Article Text

Abstract
Intracranial dural arteriovenous fistulae are rare, acquired lesions that may present with intracranial haemorrhage or progressive neurological deficits. Their cause is uncertain, although they are often associated with intracranial venous thrombosis. Their importance lies in the fact that they are potentially curable by endovascular or neurosurgical procedures, but easily missed on routine brain imaging. In addition, clinical presentation is variable, with no easily recognisable “syndrome”. A high index of suspicion is therefore required, as well as familiarity with the characteristic radiological abnormalities seen on appropriate imaging.
Statistics from Altmetric.com
Dural arteriovenous fistulae (DAVF) are abnormal, acquired connections between meningeal arteries and their associated draining veins. They may occur within the spine (usually presenting with progressive myelopathy in a middle-aged man), or intracranially, which will be the topic of this article. Although rare, the recognition of DAVF, particularly with non-haemorrhagic (“neurological” rather than “neurosurgical”) presentations is important because they are often treatable, with potential resolution of the neurological deficits. In this article we will present a series of case histories, with emphasis on the less well recognised non-haemorrhagic presentations, and a review of the literature which will focus on presentation and diagnosis, rather than detailed consideration of the surgical and endovascular treatment options.
AETIOLOGY
DAVF are distinct from “true” arteriovenous malformations (AVM), not least because they are almost certainly acquired, rather than congenital lesions (which pial AVMs probably are, although there is no irrefutable proof of this). The exceptions are the “vein of Galen malformations” seen in infants, which are probably congenital arteriovenous fistulae that present with high output cardiac failure due to the large volume of shunted blood. The natural history, age of onset, clinical presentation, radiological appearances and management of DAVF are also quite different from AVMs.
DAVF are rare, constituting just 10–15% of all intracranial vascular malformations.1–3 Their overall incidence is similar in both sexes, although an aggressive clinical course appears to be more common in men, largely due to differences in the location and drainage of the DAVF (carotid-cavernous fistulae may be more common in women and more likely to follow a benign course, whereas men seem more likely to feature drainage to cortical veins and therefore have a higher risk of complications, see below4).
Presentations of intracranial dural arteriovenous fistulae
Intracranial haemorrhage
Intracerebral
Subdural
Subarachnoid
Venous hypertension
Localised
tinnitus, cavernous-orbital syndrome
Generalised/diffuse
Intracranial hypertension, parkinsonism, dementia
Mass effect from venous ectasia (rare)
The cause of a DAVF is not always clear, but venous sinus thrombosis is commonly cited as a predisposing factor.5, 6 The mechanism is thought to be venous congestion and hypertension, leading to dilatation of small capillaries and subsequent opening of direct communication channels between small dural arteries and veins. However, the relationship between DAVF and venous thrombosis is complicated by the fact that venous hypertension and stasis caused by a DAVF can itself lead to secondary venous thrombosis (which sometimes leads to spontaneous resolution of the fistula—nature’s own endovascular therapy!).
Carotid-cavernous fistulae (CCF) may be considered separate from most other intracranial DAVF. They are usually classified into “direct” (“high flow”) or indirect (“low flow”) fistulae:
Direct CCF result from either trauma (blunt or penetrating) or rupture of an intracavernous carotid aneurysm; in both cases leading to direct communication between the cavernous portion of the carotid artery and the cavernous venous sinus.
“Low flow” or “indirect” CCF are also caused by abnormal flow between the carotid artery (usually external) and cavernous sinus, but via dural arteries and veins rather than directly. These are often spontaneous and occur more commonly in post-menopausal women (for unknown reasons, and in contrast to spinal DAVF which occur mainly in men), and are similar to the other intracranial DAVF discussed in this article.7
Case 1
A 65-year-old man was seen in the neurology clinic in April 2006 with an 18-month history of poor memory, declining mobility and frequent falls. He had a past medical history of severe alcohol dependency including several previous admissions with withdrawal seizures and acute confusional states. He had been investigated previously with brain CT and subsequently MR, reported as showing some small vessel vascular change and atrophy. He said he had not been drinking alcohol for over a year. Examination revealed impaired cognitive function with very slow responses, brisk jaw jerk and palmomental responses bilaterally. There was marked rigidity in the limbs, which had the characteristics of gegenhalten (paratonia). There was mild proximal weakness in the legs and marked gait apraxia. Review of his previous MR revealed widespread dilatation of cerebral veins, suggestive of an intracranial DAVF (fig 1A,B). Close inspection of his original CT showed unusual linear calcification, probably within intracerebral veins (fig 1C). Catheter angiography (fig 1D) confirmed a dural AV fistula arising at the left sigmoid/transverse sinus junction, with associated occlusion of the sigmoid sinus, and a second arising at the superior saggital sinus (Borden type 2). Endovascular embolisation of both fistulae, with further endovascular coil occlusion of the left transverse/sigmoid fistula was performed between November and December 2006. Repeat catheter angiography in August 2007 did not show any residual fistulae and when reviewed subsequently, his wife reported significant improvement in his mental function and in mobility, from being wheelchair bound to using a frame.

CLASSIFICATION
DAVF are classified according to one of several different schemes, of varying complexity. The most straightforward is that of Borden et al, which contains just three major types:
Type I drain directly into dural venous sinuses, or meningeal veins.
Type 2 drain into dural sinuses or meningeal veins, but in addition feature retrograde flow (due to excessive venous pressure) into subarachnoid veins.
Type 3 drain directly into subarachnoid veins and do not feature dural sinus or meningeal venous drainage.
Note that the arterial supply in each of these types is derived from meningeal vessels. Types 2 and 3 are considered more likely to result in both haemorrhage and symptoms due to secondary venous hypertension, and are usually treated actively.8 A retrospective review of 98 DAVF patients reported a significant correlation between Borden type and clinical presentation.9
Other classifications are available, notably that of Djindjian (with patterns of venous drainage correlating with symptoms)10 and Cognard (helpful in stratifying risk and treatment modality),4 but are unlikely to be of interest to most practising neurologists. In addition, there are separate classification schemes for CCF,11 although again most neurologists will probably be satisfied with the simple “high flow/direct” versus “low flow/indirect” classification.
Case 2
A 48-year-old man was admitted in April 2005 with a three-month history of progressive deterioration of memory, speech disturbance, impaired balance, left-sided weakness and double vision. He had no significant past medical history. On examination he was ataxic with a partial left 3rd nerve palsy and grossly confused. Brain CT revealed bilateral low density in the thalami, with additional change in the upper brainstem. MRI confirmed the CT findings (fig 2A,B). A number of diagnoses were considered including lymphoma and prion disease. Further review of the radiological images raised the possibility of dilatation of the straight sinus (fig 2C). On this basis, MR angiography (and subsequent catheter angiography) was performed which demonstrated a dural venous sinus fistula arising from the left transverse sinus (with associated occlusion of the sigmoid sinus) causing retrograde flow within the straight sinus and deep cerebral veins, venous hypertension and secondary ischaemia (Borden type 2). This was treated with endovascular embolisation, resulting in dramatic clinical improvement. Catheter angiography in May 2006 showed persistent occlusion of the fistula. He continues to remain well and is back to full-time work and normal daily activities.

CLINICAL PRESENTATION
There are two major modes of presentation of DAVF; due to haemorrhage or venous hypertension/congestion. Rarely, venous dilatation and ectasia can be severe enough to cause mass effect and a “tumour-like” presentation.4, 12
Case 3
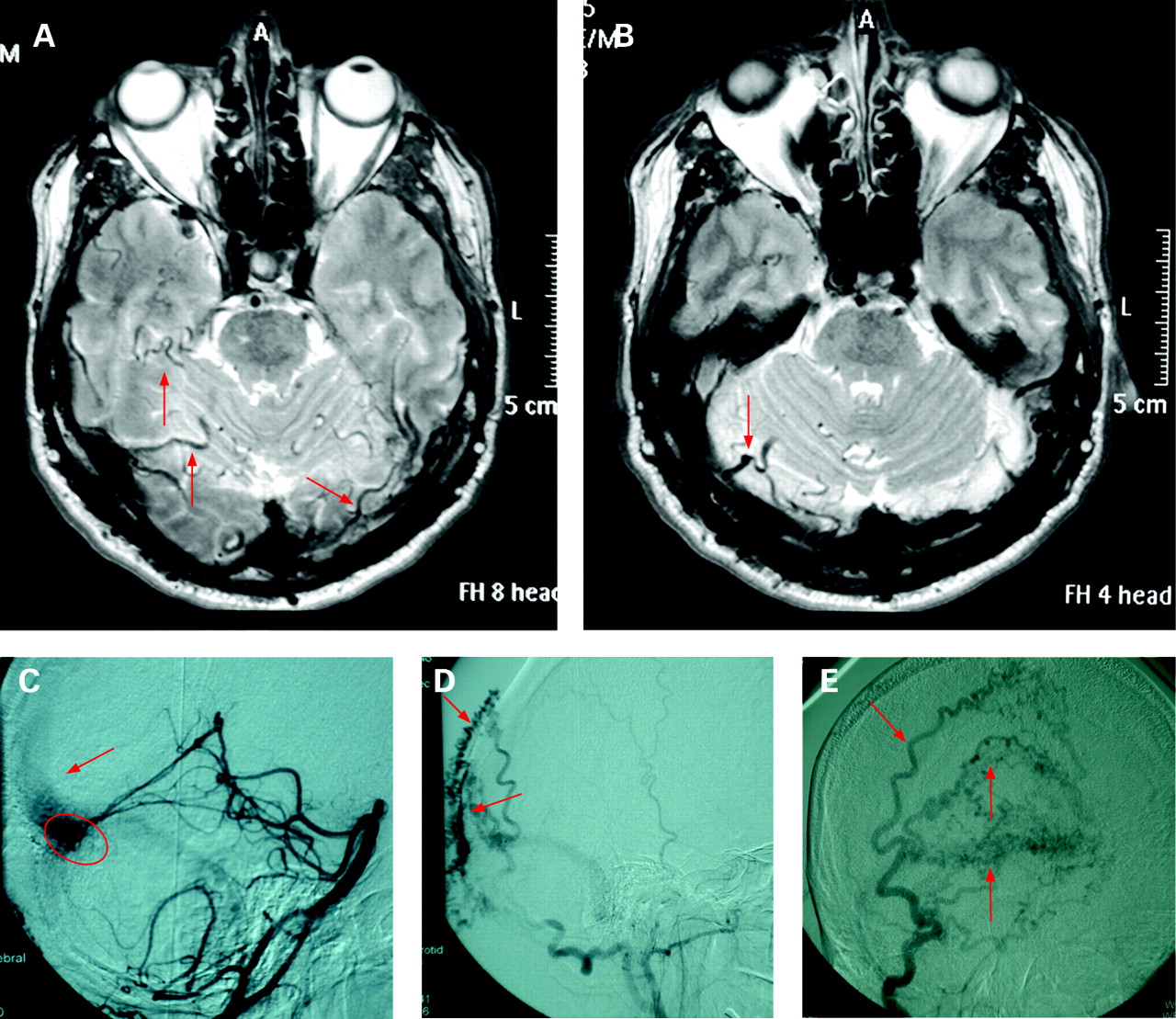
A 68-year-old man was referred to the neurology clinic in April 2006 with a four-month history of mild “confusion”, poor memory and frequent falls. He had a past history of hypertension and a right cerebellar haemorrhagic stroke in 1998, with good recovery. On examination he was noted to have very brisk knee reflexes and an ataxic gait, which had been attributed to his previous stroke. There was mild apraxia of hand gestures but language function was intact. His episodic memory was significantly impaired. No other focal neurological deficits were noted. MRI showed evidence of an old, right cerebellar haemorrhage, but also marked dilatation of the cortical veins around the tentorium and basal cisterns (fig 3A,B). Subsequent MR angiography showed an abnormal transverse sinus, strongly suggestive of a high flow dural fistula. Catheter angiography (fig 3C–E) confirmed a complex fistula arising from the left transverse sinus (again with associated occlusion of the sigmoid sinus), draining retrogradely into the superior sagittal sinus, and was notable for an extraordinarily long transit time of contrast, due to retrograde pressure from the venous sinuses being almost equal to arterial pressure. There was an acute encephalopathic deterioration immediately after catheter angiography which resolved spontaneously in a few days and was not accompanied by any radiological changes. This was interpreted as a contrast reaction, exacerbated by the marked slowing of venous flow. He underwent endovascular treatment of the fistula in three stages, involving access from the various feeding arteries and venous sinuses. Following the third stage, there was dramatic improvement in the angiographic appearances and contrast transit time, which was now near normal. There was marked clinical improvement. In August 2007 he deteriorated. Repeat MRI and subsequent catheter angiography demonstrated recurrence of the high flow fistula with retrograde flow into the superior sagittal and straight sinuses. Further endovascular treatment resulted in angiographic resolution of the fistula. By January 2008, he was much improved clinically and remains fully independent, though with some mild residual gait ataxia.

Intracranial haemorrhage can be intracerebral, subdural or subarachnoid, depending on location and drainage characteristics of the DAVF, although intracerebral seems the commonest.3 The overall risk of haemorrhage from DAVF is about 2% per year and depends on the site and haemodynamics of the lesion13, 14 (see below).
Presentations in the absence of haemorrhage (and presumably due to venous hypertension, either focal or generalised) include:
These “neurological” presentations are usually characterised by a subacute or slowly progressive onset, in contrast to haemorrhagic complications which usually present acutely in a “stroke-like” manner.
With both haemorrhage and venous congestion the size, location and drainage pattern of the fistula are important in determining the clinical presentation. Intracranial DAVF that drain into a major dural sinus usually follow a benign clinical course.5, 14, 28, 29 However, if sinus drainage occurs with retrograde flow into arterialised leptomeningeal veins, or if the fistula drains solely into cortical leptomeningeal veins, a more aggressive natural history is seen.14, 30–33 In particular, the presence of a secondary venous varix seems a strong predictor of future haemorrhage.13, 14
Because of their restricted anatomical boundaries, carotid-cavernous fistulae (CCF) present with a fairly narrow range of symptoms and signs. Extension of haemorrhage into the brain parenchyma is very rare (but can occur), and symptoms are usually restricted to a cavernous sinus/orbital syndrome with a combination of orbital pain, proptosis, chemosis, opthalmoplegia and orbital bruit, and later visual failure due to secondary glaucoma. Direct or “high flow” CCF usually present with subacute evolution of symptoms with prominent signs, whereas indirect fistulae may go unrecognised for a considerable time, due to the lack of physical signs.7
Case 4
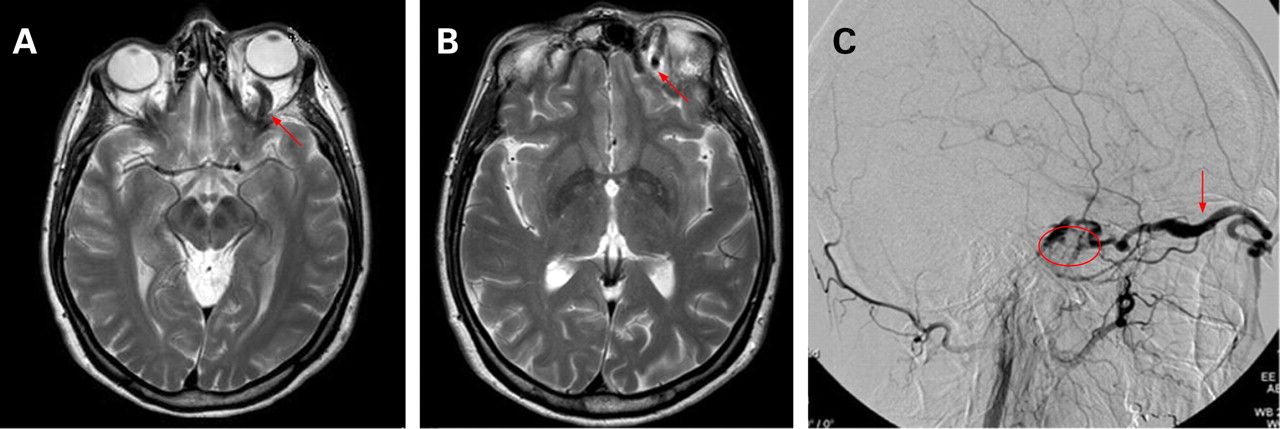
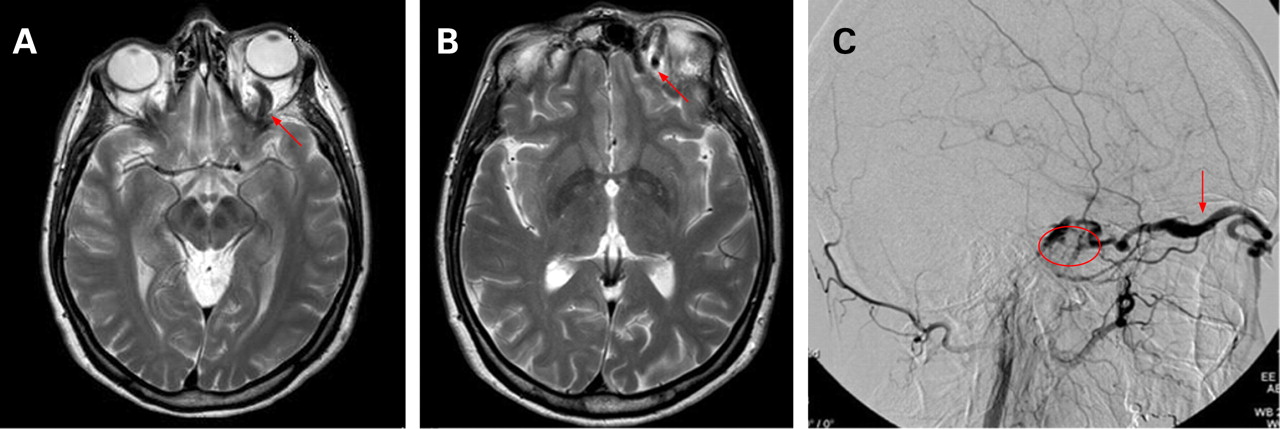
A 53-year-old woman presented to the outpatient neurology clinic in October 2007 with a history of headache. This had been present for approximately six weeks, and was constant. The pain was well localised to the left peri-orbital region, and was associated with some intermittent “puffiness” around the eye and conjunctival injection. There was no history of previous trauma. There were no visible abnormalities of the eye to examination, no bruits anywhere, and no neurological signs. A CT with contrast was requested and a trial of indometacin started for possible hemicrania continua. The CT was reported as probably normal, but subtle asymmetry of contrast density in the region of the cavernous sinus was commented upon. At clinical review two weeks later, a partial response to indometacin was noted. However, during the consultation a visible pulsation was noted just above the left eye, beneath the eyelid. An orbital bruit was now clearly audible. A diagnosis of probable carotid-cavernous fistula was made, and confirmed on subsequent MRI and catheter angiography (fig 4A–C). The fistula was of the indirect, low-flow type.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
While awaiting endovascular therapy, diplopia developed and treatment was arranged urgently. The fistula was successfully occluded by endovascular treatment, with rapid resolution of diplopia and headache over the subsequent 48 hours.
DIAGNOSIS
Those DAVF presenting with haemorrhage will usually come to the attention of radiology departments one way or another, but the underlying cause of the bleed may still be missed. Subarachnoid haemorrhage presentations would usually be investigated with angiography (CT, MR or catheter), and the fistula therefore detected in most cases. On the other hand, with parenchymal or subdural haemorrhage a much higher index of suspicion is required; for example, if there are no obvious risk factors such as hypertension, anticoagulation, falls or alcohol excess, or the location and/or appearance of the bleed is unusual (for example, haematoma not in the typical “hypertensive” distribution of basal ganglia and internal capsule), a careful review of a post-contrast CT scan might reveal a dilated vessel in relation to the bleed, or calcification within chronically congested veins (for example, case 1). MRI and MR angiography or venography are more likely to reveal the abnormality, although again the changes may be subtle and there have been cases of DAVF with normal MR imaging, detected only on subsequent catheter angiography.13, 33, 34
Non-haemorrhagic presentations are more likely to present to neurologists, and because the clinical picture varies widely (depending again on size, location and drainage pattern) with no “typical” or easily recognised presentation, a high index of suspicion is required, together with careful review of the imaging. One does not see the tangle of “flow voids” as in AVMs, but rather local (case 2) or generalised (case 1) venous dilatation and/or parenchymal signal change due to venous congestion (case 2). The changes may be subtle however, even on good quality MR images, necessitating catheter angiography (case 2).
One rare, but important observation in patients with DAVF, has been acute deterioration after diagnostic (or therapeutic in patients with intracranial hypertension) lumbar puncture.35 This can be severe, with sudden coma and death due to tonsillar herniation. With this in mind, it is interesting to note that some case series have reported “incidental” minor tonsillar herniation on MRI of patients with DAVF, which has resolved following treatment of the fistula.4
A further complication to beware of is described in case 3, following catheter angiography; an acute encephalopathic state which resolves spontaneously and attributed to a contrast reaction (secondary to extremely prolonged transit times and thus exposure to contrast).
MANAGEMENT
This is usually in the hands of neurosurgeons and interventional neuroradiologists (often in a combined approach) and will be dealt with only briefly here. Unsurprisingly perhaps, this is an area untroubled by randomised controlled trials—the evidence base is dominated by case series.
Some DAVF can be managed conservatively, for example if the only symptom is non-disabling tinnitus, and investigation reveals a “low risk” fistula without cortical venous drainage or ectasia. In addition, spontaneous resolution may occur which is usually attributed to thrombosis of the fistula. However, most DAVF presenting with haemorrhage or progressive neurological signs will require treatment. This may include endovascular occlusion, surgical disconnection of the fistula, radiosurgery or a combination of treatment modalities.13, 34
Quite striking improvement in the clinical signs may be seen after treatment of the fistula, although the clinician following up the patient should be aware that later recurrence is well described, particularly if complete obliteration of the fistula was not possible initially.
Practice points
Intracranial dural arteriovenous fistulae (DAVF) are rare, but potentially treatable causes of intracranial haemorrhage and a wide variety of progressive and sometimes fatal neurological problems.
DAVF are acquired lesions, distinct from congenital AV malformations, possibly secondary to intracranial venous thrombosis.
A high index of suspicion is required, particularly in non-haemorrhagic cases, because both CT and MR scanning—even with contrast—may be normal or show only non-specific, secondary changes of venous hypertension (beware if scans are reported by non-neuroradiologists); catheter angiography is the “gold standard” investigation.
Lumbar puncture may rarely lead to sudden deterioration, coning and even death.
Treatment may be curative, and requires a multidisciplinary approach involving neurologists, interventional neuroradiologists, neurosurgeons and occasionally radiotherapists.
Recurrence is well described even after apparently definitive treatment, so long-term follow-up is required.
Acknowledgments
We are grateful to Dr Mark Doran for allowing access to the records of case 2, and Dr Hans Nahser and Sacha Niven for advising on the neuroradiology. This article was reviewed by Rustam Al-Shahi Salman, Edinburgh, UK.
REFERENCES
Other content recommended for you
- Dural arteriovenous fistulas as a cause of intracranial hypertension due to impairment of cranial venous outflow
- Outcome of transarterial treatment of dural arteriovenous fistulas with direct or indirect cortical venous drainage
- Flow control techniques for Onyx embolization of intracranial dural arteriovenous fistulae
- Interventional neuroradiology
- Intracranial dural arteriovenous fistulas with or without cerebral sinus thrombosis: analysis of 69 patients
- Cranial dural arteriovenous fistula: transarterial Onyx embolization experience and technical nuances
- Embolization strategies for intracranial dural arteriovenous fistulas with an isolated sinus: a single-center experience in 20 patients
- Engorged medullary vein on CT angiography in patients with dural arteriovenous fistula: prevalence, types, and comparison between regional and extensive types
- Development of an intracranial dural arteriovenous fistula after venous sinus stenting for idiopathic intracranial hypertension
- Development of an Intracranial Dural Arteriovenous Fistula after Venous Sinus Stenting for Idiopathic Intracranial Hypertension