Article Text

Abstract
We report the clinical course, and neurophysiological and neuroimaging findings of a patient with Guillain-Barré syndrome associated with central nervous system lesions. During a course of intravenous immunoglobulin therapy, she had headache with meningism. Cerebral magnetic resonance imaging showed lesions in both frontal and right occipital lobes. Cerebrospinal fluid showed a raised protein concentration accompanied by mild pleocytosis. Her symptoms resolved within two months. Subsequent magnetic resonance imaging revealed cavity formation in the deep white matter and atrophic changes in the right occipital lobes.
- Guillain-Barre syndrome
- central nervous system
- immunoglobulin
- CNS, central nervous system
- CSF, cerebrospinal fluid
- CT, computed tomography
- DL, distal latency
- GBS, Guillain-Barré syndrome
- MCV, motor conduction velocity
- MRI, magnetic resonance imaging
Statistics from Altmetric.com
- CNS, central nervous system
- CSF, cerebrospinal fluid
- CT, computed tomography
- DL, distal latency
- GBS, Guillain-Barré syndrome
- MCV, motor conduction velocity
- MRI, magnetic resonance imaging
Guillain-Barré syndrome (GBS) is an acute demyelinating polyneuropathy presumably related to immunological mechanisms. The central nervous system (CNS) is usually intact in patients with GBS. However, there have been some reports of an association of GBS with CNS involvement.1–7 We report the clinical course, and neurophysiological and neuroimaging findings of a patient with GBS associated with distinctive CNS lesions.
CASE REPORT
A previously healthy 9 year old girl was admitted to Kamo Hospital because of progressive ascending weakness, beginning five days before admission. On admission, she was alert but could not stand up. Deep tendon reflexes were absent in all extremities. Head computed tomography (CT) was normal; cerebrospinal fluid (CSF) showed cell count of 1×109/l and 89 mg/dl protein. Motor and sensory nerve conduction velocity remained normal.
She was treated with intravenous immunoglobulin (400 mg/kg for five days), but did not improve. She complained of headache accompanied with meningism on the fourth day of immunoglobulin administration. Cerebral CT on the next day revealed low density areas in the right occipital area. She was transferred to our hospital.
On admission, she was alert with notable generalised weakness. She could not sit with support. Deep tendon reflexes were absent in all extremities. Cerebral magnetic resonance imaging (MRI) revealed lesions in both frontal and right occipital lobes, which showed low intensity on T1 weighted image and high intensity on T2 weighted image (fig 1). Magnetic resonance angiography was normal. We firstly suspected acute disseminated encephalomyelitis, but a nerve conduction study on the next day showed remarkable reduction of motor conduction velocity. CSF showed 40×109/l lymphocytes, no erythrocytes, and 3.56 g/l protein. GBS with CNS involvement was diagnosed.
{kind=link}
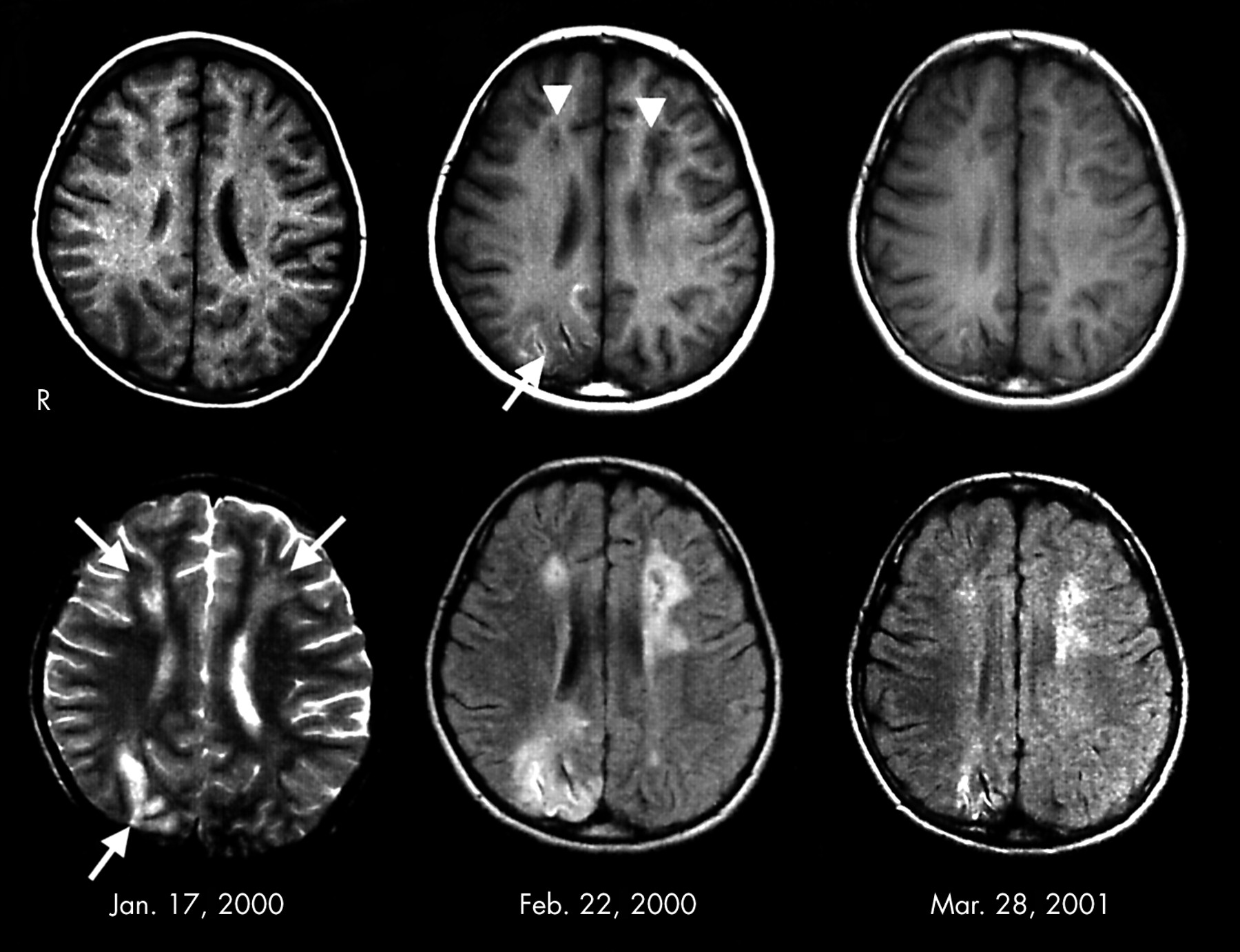
MRI findings. Left: MRI on admission. T2 weighted image (lower) showed high intensity areas in the deep white matter in the bilateral frontal lobes, and in the cortex and subcortex in the right occipital lobe (arrows). T1 weighted image (upper) showed low intensity areas in the corresponding place. Middle: MRI one month after admission. T1 weighted image (upper) showed cavity formation in the deep white matter in the bilateral frontal lobes (arrowheads). Abnormal low intensity was recognised in the cortex and subcortex in the right occipital lobe (arrow). Fluid attenuated inversion recovery image (lower) showed high intensity areas around the cavity formations. Right: MRI one year after discharge. The size of cavity and the extent of abnormal high intensity areas were remarkably reduced.
Her symptoms gradually resolved. She could sit with support four weeks after admission and could walk for a long distance eight weeks later. No recurrence was seen during two years follow up.
LABORATORY EVALUATIONS
Serum anti-GM1 and anti-GQ1B antibodies were negative on admission. Stool culture yielded no growth. CSF concentration of myelin basic protein was 0.6 ng/ml (reference concentration <0.1 ng/ml) on admission. Oligoclonal bands were not recognised in her CSF.
NEUROPHYSIOLOGICAL STUDIES
The initial motor conduction velocity (MCV) remained normal. However, reduction of MCV and prolonged distal latency (DL) were observed in the median (MCV 31 m/s, DL 11.6 ms), ulnar (28 m/s, 10.0 ms), and tibial nerves (34 m/s, 7.5 ms) on admission. Absent F waves were also recognised in the median and tibial nerves. MCV became normal four weeks after admission. Sensory conduction velocity remained normal throughout.
Electroencephalography on admission showed mild slowing of background activities without paroxysmal discharges. It became normal at discharge. Pattern reversal visual evoked potentials showed mildly prolonged N2 latency and abnormal waveforms on admission. Visual evoked potentials were normalised within one year after discharge. Brain stem auditory response and somatosensory evoked potentials were unremarkable.
NEUROIMAGING
MRI on admission showed multiple lesions in the cortex and subcortex in the right occipital lobe and in the deep white matter in both frontal lobes (fig 1). These lesions were not enhanced by paramagnetic contrast infusion. MRI one month after admission showed cavity formation in the deep white matter and atrophic changes in the right occipital lobe. Fluid attenuated inversion recovery image showed high intensity areas around these lesions. The size of the cavity and the extent of high intensity areas were remarkably reduced one year after discharge.
DISCUSSION
GBS is regarded as a predominantly motor neuropathy with few sensory features. Although the CNS is rarely involved, GBS associated with CNS manifestations has been described in children,1,2,4 as well as adults.3,5–7 Gamstorp reported an 8 year old girl with GBS by with unconsciousness, oscillating eye movement, and convulsions, and proposed the term “encephalomyeloradiculoneuropathy”.1 Amit et al described a 10 year old girl with GBS associated with deep coma.4 Contrast enhanced CT displayed multifocal enhancement of the white matter. In our patient, MRI showed multiple CNS lesions, not only in the periventricular white matter, but also in the occipital cortex and subcortex. It is interesting that CNS manifestations were not evident in our patient, although the previously reported patients always had CNS symptoms, such as reduced consciousness, seizure, or brain stem impairment.1,4–7 This implies that an association of CNS involvement in patients with GBS could be underestimated because some lesions can be clinically silent.
Mild pleocytosis was observed in the second lumbar tap in our patient. We consider this pleocytosis attributable to intravenous immunoglobulin. Aseptic meningitis is a common complication of intravenous immunoglobulin therapy. We consider her headache with meningism was attributable to intravenous immunoglobulin, although these symptoms can be a clinical manifestation of GBS itself.8 Another explanation is that pleocytosis may be related to CNS lesions. CSF pleocytosis is often seen in patients with demyelinating CNS disorders such as multiple sclerosis.
There are some possible explanations for the pathogenesis of CNS lesions in our patient, including watershed infarction, demyelination, reversible posterior leucoencephalopathy, and adverse effects of immunoglobulin. With regard to watershed infarction, there was no clinical event that could cause ischaemic brain damage. Given that extensive CNS lesions seen in our patient were watershed infarction, it is not likely to be clinically silent. Raised CSF myelin basic protein indicated the demyelinating nature of CNS lesions in our patient. Some authors have discussed the possibility of shared pathogenic central and peripheral nervous system epitope.3,6 Several animal studies reported peripheral nervous system lesions in experimental allergic encephalitis,9,10 as well as central nervous injury induced by peripheral nerve antigen.11,12 Reversible posterior leucoencephalopathy may be another explanation for CNS lesions in our patient. Reversible posterior encephalopathy is often associated with a condition in which blood pressure rises acutely.13,14 Patients with this syndrome often have seizures, consciouness loss, or visual disturbance. On the other hand, our patient lacked apparent hypertension or CNS symptoms, and MRI lesions were asymmetric. Intravenous immunoglobulin itself could have been a cause of CNS lesions in our patient. There have been previous reports of encephalopathy associated with intravenous immunoglobulin treatment in patients with GBS.7,15–17 Although hyperviscosity or vasospasm have been suggested to be related to the development of encephalopathy in those patients, its pathogenesis has not been clarified.
In summary, we report a patient with GBS associated clinically silent CNS lesions. Such cases have been reported rarely, but our experience suggests that the association of CNS lesions with GBS may be underestimated.