Article Text

Abstract
AIM To investigate the relation between lesion volume, lesion location, and clinical outcome in children with infarction in the territory of the middle cerebral artery (MCA).
PATIENTS AND METHODS Children with MCA territory infarcts were selected retrospectively from a database of children with ischaemic stroke. Lesion volumes were expressed as a percentage of the supratentorial intracranial volume and were categorised as “small”, “moderate”, or “large”. Lesion location was categorised as cortical or purely subcortical. Outcome was ascertained by parental questionnaire and was categorised as “good” or “poor”.
RESULTS 38 patients were identified (median age 6 years); 21 patients had lesions that involved cortical tissue. Outcome was good in 12 cases and poor in 26 cases (including 2 children who died). Although there was no significant effect of lesion size or lesion location on outcome for the group as a whole, all children who had infarcted more than 10% of intracranial volume had a poor outcome. Of note, some children with small subcortical lesions had pronounced residual deficits.
CONCLUSIONS Although the outcome after a small infarct in the MCA territory is variable and unpredictable, infarction of more than 10% of intracranial volume is universally associated with a poor outcome. Characterisation of lesion volume and topography might be helpful in identification of such children for participation in future trials of treatments for acute stroke.
- stroke
- outcome
- intracranial volume
Statistics from Altmetric.com
Although acute stroke treatments are promising, many are also potentially toxic. Patient selection for such interventions remains a difficult issue, especially in the paediatric age group, where patient numbers are small, making large randomised controlled trials difficult. Given that, anecdotally, the outcome after ischaemic stroke in childhood is thought to be good, many clinicians would hesitate before instituting potentially hazardous interventions in children. This suggests that a method of predicting clinical outcome soon after the event would be useful.
Animal model studies of cerebral ischaemia have reported the volume of infarcted brain tissue as a measure of the efficacy of interventions aimed at limiting ischaemic damage.1 It is unclear how this translates to clinical outcome in humans. The territory of the middle cerebral artery (MCA) is the most frequently affected arterial territory in childhood stroke.2 Saunders and colleagues3 showed recently that measurement of infarct volume on T2 weighted magnetic resonance imaging (MRI) scans taken within 72 hours of stroke predicted clinical outcome in a group of adults with cortical MCA territory infarction. If there is an association between lesion volume and outcome in children, knowledge of this would be useful in the management of children presenting with acute ischaemic stroke, specifically in targeting groups of children for therapeutic trials.
The influence of lesion location and of clinical factors must also be considered in this analysis. In particular, involvement of cortical tissue is thought to affect outcome adversely, whereas it has been reported that subcortical infarction in childhood carries a good prognosis.4 5 However, it is unclear whether this is always the case or whether lesion size influences this relation in any way. Finally, some studies have reported that children with a pre-existing medical condition (“symptomatic” stroke) have a worse prognosis than those with apparently “idiopathic” stroke.4 6 7
We undertook a retrospective study to explore the influence of lesion size, lesion location, and clinical variables on outcome in a population of children with MCA territory infarcts.
Methods
PATIENTS
Children seen at Great Ormond Street Hospital for Children between 1991 and 1996 who had been scanned using MRI and who had evidence of an infarct in the MCA territory were eligible for inclusion. Patients were selected retrospectively from a database that forms part of a longitudinal study on ischaemic stroke in childhood. The patients were investigated for vascular and non-vascular risk factors for stroke according to a standardised protocol.8The patients known to be at risk of stroke before the actual event (for example, those with congenital cardiac disease) were categorised as having symptomatic stroke. The remaining children, in whom stroke occurred apparently out of the blue, were termed the idiopathic stroke group. Previously silent risk factors for stroke were discovered after investigation in some of this group. Children known to have moyamoya syndrome were excluded because many of them had multiple lesions and neurological impairment in this group might be related to cerebral hypoperfusion without frank infarction. Children who had a stroke within the first 28 days of life were also excluded.
OUTCOME
Functional scales used to evaluate outcome after stroke in adults do not cover areas that are important in the paediatric population. In adults with stroke, data obtained from simple questions about outcome have been shown to correlate well with detailed functional assessments.9 In our study, outcome was assessed by means of a parental questionnaire, designed by us as part of another study (V Ganesan et al, unpublished, 1996), which had prior approval from the regional ethics committee. In the case of parents who did not respond, the questionnaire was filled out by one of two neurologists (VG or FJK), either at a clinic visit or from case note review. The aim of the questionnaire was to evaluate whether the child had a disability that was sufficient to interfere with his/her age appropriate activities of daily living. The questionnaire comprised seven simple questions exploring whether the child required assistance in the home or school environment, and specifically the areas of motor and language function, educational requirements, behaviour, and epilepsy. Five of the questions required simple “yes” or “no” responses. The remaining two questions required a judgment about the severity of motor impairment on a four point scale, with clear guidelines given for scoring. A cumulative “outcome score” was calculated from the responses to these questions with a minimum possible score of 0 and a maximum possible score of 13. Before administration of the questionnaire it was decided that patients scoring ⩽ 4 would be categorised as having “good” outcome (impairments unlikely to interfere with day to day life), and that patients scoring > 4 would be categorised as having “poor” outcome. Patients who died as a direct effect of the stroke were included in the poor outcome group. In a previous study, parental responses to this questionnaire correlated well with objective assessments by paediatric therapists (V Ganesan et al, unpublished, 1996).
MEASUREMENT OF INFARCT SIZE AND TERRITORY
The patients were scanned on a 1.5 T Magnetom SP4000 (Siemens, Erlangen, Germany) using a standard quadrature head coil. Turbospin echo T2 weighted images (TE = 90 ms, TR = 4600 ms) or double echo short tau inversion recovery (DESTIR) (TE = 5 ms, TR = 3500 ms, TI = 145 ms) images were acquired throughout the whole head with 5 mm slice thicknesses and a 2.5 mm slice gap. A three quarters field of view was used in all cases, together with matrix sizes of 135 × 256 for the DESTIR and 192 × 256 for the turbospin echo images.
Axial T2 weighted MR images were imported into a SUN workstation. Infarct volume was measured by drawing a region of interest around the area judged to be abnormal on the T2 weighted image using the image analysis package Xdispim.10 Infarcted tissue was defined as tissue having abnormal high signal on T2 weighted images.
The variation of brain volume with age had to be taken into consideration when comparing lesion volumes between patients of different ages. Therefore, lesion volumes were expressed as a percentage of supratentorial intracranial volume (ICV) (including the supratentorial cerebrospinal fluid). To measure ICV, a region of interest was drawn around the whole brain, using the method described above, on serial axial T2 weighted images from images acquired at the highest level of the brain down to the level of the midbrain.
To calculate the absolute measured volumes, the measurements of area were corrected for the size of the field of view and matrix size; the areas obtained on each slice were multiplied by the slice thickness and summated. Finally, the lesion volume was expressed as a percentage of the supratentorial ICV (%ICV infarcted).
To investigate the reproducibility of this method of measurement, lesion volume and ICV were determined on two separate occasions by two independent observers, one a paediatric neurologist (VG), the other a neuroradiologist (VN). The mean per cent difference and 95% confidence intervals were calculated within and between observers for the measurements of ICV and infarct volume.
Lesions were divided into categories comprising “large”, “moderate”, and “small” based on the 33rd and 67th centiles for the mean values of %ICV infarcted for the whole group. This categorisation was selected before the start of the study. In the case of the four patients with bilateral lesions, the total infarct volumes for both hemispheres was summated. However, these patients were not included in the statistical analysis examining the relation between lesion volume and outcome because the small numbers meant that the effect of having bilateral lesions could not be examined separately.
To investigate whether cortical involvement was an important determinant of outcome in our group of patients, the lesions were divided into those that involved cortical structures and those that were confined to subcortical structures. Subcortical structures were taken to include the subcortical white matter and deep grey matter; “cortex” referred solely to the superficial grey matter. Subdivision of patients into more specific clinicopathological groups was not possible because of the small number of patients in our study.
Results
PATIENT CHARACTERISTICS
A total of 38 children were identified, ranging in age from 6 months to 15 years (median, 6 years). There were 22 boys. In 24 cases, MRI studies were available from the first week after the acute stroke; six patients were scanned within one month and five within one year of the stroke. Three patients were imaged much later: after five, six, and eight years. One child had an acute deterioration after making an initial recovery; in this instance the scan obtained after the second event was analysed. Four children had had previous strokes and bilateral lesions. In two of these cases, areas of infarction that had occurred “silently” (without any corresponding clinical event) were apparent on T2 weighted MRI at the time of a second, clinical stroke. Eleven children fell into the symptomatic stroke category (indicated with an asterisk in table 1). Table 1 summarises further clinical details.
Patient details, lesion size, lesion location, and outcome
INFARCT SIZE AND TERRITORY
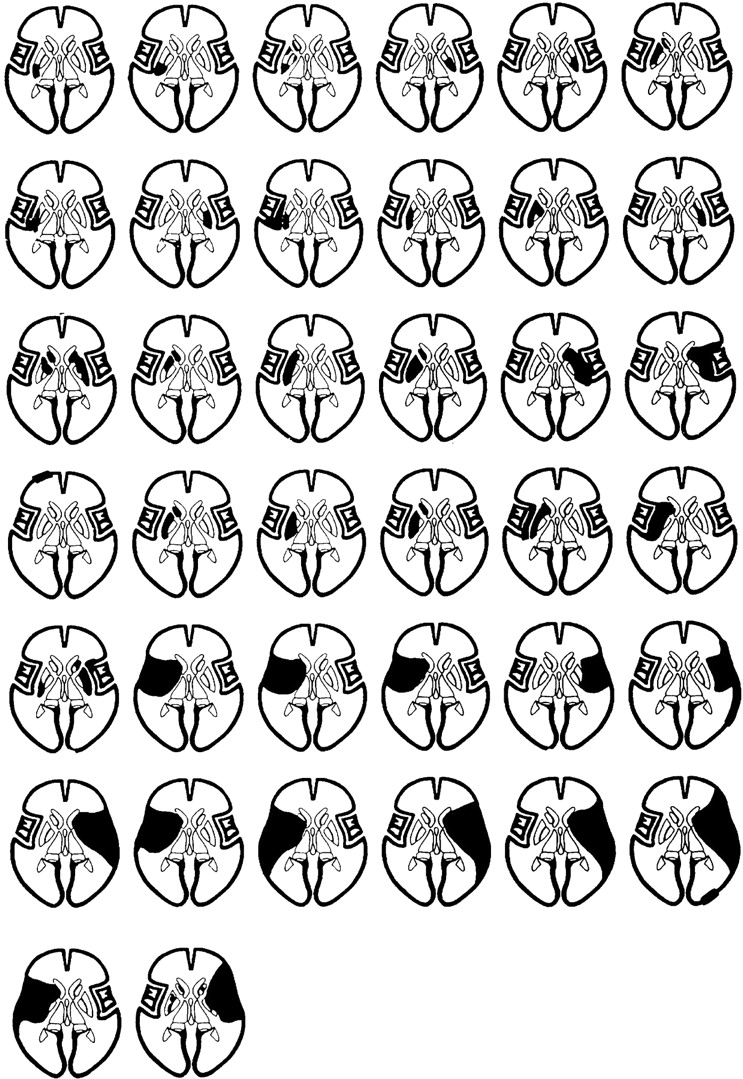
The lesion volumes ranged from 1 cm3 to 244 cm3, which represented a range of 0.12% to 21.52% of ICV. Figure 1 illustrates the topographical characteristics of the lesions for individual patients. Figure 2 shows the allocation of lesions into large, moderate, and small categories (defined according to the 33rd and 67th centiles for mean values of %ICV infarcted (1.03% and 5.29% ICV)) by each observer.
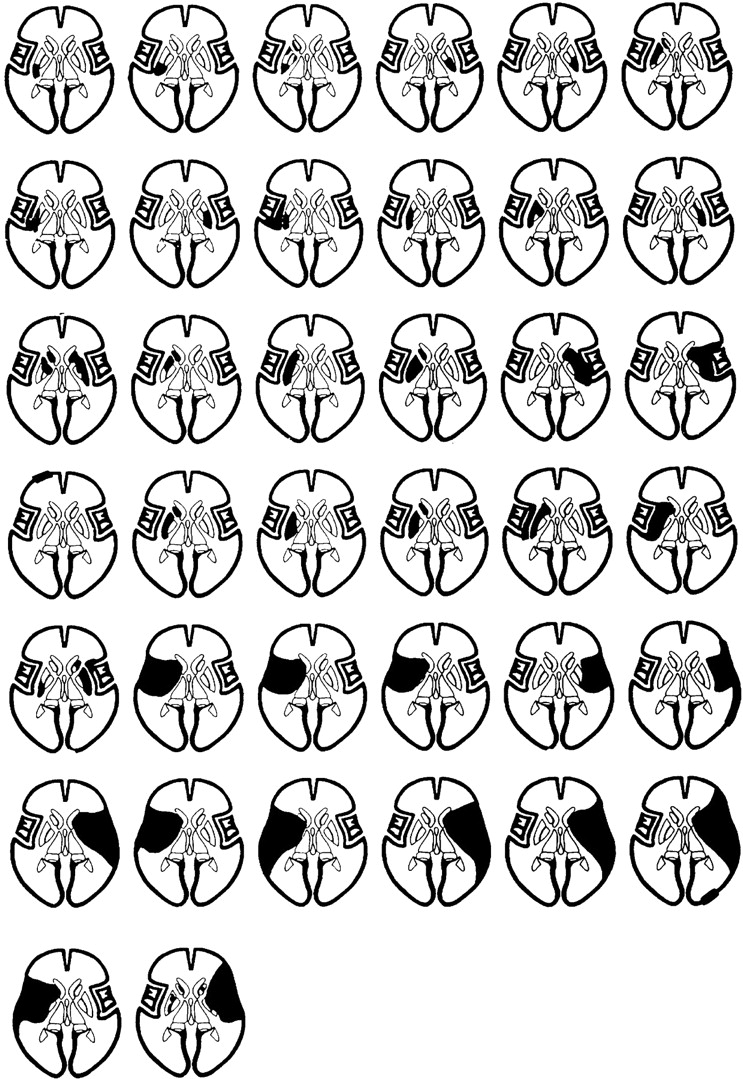
Line drawings of a transaxial section through the brain at the level of the IIIrd ventricle illustrating the lesion characteristics for individual patients. Each figure represents one patient and the figures are arranged in ascending order of lesion size.

Per cent intracranial volume (%ICV) infarcted measured by observers 1 and 2, plotted on a logarithmic scale to illustrate the allocation of the small lesions. The horizontal lines indicate the 33rd and 67th centiles for the values of mean %ICV infarcted, according to which lesions were allocated into “small”, “moderate”, and “large” categories.
Twenty one of the lesions involved the cortex and the remaining 17 lesions were confined to subcortical structures. All but one of the lesions that involved the cortex also involved subcortical structures (fig 1).
REPRODUCIBILITY AND AGREEMENT
Table 2 summarises the data on the reproducibility of the measurements of ICV and infarct volume within and between the two observers. The reproducibility of volume measurements for small lesions was much poorer than for large lesions, as is evident in fig 2 and table 2; the large number of relatively small lesions in our study tended to increase the mean per cent difference between observers for values of lesion volume.
Interobserver and intraobserver reproducibility of intracranial volume and infarct volume measurements
There was agreement between the observers on the allocation of the lesions into the three groups in 33 of 38 cases. In the five cases where lesions were allocated into different categories, the differences in the %ICV volume infarcted between the two observers was 1.29%, 1.44%, 0.18%, 0.14%, and 0.13%; therefore, these differences were very small, indicating that these values lay around the cut off points for the groups (fig 2). The final allocation of individual patients into the categories was based on the mean value for %ICV infarcted.
RELATION BETWEEN LESION SIZE, LOCATION, AND OUTCOME
Twelve children had a good outcome and 26 children had a poor outcome, as defined previously. Two children died as a result of intractable intracranial hypertension in the acute phase of stroke; they were included in the poor outcome category.
The relation between infarct size, location, and outcome, summarised in table 1 and fig 3, is not simple. In a logistic regression model there were no significant relations between infarct size category (p = 0.90), infarct location (p = 0.88), the presence of a previous risk factor (p = 0.39), and outcome for the group as a whole.

{kind=link}
{kind=link}
{kind=link}
(A) Outcome related to infarct size category for the 34 children with unilateral lesions (see methods for definitions of infarct size and outcome categories). Of the eight children with previous risk factors, one had good outcome and seven had poor outcome; one had a small lesion and seven had large lesions. (B) Outcome related to mean per cent intracranial volume (%ICV) infarcted and lesion location. See results section for definition of “cortical” and “subcortical” infarct locations.
Considering the subgroups of children with unilateral cortical lesions (n = 18) and unilateral subcortical lesions (n = 16) individually, lesion volume did not significantly influence outcome in either group (logistic regression, p = 0.28 for those with cortical lesions; logistic regression, p = 0.5 for those with subcortical lesions).
However, it was apparent that there was a relation between infarct volume and outcome for the largest lesions. Children who infarcted more than 10% ICV were significantly more likely to have a moderate or severe level of residual disability (Fisher’s exact test, p = 0.036) (fig 3). In all these cases the lesions involved cortical tissue.
All the children who had bilateral lesions fell into the poor outcome category. One was in the small lesion category, one in the moderate lesion category, and two were in the large lesion category. Both the children who died had large lesions.
All of the seven children with small lesions and poor outcome had lesions that involved the basal ganglia. Five of them had lesions confined to these structures.
As a group, children with symptomatic stroke (those with a previous risk factor) had larger lesions then those with idiopathic stroke (χ2, p = 0.02). However, this was not predictive of a worse outcome.
Discussion
Our findings indicate that, in children with MCA territory infarcts, although the functional sequelae of small lesions might be variable, infarction of more than 10% ICV is associated with pronounced residual deficits.
There are methodological constraints inherent in measuring infarct volumes in the manner described here. The reproducibility of measuring individual volumes in the our study was compromised by subjectively defining the lesion boundaries, both in the acute and chronic stages. This was especially difficult in the case of small lesions, as is apparent from the data presented in table 2, where relatively small absolute differences in measurement resulted in large percentage differences in repeated measurements. In contrast, the reproducibility of the ICV measurements was good.
The natural history of cerebral infarction on MRI is for signal hyperintensity and swelling on T2 weighted images to be apparent around six to 12 hours after symptom onset.11 Chronic infarcts show signal hyperintensity and tissue atrophy on T2 weighted imaging. In the early stages of evolution of a cerebral infarct, tissue swelling makes definition of lesion boundaries difficult; in more chronic lesions, atrophy may cause similar problems. Although automated or semi automated image analysis techniques might improve reproducibility,3 12 the accuracy with which such techniques measure the true volume of damaged tissue is questionable. Moreover, absolute values for infarct volume at any stage in the lesion’s evolution must be viewed with some scepticism because early measurement might overestimate and late measurement might underestimate the actual volume of damaged tissue. Because swelling is more apparent around large lesions than small ones, lesion size might also be an important factor determining the variation in individual lesion volumes during the evolution of the lesion. Our patients comprised a heterogeneous group in terms of the timing of imaging in relation to the neurological insult. Although most of them were imaged acutely, in a few cases there was an interval of several years between the event and the MRI study. However, as we were studying the relative rather than the absolute effects of lesion volume on outcome (by categorising lesions into small, moderate, and large), we believe that inclusion of all the patients was valid.
In a recent study examining the relation between lesion volume and outcome in adults with cortical MCA territory stroke, Saunders and colleagues3 showed a significant relation between lesion volume on T2 weighted MRI obtained within 72 hours of the onset of symptoms and outcome. The population in this study was relatively elderly (mean age, 66.5 years) and of the nine patients who died, none appear to have died as a direct result of the stroke (although at least two died of secondary illnesses, such as pulmonary embolism). Compared with this group, our patients formed a more heterogenous group, which included patients with purely subcortical infarction, and death or disability were more directly attributable to the acute stroke.
Lovblad and colleagues12 found that in adults with MCA territory infarction, the volume of lesions on T2 weighted MRI at a chronic time point correlated well with indices of stroke severity and functional outcome. Although that study included some patients with purely subcortical lesions, these associations were stronger in the subgroup of patients with cortical MCA lesions. It was noted that the correlation between lesion size and clinical status was less for smaller lesions than for large ones. The relative frequency of small, subcortical lesions in our study might partly account for the discrepancies between our findings and those of Lovbladet al. The methodological difficulties discussed previously might also have some bearing on this. Comparison of our results with those of the two studies above, however, must also take into account the differing effects of basal ganglia injury in adults and children, as discussed below.
Unlike adult stroke patients, in whom the profile of risk factors is relatively homogenous, children who suffer ischaemic stroke are a heterogeneous group. Symptomatic stroke or stroke in children with a pre-existing medical condition (such as congenital heart disease) has been reported to previously be a risk factor for poor outcome.4 6 7 Although this might be associated with factors relating to the underlying diagnosis (such as chronic hypoxia) it is noteworthy that these children tended to have larger lesions. Compensatory mechanisms might be less efficient in children whose cerebral perfusion is under chronic stress. In children with cardiac disease, embolic occlusion might cause occlusion of arterial trunks, resulting in larger lesions. However, as is apparent from our data, the relation between the presence of a risk factor for stroke and lesion size, lesion location, and outcome is not a simple one. Neurological co-morbidity from the pre-existing risk factor needs to be considered; however, given the small numbers of patients in our study we were unable to examine these questions in further detail.
Idiopathic ischaemic stroke in childhood has been reported previously to be confined frequently to basal ganglia structures.4 In our group, 15 of the 27 patients without previous medical diagnoses had lesions confined to the basal ganglia, without cortical involvement. Five of them had had chickenpox within the six months preceding the stroke; the relation between preceding varicella and basal ganglia infarction in childhood has been described elsewhere.13
We found that some children with relatively small lesions confined to the basal ganglia had pronounced residual deficits. Unlike adult patients, children have been shown to develop residual dystonia after basal ganglia infarction.4 14 15 Hand function tends to be the worst affected, although progressive dystonia can lead to more generalised disability. Previous reports suggest that striatocapsular infarction in adults might be associated with pronounced cognitive and motor sequelae.16 17 There is also evidence that language function,18 behaviour, and attention19 might be affected in children with subcortical lesions. Although striatocapsular infarction is a relatively common pattern in childhood stroke, its psychometric correlates have not been explored in detail. Our data suggest that the residual sequelae after basal ganglia infarction can lead to pronounced functional impairment and support more detailed characterisation of this group of patients.
Although, anecdotally, outcome after stroke in childhood is thought to be good, it is clear from previous publications that most children are left with residual deficits and that there is an appreciable mortality.20 21 This argues for a role for acute stroke treatments in the prevention of disability in the paediatric stroke population. The recent trials of acute stroke treatments in adults have shown that very large numbers of patients are required to evaluate treatments that have a finely balanced risk–benefit ratio. Although the estimated incidence of ischaemic stroke in childhood varies widely from 0.6 to 8/100 000/year,20 21 compared with ischaemic stroke in adults (which has an incidence of 180/100 000/year22) patient numbers are small. Some means of categorisation of patients into prognostic groups would facilitate trials of treatment in smaller groups of patients.
In our group of patients, infarction of more than 10% of the ICV was associated with pronounced disability or death in all cases. This suggests that a threshold exists for lesion size, above which outcome is universally poor. The clinicopathological stroke syndrome of “malignant middle cerebral artery infarction” is characterised by large MCA territory infarcts. This has been shown to have a very poor prognosis in adult patients.23 24 It appears from our study that a similar clinicopathological syndrome is identifiable in children. Our data suggest that by combining information from lesion volume and topography, a group of children with ischaemic stroke who would be predicted to have poor outcome could be identified and enrolled in future therapeutic trials.
Acknowledgments
We thank the Wellcome Trust for financial support.