressor agents.
Severe cerebral oedema is rare following hypoxic–ischaemic brain injury but, when present, raised intracranial pressure (ICP) will further compromise CBF and may provoke herniation. ICP should be maintained below 20 mm Hg and, if raised ICP is suspected clinically, treatment is with head positioning up, osmotherapy (mannitol, hypertonic saline), controlled hyperventilation and metabolic control (ie, treatment of fever, shivering, seizures, hypoglycaemia and hypokalaemia). There is no evidence to justify the use of direct ICP measurement.
Following successful resuscitation and transfer, the initial aims of management are to establish haemodynamic stability, and adequate tissue oxygenation, and to prevent secondary cerebral damage due to hypotension.
Intubation will usually have been undertaken and ventilation established by the time of admission for out of hospital incidents.
Sedation (eg, midazolam, fentanyl) will reduce the stress of procedures and facilitate ventilation; neuromuscular blockade is occasionally necessary, particularly if therapeutic hypothermia is used.
Blood sugar control is controversial (hypoglycaemia may reduce CBF); it is reasonable to aim for normoglycaemia.10
Fever and seizures, both of which increase metabolic demand on the brain, should be treated aggressively.
Neuroprotective agents have not been shown to be valuable.
After restoration of spontaneous circulation, systemic coagulopathy can occur, commonly due to an increase in cytokines without adequate activation of endogenous fibrinolysis. Aspirin should, therefore, be given on admission.
Induced hypothermia
A surprisingly good outcome can follow prolonged cardiac arrest in hypothermic conditions (eg, drowning, severe hypothyroidism and survival in extremely cold climates). This observation led to the use of induced controlled hypothermia following cardiac arrest associated with ventricular fibrillation. Hypothermia causes a decrease in CBF and a consequent reduction of cerebral metabolism. A meta-analysis of randomised trials has shown that treated patients are more likely to be discharged with no or minimal neurological damage (relative risk 1.68) which translates into a number needed to treat of six patients.11 However, hypothermia can be difficult to apply and uncomfortable, patients require sedation and a neuromuscular blocking agent (vecuronium or pancuronium) to prevent shivering, and so the technique is restricted to patients in coma. Complications include cardiac arrhythmias which develop if temperature is <32°C, sepsis (particularly pneumonia), hypotension during rewarming, coagulopathy due to thrombocythaemia, thrombocytopenia, renal failure, hypokalaemia and pancreatitis.12
Outcome
The clinical effects—and consequences—of hypoxic–ischaemic brain injury are highly variable. The best outcome is generally seen in patients who have had only a short period of impaired consciousness following resuscitation. Regaining purposeful motor movements and awareness with preserved memory within a few hours is usually associated with a good recovery and functional independence. However, the literature on prognostic factors and outcome is difficult to apply these days because it is largely based on studies before the modern techniques of post-resuscitation support, including the early use of sedation and ventilation, which now prevent a full assessment of conscious level and more or less any informative neurological examination in the immediate post-arrest period.
Several factors are important prognostic findings, particularly in patients who have not received significant sedation The outcome of hypoxic–ischaemic brain injury worsens if:
The patient has been in coma (ie, unresponsive) for >6 h.
There are no spontaneous limb movements or localisation to painful stimuli in the initial stages.
There is prolonged loss of pupillary responses (provided atropine has not been administered).
There is sustained conjugate eye deviation (upgaze or downgaze).
There are specific forms of abnormal eye movements (eg, upbeat and downbeat nystagmus, ping pong gaze or period alternating nystagmus).
There are myoclonic seizures.
Lower cranial nerve function is involved (eg, absent cough and gag reflexes).
However, it must be emphasised that these days the early assessment of the post-resuscitation state is unreliable for the reasons discussed above and fraught with confounding factors that prevent the clinician being able to present a clear prognosis for outcome.
The assessment of coma has been reviewed in detail elsewhere. The conventional method used over many years has been the Glasgow Coma Score. This has proved valuable, robust and reproducible but it was designed to monitor patients with head injury and is not thorough or detailed enough to permit accurate assessment of medical causes of coma. Widjicks has introduced a wider ranging scale which corrects many of the omissions of the Glasgow Coma Score and may prove more sensitive and specific for recognising change in the conscious state of patients in coma due to hypoxic–ischaemic brain injury (the full outline of unresponsiveness (FOUR) score)13 (table 4).
FOUR score (Full Outline of UnResponsiveness)
Prognostic models to predict outcome
Various prognostic models based on clinical findings have been widely quoted, but not widely used, over many years.14,–,19 None has adequate sensitivity or specificity to be of value in determining management and, in particular, to guide when to abandon efforts to continue support in the hope of eventual improvement. Most clinical algorithms depend on brainstem reflexes (particularly the absence of pupillary light, corneal and oculocephalic reflexes), spontaneous eye movements and motor responses (spontaneous and evoked to painful stimuli) but each one of these has limitations in patients who are sedated.
Focal or generalised convulsive tonic–clonic seizures are relatively unusual in the initial stages
More accurate predictive models, which include neurophysiological observations, have been proposed but these are difficult to construct because large numbers of patients must be included in any prospective study, and of course any prognostic model must be validated in an independent data set. These models may also be influenced by the use of early sedation.
In summary, a poor prognosis is likely, in the absence of sedating medication, which these days is unusual, if the corneal and pupillary light reflexes and motor responses are absent at 24 h and 72 h.
Epileptic seizures
Focal or generalised convulsive tonic–clonic seizures are relatively unusual in the initial stages following hypoxic–ischaemic brain injury, but they may appear during the recovery period. Their occurrence implies severe but incomplete damage to the cortical and subcortical structures. Prolonged generalised seizure activity may not always be apparent in coma because of limited facial, limb or trunk movements due to sedation or damage to the motor pathways. Moreover, ictal movements may be restricted to blinking, fixed or varying eye deviations, or small repetitive facial or limb movements which are easily overlooked. Even non-convulsive status epilepticus may be missed for similar reasons. Generalised repetitive trunk and limb movements are not always ictal and may be due to brain stem ‘shivering’ or the effects of medication.
Spontaneous, unrelenting generalised multifocal myoclonus (post-hypoxic myoclonic status) may develop immediately after resuscitation when it typically causes bilateral synchronous local or generalised jerking of the face, limbs, trunk or diaphragm. The EEG shows limited background activity with a burst suppression pattern and intermittent generalised periodic complexes with no cortical focus. It responds poorly to medication and carries a uniformly poor prognosis.20
Another form of myoclonus (Lance–Adams syndrome) can start 24–48 h after resuscitation. It often follows a primary respiratory arrest or anaesthetic event and tends to occur at a younger age than post-hypoxic myoclonic status. Consciousness is usually less deeply impaired, and focal myoclonus is often action or startle sensitive. The prognosis is generally favourable and these patients continue to improve over time although cerebellar signs including ataxia, dysarthria and intention tremor may persist.21 The EEG shows a focal cortical origin with responsive cortical rhythms which progressively regain normal patterns. It responds reasonably well to antiepileptic drugs including valproate, piracetam, levetiracetam and clonazepam.22
Investigations
EEG
The EEG has been widely used over many years to assess the level of consciousness and to guide prognosis after hypoxic–ischaemic brain injury.23,–,26 However, the appearances are influenced by confounding factors, including medication, metabolic derangements and sepsis that bear upon the level of arousal, duration of coma and interval between resuscitation and EEG recording. In the initial stages following resuscitation there may be electrical silence but distinct rhythms may gradually evolve which guide prognosis.
Several systems of classification of the EEG in coma have been proposed but none can predict outcome with complete reliability. Reactivity of the EEG to external stimuli is more important than the dominant frequency alone; the presence of reactivity indicates a better prognosis (figure 1). A number of patterns suggest a poor prognosis including26:
Generalised electrical suppression; electrocerebral silence or generalised voltage suppression below 10 µV for >24 h in normothermic patients who are free of toxic ingestion or pharmacological sedation is the only reliable indicator that there is no chance of meaningful recovery.
Generalised burst suppression (figure 2) in a non-sedated patient indicates severe injury of the thalamus, cortex or their connections. It is associated with fatal outcome or vegetative state, particularly when bursts consist of epileptiform activity (recovery has been reported when the pattern is present early and transiently after resuscitation).
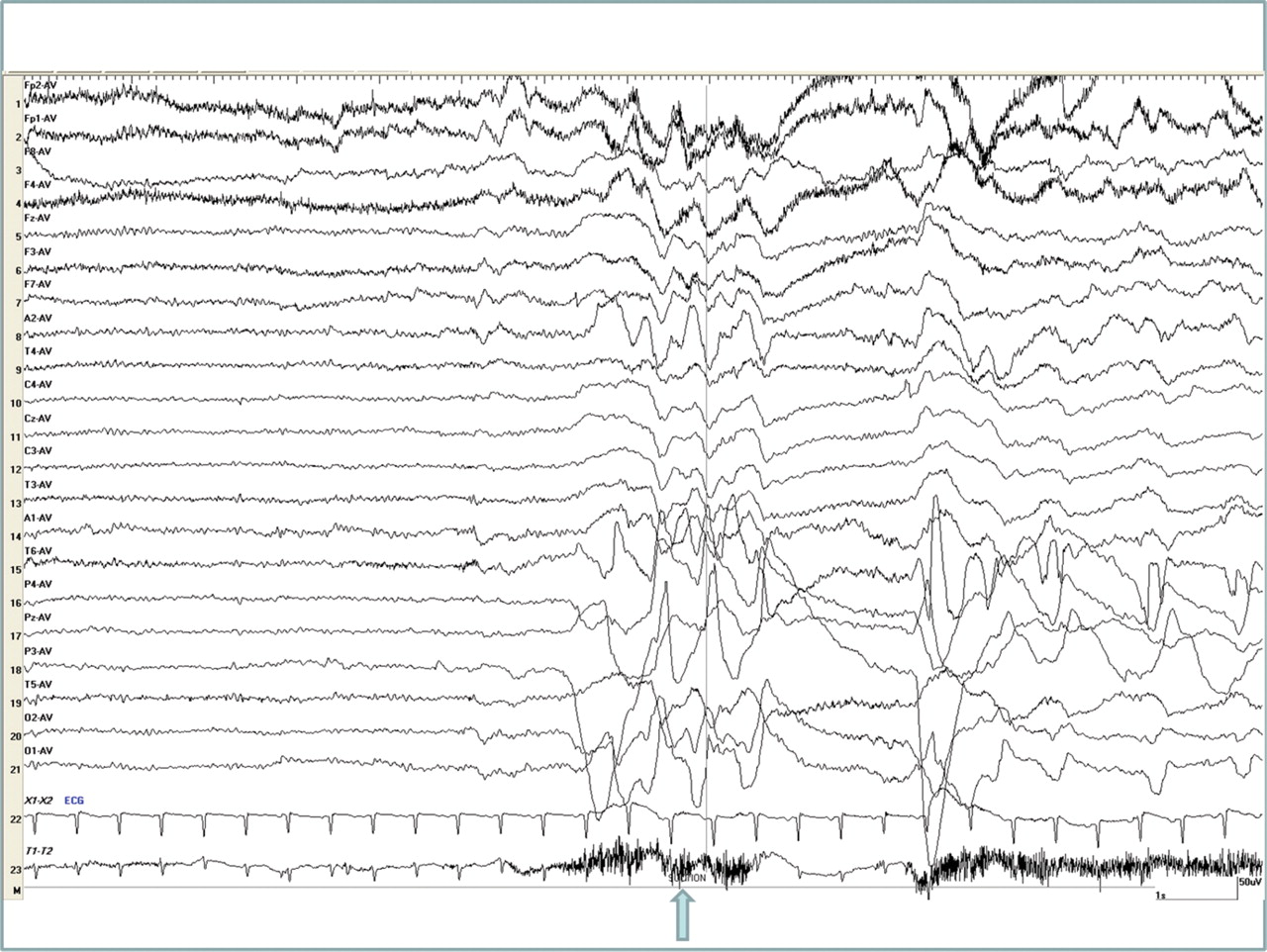
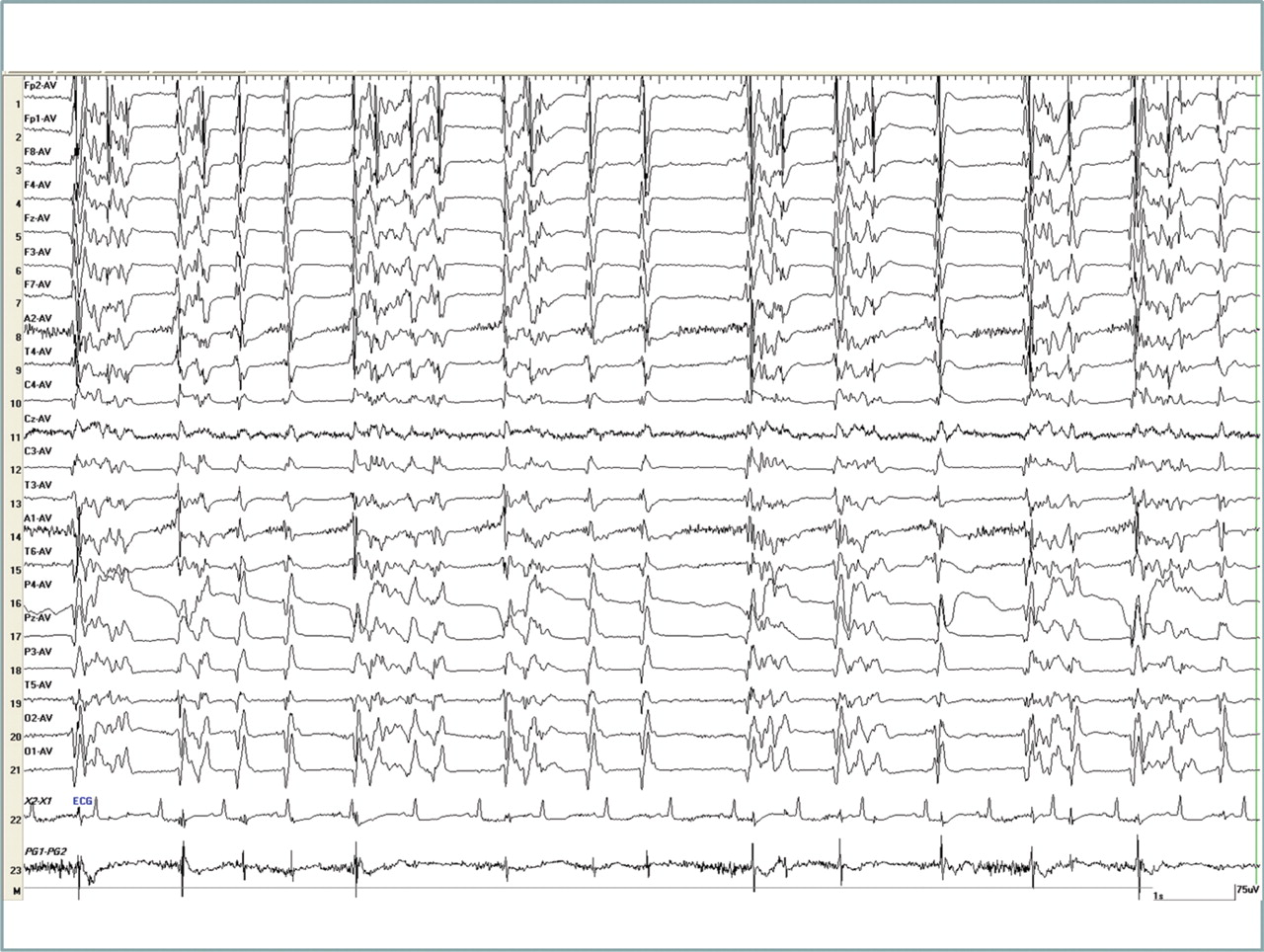
Post-anoxic status epilepticus, either myoclonic (figure 3) or non-convulsive, (associated with periodic lateralised or diffuse epileptiform discharges (PLEDs or Bi-PLEDs)) is considered a predictor of fatal outcome; occasionally, however, if EEG reactivity is preserved, such patients may have a favourable outcome with aggressive management.
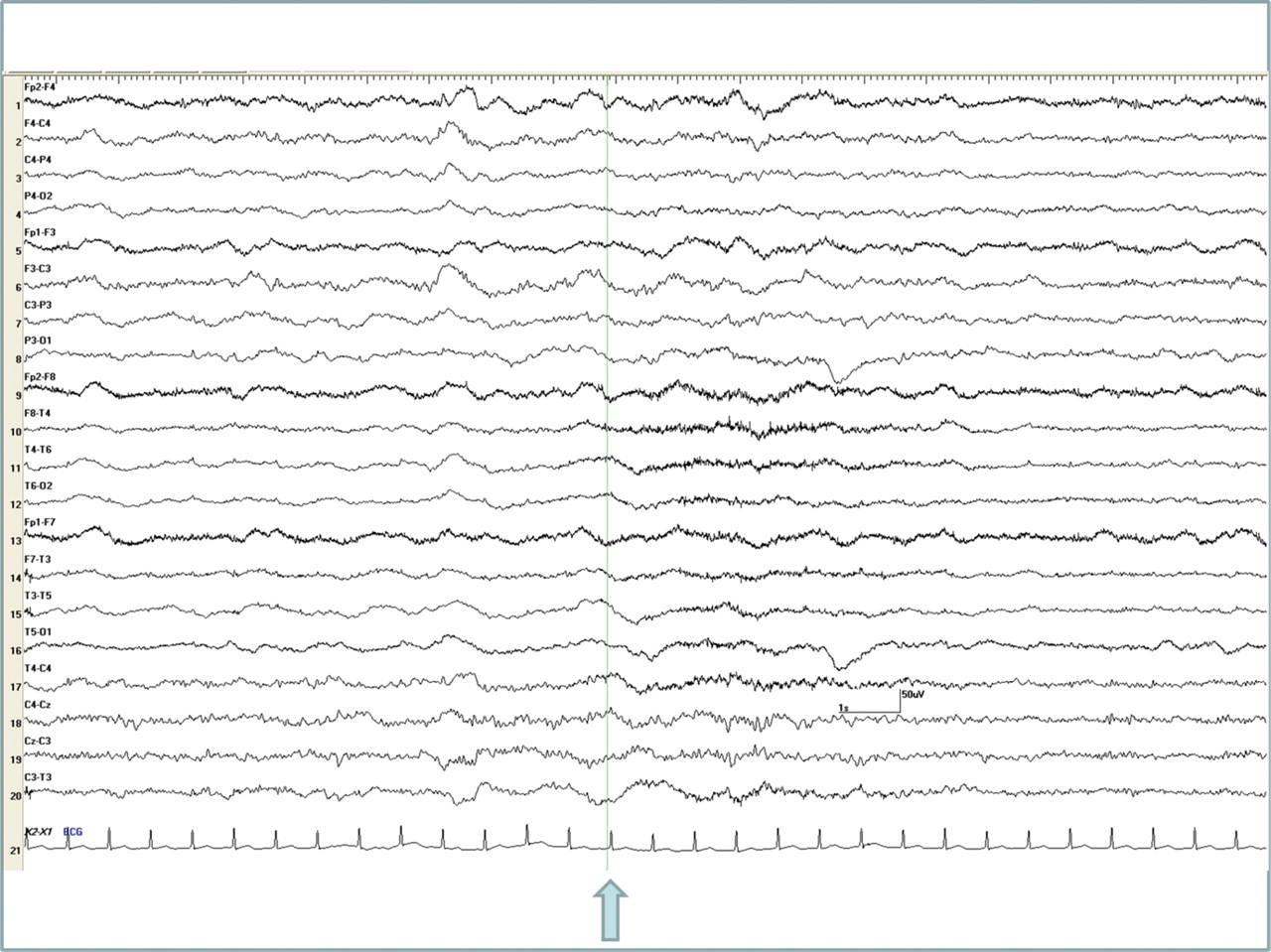
Complex partial seizures or non-convulsive complex partial status may also occur (figure 4), often without associated clinical manifestations. The prognosis depends on the extent of cortical involvement.
Alpha coma consists of diffuse or frontally predominant, unresponsive rhythms with fixed and unwavering alpha frequencies occasionally extending into the theta range (figure 5). It indicates a grave prognosis with about a 90% probability of death or vegetative state.

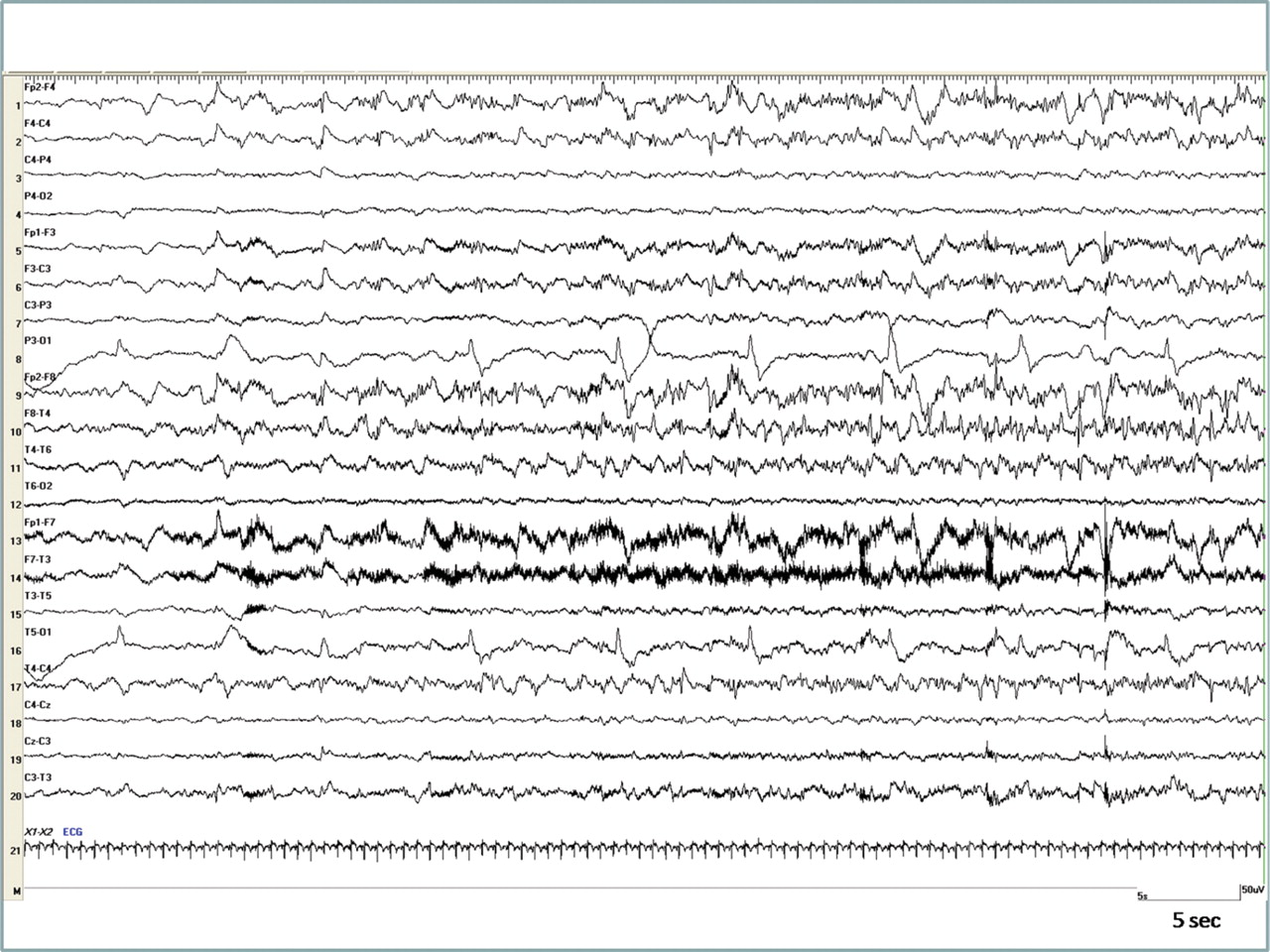
Responsive cortical rhythms in a 37-year-old man after cardiac arrest. He showed no overt response to auditory stimuli but grimaced in response to noxious stimuli. Background rhythms consisted of a mixture of slow and faster frequencies and he responded to noxious stimuli (arrow). Note that faster rhythms slightly enhance immediately after the stimulus and the underlying slow rhythms attenuate for a while (3–4 s later), suggesting a change of vigilance. The presence of faster frequencies with spontaneous fluctuation and reactivity to external stimuli are important predictive features. This patient was successfully discharged from hospital with minimal cognitive impairment.

Three days after cardiac arrest post-anoxic myoclonus associated with burst suppression pattern on video EEG. The patient had continuous twitching of his facial muscles and of his upper body and arms throughout this test. He died 2 days after the recording. Note the ongoing diffuse and bilaterally synchronous bursts of spikes/polyspikes and their association with the recorded myoclonus (bottom tracing); EEG discharges are separated by intervals of generalised attenuation of all activity lasting for 0.5–1 s with the pattern being non-reactive to external noxious stimulation, including suction.

Post-anoxic lateralised myoclonic status in a 54-year-old comatose man. Note the periodic epileptiform complexes over the left hemisphere (periodic lateralised epileptiform discharges (PLEDs)) that invariably precede the time locked electromyography potentials recorded from the right forearm (lowest trace). In between the PLEDs there is low voltage 1–6 Hz activity. The whole pattern, including the rate of the discharges, remained unresponsive to noxious stimuli, including suction (performed here between the two arrows).

Non-convulsive complex partial status epilepticus. The EEG shows ongoing subclinical seizures over the right temporal areas without clinical accompaniments on video.
Alpha/beta coma pattern. Note the diffuse unremitting low voltage rhythmic 10–16 Hz activity that showed no response to external noxious stimuli, including suction (arrow); there were no changes in the ECG either. A follow-up EEG 7 days later off sedation showed only sparse low voltage activity, a stage before complete electrical suppression. The patient died 1 day later. The EEG changes seen during noxious stimulation are artefactual.
Somatosensory evoked potentials
Short latency somatosensory evoked potentials (SSEPs) are valuable in assessing prognosis because they provide information about the integrity of the afferent pathways via the brainstem and thalamocortical projections to the primary somatosensory cortex. They are also less susceptible than the EEG to sedative drugs, metabolic factors and sepsis. Subcortical involvement is reflected by slowing of the central conduction time and reduction of the N20 amplitude, while cortical injury causes absence of N20 only when there is extreme damage. Bilateral absence of the cortical N20 response, in the absence of known pre-existing cortical lesions is interpreted as widespread cortical injury after cardiac arrest with a high specificity for poor outcome.27 However, a normal N20 has poor accuracy for predicting good outcome.
Short latency somatosensory evoked potentials (SSEPs) are valuable in assessing prognosis
Long latency SSEPs (N70) are thought to reflect complex corticocortical connections important for intellectual functions, and their presence has been associated with a good outcome28; however, the predictive value of their absence for poor outcome is less certain than the N20.
Imaging
In the first 2 days after hypoxic–ischaemic brain injury, CT may show diffuse swelling with effacement of the basal cisterns, ventricles and sulci, attenuation of the grey–white matter interface29 and hypodensity of the cortical grey matter and basal ganglia (caudate, lenticular nucleus, thalamus and putamen) due to cytotoxic oedema. There is also hypodensity of the white matter due to distension of the deep medullary veins and consequent obstruction of the cerebral venous drainage. Focal areas of infarction may develop in the basal ganglia or cortical boundary zone territories.
MRI is undertaken less commonly because patients often require sedation, ventilation and airway protection and, therefore, transfer to and from radiology departments is difficult, but it may be particularly helpful in revealing the extent of damage. In the first few days, diffusion weighted imaging (DWI) and fluid attenuated inversion recovery (FLAIR) images show widespread hyperintensity, initially involving the basal ganglia, caudate, striatum and thalamus followed by the cortex and subcortical white matter, cerebellum and hippocampus.22 30 Conventional T1 and T2 weighted scans are normal. Diffusely abnormal findings on DWI and FLAIR correlate with a poor outcome.31 32 Apparent diffusion coefficient (ADC) mapping may add greater precision with severe reduction in whole brain ADC predicting a poor outcome.
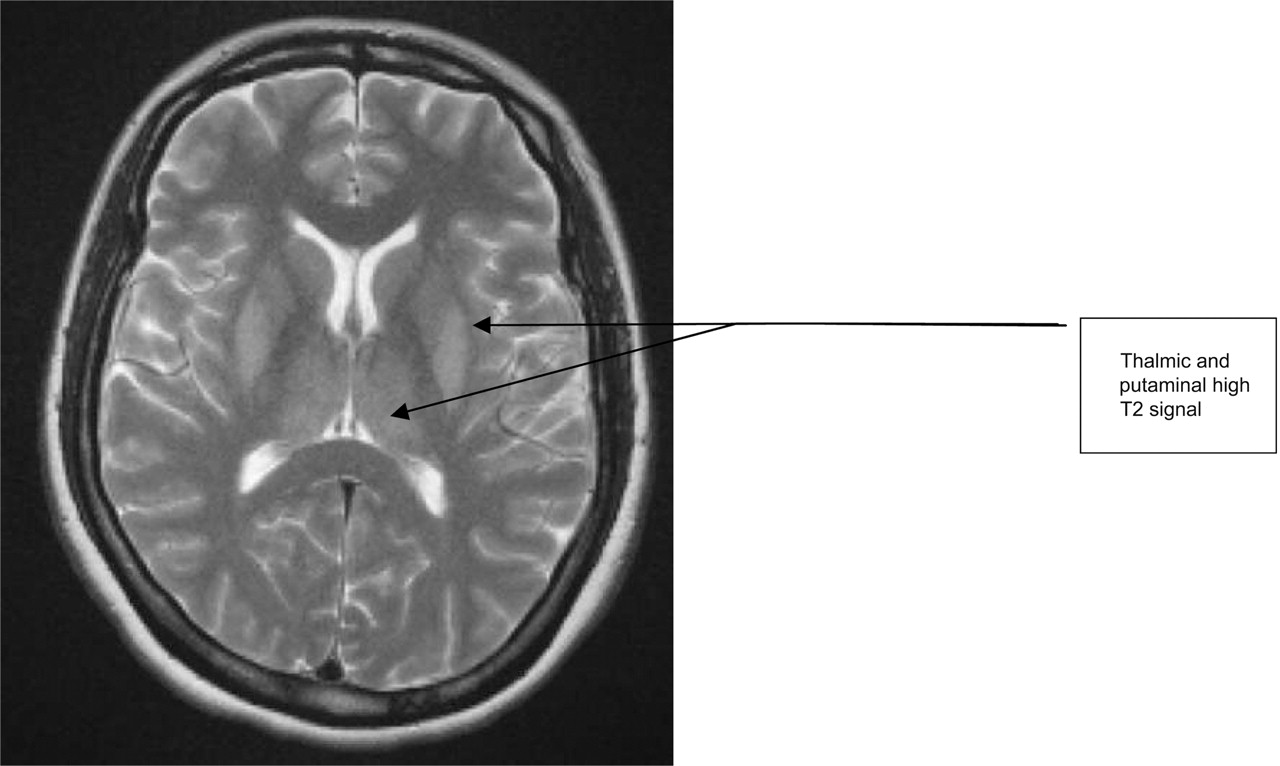
In the subacute phase (7–20 days) there is progressive resolution of brain oedema with disappearance of DWI hyperintensity (pseudo-normalisation). Extensive basal ganglia, cortical and hippocampal grey matter change is seen on FLAIR and T2 weighted images but white matter hyperintensity may also develop on T2 weighted images. Similar changes are seen after predominantly hypoxic brain injury (figure 6). Figure 7 shows subacute changes after hypoxic–ischaemic brain injury. High signal persists on DWI but extensive changes are seen on T2 and FLAIR. The ADC shows pseudo-normalisation in the deep gray matter but restricted diffusion persists in the occipital and perirolandic cortex. Rarely, there may be extensive, diffuse white matter change without involvement of the deep grey matter (figure 8).

Isolated hypoxic brain injury is usually caused by asphyxia such as after strangulation. Deep grey matter caudate, putamen and thalami show high signal on T2 MRI.

After hypoxic–ischaemic brain injury, MRI changes include high signal in the caudate and putamen, less so in the thalami, with restricted diffusion on ADC in the occipital regions and perirolandic cortex. ADC, apparent diffusion coefficient; DWI, diffusion weighted imaging; FLAIR, fluid attenuated inversion recovery.

Diffuse white matter high signal following hypoxic–ischaemic brain injury. ADC, apparent diffusion coefficient; DWI, diffusion weighted imaging.
In the chronic phase there is diffuse atrophy. T1 and T2 sequences may show cortical laminar necrosis (ie, cell death involving layers III and IV of the cortical mantle).
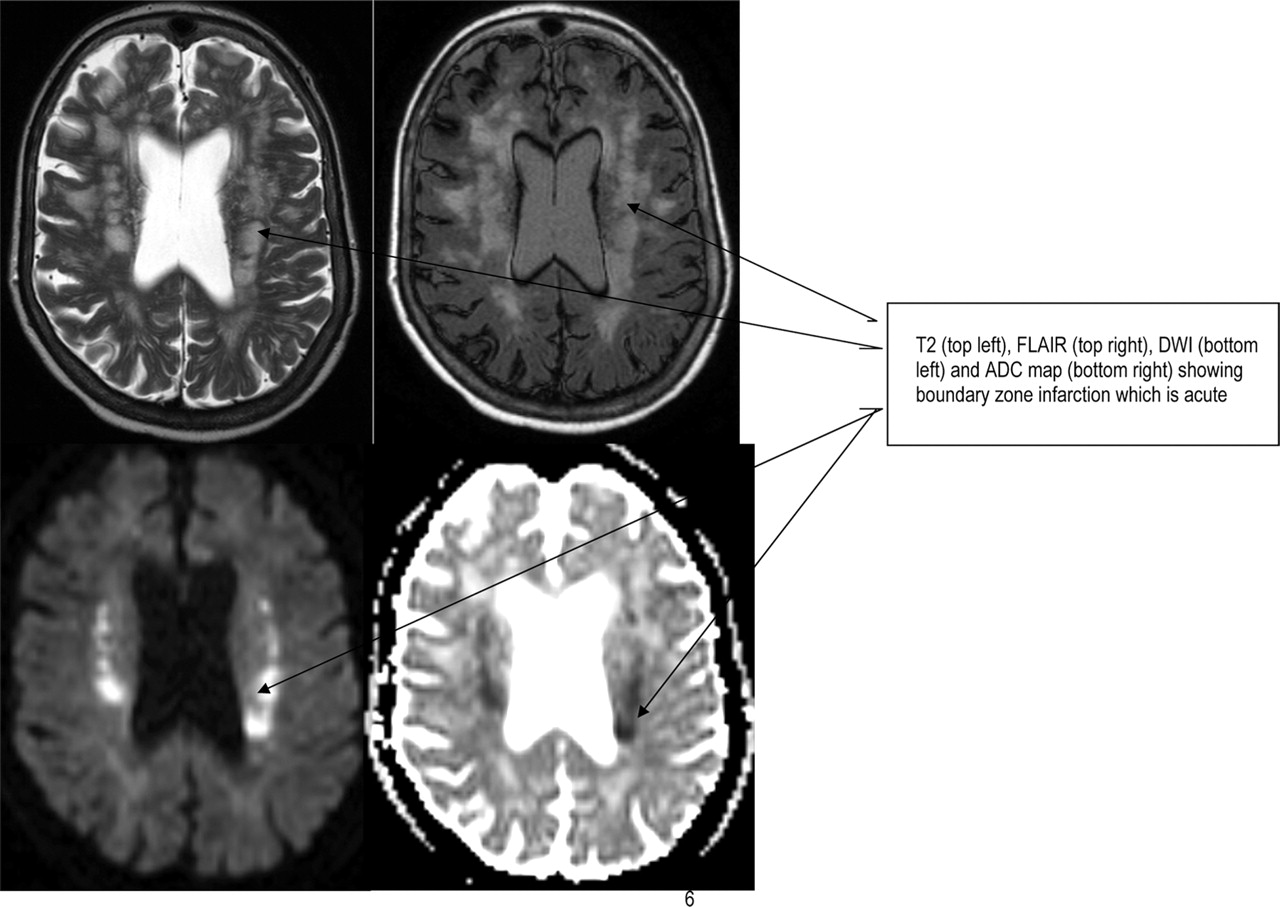
Infarction in boundary zone territories between the anterior, middle and posterior cerebral arteries (figure 9) and within the cerebellum often follows the more limited hypoperfusion which may occur during prolonged cardiac bypass.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
After severe circulatory compromise (eg, during problematic cardiac surgery), a pattern of boundary zone ischaemia and infarction often occurs. MRI shows high signal on T2 and FLAIR in these regions as well as restricted diffusion on ADC and high signal on DWI. ADC, apparent diffusion coefficient; DWI, diffusion weighted imaging; FLAIR, fluid attenuated inversion recovery.
It has been suggested that DWI hyperintensity restricted to the thalamus and selected cortical regions occurs after primary hypoxic injury but otherwise any imaging changes are difficult to distinguish from hypoxic–ischaemic injury. Delayed leucoencephalopathy may occur weeks or months after the initial insult and is more common after carbon monoxide poisoning or isolated hypoxic brain injury.
Biomarkers
Several blood tests have been suggested as markers of neuronal damage in hypoxic–ischaemic brain injury. Neuron specific enolase has been widely used after head injury, encephalitis and status epilepticus but data are conflicting following hypoxic–ischaemic brain injury. Although several prognostic studies have shown that significantly raised neuron specific enolase levels (>80 ng/ml) at days 1–4 post-resuscitation accurately predict poor outcome, there remains uncertainty about sensitivity and specificity.33 The role of S100 as a prognostic marker is unproven.34
Aspects of clinical management
As always in neurology, it is essential to take a meticulous history, from witnesses and family in this context, about any previous medical problems and the circumstances of the acute event and resuscitation. In the ICU situation this is often both difficult and distressing, and is therefore frequently neglected by the admitting medical and nursing teams.35 In patients who have been treated with hypothermia, or there is renal or hepatic impairment, the metabolism of sedatives and neuromuscular blocking drugs is unpredictable and often delayed, making history taking even more difficult.
It is essential to take a meticulous history, from witnesses and family
Always consider the possibility that the patient is locked-in
The most valuable assessment of the deeply unconscious patient is response to painful stimuli in the cranial nerve territory. The initial resulting limb response may be limited and it is often necessary to have another observer hold the limbs to feel whether flexion or extension develops following noxious stimulation. A generalised flexion response, however limited, is perhaps the most helpful indicator that a good outcome is possible but this needs to be interpreted with caution depending on the coexisting circumstances, including the delay after the hypoxic–ischaemic event and the presence of coexisting systemic factors such as organ failure.
Always consider the possibility that the patient is locked-in where there is preservation of consciousness despite complete paralysis of cranial nerve and limb musculature. Any residual responsive eye movements must be intensively sought.36
Ancillary investigations play an important role in the assessment and have traditionally been underused. As described above, MRI, EEG and SSEPs can provide detailed, accurate and reliable information about the distribution and severity of hypoxic–ischaemic brain injury.37
Inexperienced neurologists often feel pressurised to provide an ‘instant’ and definitive prognosis. Often this is impossible in the early stages. Repeated clinical assessment may be necessary before the outcome can be predicted. Also, it is necessary to wait for any effects of medication, hypothermia, sepsis and intercurrent metabolic effects to resolve. As a rule, it is extremely difficult to provide a clear prognosis within 3 days of the acute event unless the initial insult was clearly overwhelming. If a clear prognosis cannot be determined, the patient should be monitored regularly with the ICU team. In practice a critical decision is whether an oropharyngeal tube should be replaced by a cuffed tracheostomy which makes prolonged survival more likely even if ventilatory support is reduced or withdrawn. This decision therefore requires very careful consideration between intensivists, neurologists and the patient's family. However, the decision to undertake tracheostomy does not have to be made in the acute stages and can often be delayed for several days. It is important to emphasise that the decision to reduce or discontinue support cannot be rushed and all members of the team and the family must be in agreement with the management decisions.
It is important to maintain a clear and consistent approach in talking to relatives. A single doctor should lead the discussion. It is common for relatives to receive different opinions, conflicting advice or simply confusing and incomplete information from different doctors. As neurologists, our first responsibility should be to communicate with intensive care colleagues so that, as a team, we can all provide clear and decisive leadership and guidance to the patients' families.
The decision to reduce or discontinue support cannot be rushed
Practice points
Hypoxia and ischaemia are distinct mechanisms of brain injury but they usually coexist.
Ischaemic brain insults are more likely than hypoxic insults to cause permanent neurological sequelae.
The events surrounding cardiac arrest and resuscitation are critical in determining outcome; these include the initial insult, the effectiveness of immediate resuscitation and transfer, and the post-resuscitation management on the ICU.
Clinical assessment of patients within 72 h of hypoxic–ischaemic brain injury remains a valuable guide but must be interpreted with caution, particularly if the patient has been sedated at any time.
Neurophysiological tests are an important adjunct to diagnosis and determining prognosis; there are some characteristic patterns which suggest a poor prognosis.
Brain imaging changes develop soon after hypoxic–ischaemic brain injury; MRI (particularly DWI) may show the extent and severity within 24 h.
The pattern of residual neurological sequelae is highly variable, ranging from subtle neurocognitive deficits to severe permanent impairments in the level of awareness.
Long term implications
Following resuscitation the patient with hypoxic–ischaemic brain injury generally remains in a coma for several days although rarely this may persist for longer. Even if the level of consciousness improves, many patients remain in a vegetative or minimally aware state for prolonged periods. Recovery is then associated with a variable level of residual cognitive impairment.38
Impaired level of consciousness
Patients who have sustained a relatively mild hypoxic–ischaemic brain injury will regain consciousness within a few hours or, at most, 1 or 2 days. However, if the insult is more severe, recovery from coma is less certain and much slower, even in the absence of persisting metabolic, inflammatory, toxic or infectious factors which might prolong coma. There is usually improvement over 2–4 weeks to a state of wakefulness with eyes opening, but persisting impaired or absent awareness of self or environment. This vegetative state may be partially or totally reversible, or may progress to permanence or death.
The vegetative state can be considered permanent 3 months after injury but this figure is arbitrary and late recovery has been reported.39,–,41 It can only be recognised on the basis of exhaustive clinical assessment. Recent functional imaging studies have shown patchy preservation of cognitive activity, including some apparent responsiveness, which indicates that our understanding of these states is still uncertain.42 43 Furthermore, it is clear that patients previously thought to be vegetative have varying degrees of awareness and, rarely, might even be locked-in. We have previously emphasised the importance of excluding this possibility by detailed and repeated examination and EEG.
Progression from the vegetative state occurs with some patients regaining awareness and the development of appropriate responses. The minimally aware state (minimally conscious state)44 is characterised by the ability to follow a single command, to exhibit a gesture or verbal response to yes/no questions, the presence of intelligible verbalisation and responsive behaviours that are not reflexes or sustained visual pursuit to moving objects. The neurologist must be sure that any problems are not a manifestation of severe motor weakness or of a partial locked-in state.
Movement disorders
A variety of movement disorders may develop after hypoxic–ischaemic brain injury because the basal ganglia are particularly vulnerable. The pattern depends to some extent on the age of the patient and the severity of the insult. In younger patients with predominantly hypoxic brain injury, dystonia develops after several weeks, thought to be due to putaminal damage. In older patients with predominantly ischaemic insults, an akinetic rigid syndrome may develop as a consequence of pallidal damage. The onset of movement disorder may be delayed by several months, developing after a period of relative stability, more often in young patients.36
Boundary zone infarction
Boundary zone infarction is associated with hypoxic–ischaemic brain injury due to cardiac arrest. It also occurs after prolonged cardiac bypass associated with hypotension and here may be in part due to multiple emboli and not just hypotension. The vulnerable border zone regions lie between the territories of brain supplied by the three major cerebral arteries.45 The distribution and severity of clinical involvement is determined by the extent of the hypoxic–ischaemic insult and any underlying stenosis or occlusion of the cervical and intracranial vessels (eg, unilateral boundary zone infarction may develop distal to severe disease of one internal carotid artery). Various clinical syndromes have been described.45
Cognitive impairment
The pattern of cognitive problems in those who survive ranges from subtle impairment of recall to severe intellectual deficits. Memory function is preferentially impaired, particularly spatial and verbal memory and recall. Following a brief period of circulatory arrest the patient may be transiently confused or develop a severe Korsakoff-like amnesic state with profoundly impaired recall and recognition but retained short term memory. Amnesia following cardiac arrest is associated with limited lesions affecting the hippocampi bilaterally with little cortical damage.46 47 Recovery after more prolonged arrest is associated with intellectual deficits, including disorders of attention, orientation, insight and judgement.
Delayed post-hypoxic leucoencephalopathy
This is a rare condition which was initially thought to follow only carbon monoxide poisoning. However, it is now recognised after other insults causing primarily hypoxic injury (table 1). Patients seem to have made a complete recovery from hypoxic coma with normal cognitive function for 1–4 weeks before a relapse occurs with cognitive deterioration, frontal lobe (urinary incontinence and gait disturbance) and extrapyramidal signs (short stooping gait, parkinsonian expression and rigidity).48T2 MRI shows extensive white matter change and involvement of the basal ganglia. Up to 50% are said to make a good recovery but residual cognitive and extrapyramidal deficits are also common and this syndrome may even culminate in an unresponsive vegetative state.
Acknowledgments
This article was reviewed by Heini Mattle, Berne, Switzerland.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Other content recommended for you
- Early diffusion weighted imaging and expression of heat shock protein 70 in newborn pigs with hypoxic ischaemic encephalopathy
- Imaging in children presenting with acute neurological deficit: stroke
- What to see when you are looking at confusion: a review of the neuroimaging of acute encephalopathy
- Neurointensive care biophysiological monitoring
- Cortical abnormalities on MRI: what a neurologist should know
- An MRI review of acquired corpus callosum lesions
- Controversy of posterior reversible encephalopathy syndrome: what have we learnt in the last 20 years?
- Imaging in acute ischaemic stroke: essential for modern stroke care
- CJD mimics and chameleons
- Neuroimaging findings in human prion disease