Article Text

Abstract
Objective Guidelines state that verapamil is contraindicated in infants. This is based on reports of cardiovascular collapse and even death after rapid intravenous administration of verapamil in infants with supraventricular tachycardia (SVT). We wish to challenge this contraindication for the specific indication of verapamil sensitive ventricular tachycardia (VSVT) in infants.
Design Retrospective case series and critical literature review.
Setting Hospitals within New Zealand.
Patients We present a series of three infants/young children with VSVT or ‘fascicular VT’.
Results Three children aged between 8 days and 2 years presented with tachycardia 200–220 beats per minute with right bundle brunch block and superior axis. Adenosine failed to cardiovert and specialist review diagnosed VSVT. There were no features of cardiovascular shock. Verapamil was given as a slow infusion over 10–30 min (rather than as a push) and each successfully cardioverted without incident. Critical review of the literature reveals that cardiovascular collapses were associated with a rapid intravenous push in cardiovascularly compromised infants and/or infants given other long-acting antiarrhythmics prior to verapamil.
Conclusions Verapamil is specifically indicated for the treatment of fascicular VT, and for this indication should be used in infancy, as well as in older children, as first-line treatment or after failure of adenosine raises suspicion of the diagnosis. We outline how to distinguish this tachycardia from SVT and propose a strategy for the safe intravenous slow infusion of verapamil in children, noting that extreme caution is necessary with pre-existing ventricular dysfunction.
- arrhythmia
- ventricular tachycardia
- ECG
- infant
- calcium channel blocker
- safety
- contraindication
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Fascicular ventricular tachycardia (VT) is also known as verapamil-sensitive VT because it is uniquely sensitive to verapamil, and will not be cardioverted by other antiarrhythmics.
Features of fascicular VT are: right bundle branch block, superior or right axis deviation, ventriculoatrial dissociation (sometimes) with fusion or capture beats.
Guidelines state that intravenous verapamil is contraindicated in infants due to fear of cardiovascular collapse with a rapid intravenous push.
What this study adds?
This report reminds us that fascicular VT is different from supraventricular tachycardia and requires different management irrespective of age.
Verapamil is effective in terminating fascicular VT and can be used safely in young children, including infants with preserved ventricular function when infused slowly with careful monitoring—this is particularly important if tachycardia has been ongoing for a long time and there is suspicion of depressed myocardial function—we propose infusion of 0.1 mg/kg over at least 10 min.
Calcium should be available at the bedside and concomitant use of atrioventricular blocking agents like beta blockers or digoxin should be avoided.
Introduction
It is generally accepted that intravenous administration of the calcium antagonist verapamil for the treatment of tachyarrhythmias is contraindicated in children under 1 year of age due to a proven risk of haemodynamic collapse and even death in young children. Verapamil is a negative inotrope, and the myocardium of very young children, in particular neonates, may be especially sensitive to changes in intracellular calcium concentrations and the blockade of calcium channels based on knowledge from animal studies.1–3 The first reports of cardiovascular collapse after intravenous administration of verapamil in young infants were published in the mid-1980s. Epstein et al reported three cases of cardiovascular collapse in infants aged 2–6 weeks.4 Based on this case series and a handful of other case reports and small series,5–7 best practice guidelines now state that intravenous verapamil is contraindicated in infants for the treatment of supraventricular tachycardia (SVT) and fascicular ventricular tachycardia (VT).8 With the arrival of adenosine, verapamil disappeared from use in this age group. Nevertheless, calcium channel blockers are uniquely effective as the treatment of fascicular VT, to the point that this arrhythmia is also known as ‘verapamil sensitive ventricular tachycardia’. It typically occurs in children and young adults without structural heart disease.9–14 The underlying mechanism is believed to be a re-entry tachycardia involving the Purkinje fibres of the fascicles—typically the left posterior fascicle of the left bundle branch but also has features of an automatic tachycardia, can be incessant, unresponsive to direct current cardioversion and may lead to cardiomyopathy.
Fascicular VT has been classified into three types:
Left posterior fascicular VT with right bundle branch block (RBBB) and superior axis deviation.
Left anterior fascicular VT with RBBB and right axis deviation.
High septal VT with normal QRS duration and normal frontal axis plane.
Left posterior fascicular VT makes up about 90% of cases, followed by left anterior fascicular VT. High septal VT has not been described in young children.
Fascicular VT in young children is much less common than SVT but its detection is important because it does not respond to adenosine, nor amiodarone. Intravenous verapamil terminates the tachycardia in 93% of cases in children.15 The reported cases of collapse in infants were associated with a rapid intravenous push of verapamil. Our experience is that a slower infusion is effective and safe in infants for this specific indication, when it is clear there is no circulatory compromise prior and no more than mild left ventricular (LV) dysfunction. We present three illustrative cases, review the literature and suggest a strategy for the safe treatment of such cases.
Case presentation
Research Governance Committee approval for this report was obtained from Auckland and Waikato District Health Boards, along with consent from each family.
Case 1
An infant presented in the first 3 months of life to the emergency department with 4 days of increased work of breathing, 2 days of cough and on presentation a tachycardia of 220 beats per minute (bpm) with a superior axis and RBBB presumed to be SVT. Ice dunk and four doses of intravenous adenosine to a maximum dose of 500 mcg/kg were unsuccessful. The remote on-call paediatric cardiologist diagnosed verapamil sensitive or fascicular VT from the 12-lead ECG (figure 1A).

(A) ECG of patient 1 on arrival. This shows a tachycardia at about 220 bpm with a superior axis and right bundle branch block. There are no capture beats but ventriculoatrial (VA) dissociation is visible, proving this to be ventricular tachycardia (VT) and not supraventricular tachycardia (SVT) with aberrancy. Superior axis and right bundle branch block (RBBB) make this the most common form of fascicular VT; left posterior fascicular VT. (B) ECG after conversion to sinus rhythm with intravenous verapamil. This shows a normal axis and no fascicular block. This indicates involvement of the posterior fascicle as retrograde limb in the tachycardia circuit.
The patient remained in the emergency department and verapamil 0.1 mg/kg was infused over 20 min in presence of the neonatal intensive care and emergency department consultants with a resuscitation dose of calcium drawn up at the bedside. After a few minutes the tachycardia reverted to sinus rhythm (figure 1B) and all vital signs including blood pressure (BP) remained stable. After overnight observation in the intensive care unit (ICU), the patient was started on oral verapamil the following day and discharged home. An echocardiogram prior to discharge demonstrated a structurally normal heart with normal systolic function.
Case 2
An 8-day-old term baby presented to hospital for a planned review for an antenatally diagnosed muscular ventricular septal defect. The infant was found to be tachycardic (200 bpm) and tachypnoeic at the time of the echocardiogram. The mother reported that tachypnoea began 48 hours prior with increased sweatiness for 24 hours though the baby was still breast feeding satisfactorily. On admission to the neonatal ICU clinical signs and chest X-ray changes were consistent with mild cardiac failure but preserved peripheral perfusion. The echocardiogram showed a small muscular ventricular septal defect and mildly impaired LV systolic function. A dose of furosemide and empiric antibacterial treatment was given. The ECG demonstrated a broad complex tachycardia at a rate of 195 bpm with a superior axis and RBBB. Intravenous adenosine was ineffective four times to a maximum dose of 250 mcg/kg. The on-call paediatric cardiologist reviewed the 12-lead ECG remotely and diagnosed of fascicular VT. A resuscitation dose of calcium gluconate was drawn up and available at the bedside during the verapamil infusions but was not required. A dose of 0.05 mg/kg of intravenous verapamil infused over 30 min did not revert the tachycardia so a second dose of 0.05 mg/kg was given over 30 min and the tachycardia reverted to sinus rhythm 15 min into the infusion. Oral verapamil (1 mg/kg/dose three times a day) was started 4 hours after the end of the infusion. Two further episodes of VT within the next 12 hours reverted with infusions of the same dose of verapamil. The BP remained stable throughout.
Case 3
A 2-year-old child was referred to a hospital by the general practitioner for a tachycardia and a short history of lethargy, a single vomit and the mother having noticed a fast heartbeat. The heart rate was 199/min on presentation and the respiratory rate was 77/min. The ECG was presumed to show SVT and ice was administered to the patient’s forehead followed by increasing doses of intravenous boluses of adenosine with no effect. The ECGs (figure 2A,B) were reviewed remotely by the on-call paediatric cardiologist and fascicular VT was diagnosed. An echocardiogram demonstrated normal cardiac size and systolic function. An infusion of 0.2 mg/kg of verapamil was started in the resuscitation bay of the emergency department (with calcium available), but was stopped after 0.1 mg/kg after cardioversion to sinus rhythm. BP was stable. A further 0.1 mg/kg of verapamil was infused slowly for a recurrence of the tachycardia 3.5 hours later. The tachycardia reverted within 2 min. For several recurrences of fascicular VT overnight a total of 0.2 mg/kg of verapamil was given as fractionated slow infusions of 1.66 mcg/kg/min (0.1 mg/kg/hour). The oral maintenance dose was increased to 2 mg/kg three times a day and the child was discharged home after a few days of observation without recurrence of tachycardia. Further recurrences of tachycardia at 5 months and 1 year were successfully treated with slow intravenous verapamil infusions followed by an increase of the regular oral dose.
{kind=link}
{kind=link}
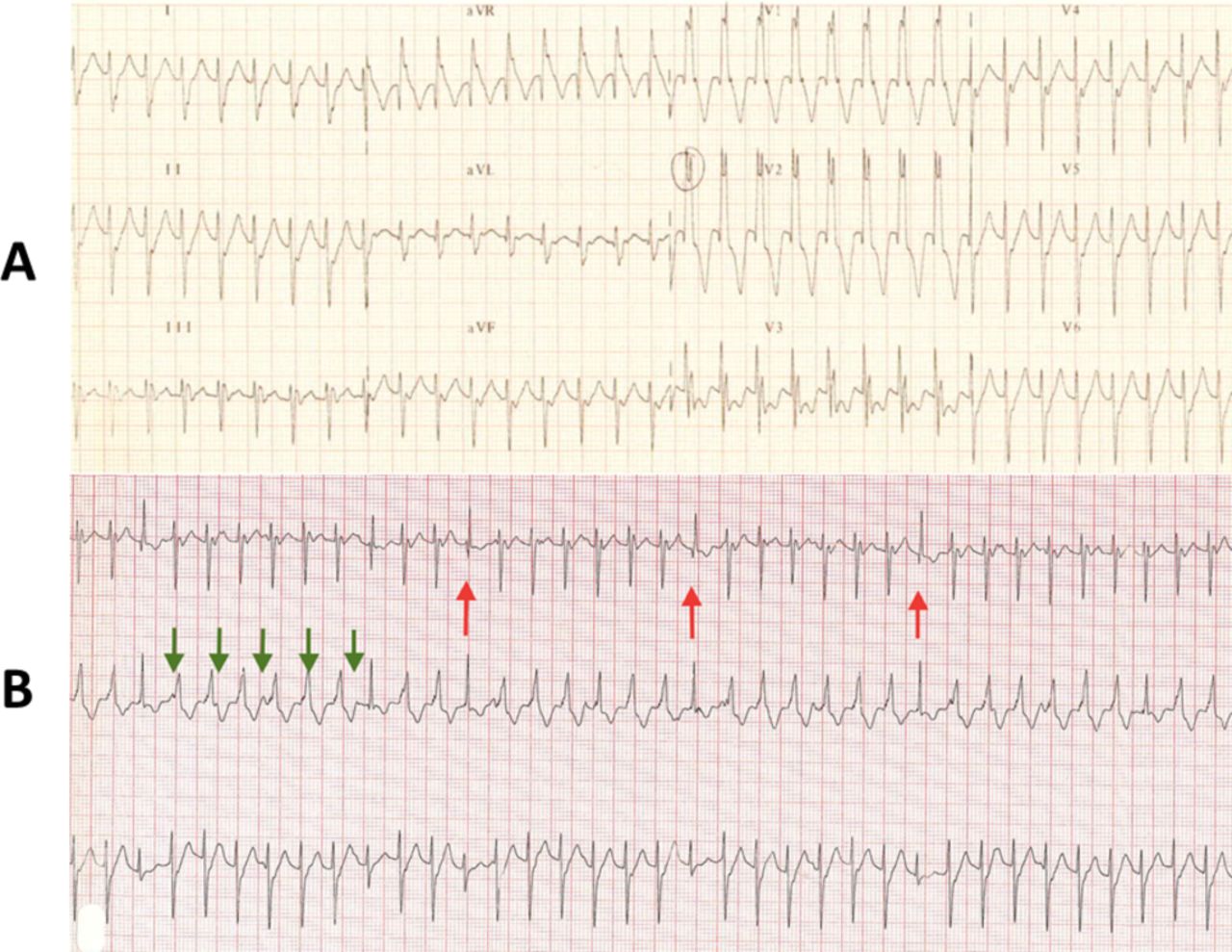
(A) ECG on presentation in the 2-year-old child. It demonstrates tachycardia at 194 bpm with right bundle branch block (RBBB) and superior axis deviation. (B) Three-lead rhythm strip from case 3: this demonstrates ventriculoatrial (VA) dissociation and capture beats proving that this is ventricular tachycardia. Green arrows mark P waves and red arrows mark capture beats.
Discussion
This case series of more than nine intravenous infusions of verapamil in three small children, including two infants, shows that verapamil can be used safely and effectively for the treatment of fascicular VT in haemodynamically stable young children and infants. The cases demonstrate that if intravenous verapamil is given slowly the feared side effect of haemodynamic instability and atrioventricular (AV) block may not occur. Given the fact that other treatments are ineffective for fascicular VT, the opinion that the use of intravenous verapamil is contraindicated in infants needs to be challenged for this type of tachycardia.
The recommendation to avoid verapamil in young children is based on very limited evidence but is widely accepted. In the current European Heart Rhythm Association/Association for European Paediatric and Congenital Cardiology arrhythmia working group consensus statement on the management of arrhythmias in the paediatric age group8 verapamil is listed as contraindicated in infants under 1 year of age for the treatment of SVT and fascicular VT, citing the article of Porter et al from 198316 in which two cases of junctional ectopic tachycardia treated with intravenous verapamil responded with hypotension requiring resuscitation with calcium. In that original article intravenous verapamil for treatment of SVT was recommended in all age groups nevertheless. In 2013, Lapage et al published a review titled ‘Verapamil in infants: An exaggerated fear?’ in which they evaluate the limited evidence that has led to the acceptance of infancy as a contraindication for intravenous verapamil.17
In most reported cases of cardiovascular collapse after intravenous verapamil additional risk factors for compromise can clearly be identified, typically long duration of tachycardia with signs of poor cardiac output or congestive heart failure, age <6 weeks, concomitant sepsis or myocarditis, pretreatment with AV nodal blocking agents such as digoxin or beta blockers or inadvertent administration of an inappropriately high dose of verapamil. There is only one report of a child older than 6 weeks who had a complication with an adequate dose of verapamil; this infant also had myocarditis.7 Given the availability of adenosine, it is sensible to avoid intravenous verapamil in infants with SVT, especially those with pre-existing haemodynamic compromise or sepsis. However, Roguin et al reported successful verapamil treatment of SVT in two infants aged 20 days and 6 weeks with the administration of calcium gluconate prior to giving intravenous verapamil. They reported haemodynamic stability and no interference with the antiarrhythmic effect of verapamil.18
There are several reports of successful conversion of fascicular VT in young infants with intravenous verapamil.9–12 19 It is interesting to note that in none of these case reports verapamil was used as a first-line agent. All infants were pretreated either with adenosine, a beta blocker, amiodarone, procainamide, lidocaine or a combination of the above and/or overdrive pacing or synchronised cardioversion. No adverse effects of verapamil were reported. A cardioversion rate for intravenous verapamil of 93% was reported in the largest cohort of paediatric patients with fascicular VT to date.15 No adverse events of verapamil were reported though the study focused on success rates of medical and catheter-based treatments and not adverse events. Moran and Colan reported the haemodynamic effects of intravenous verapamil in a prospective study of children under the age of 2 years with hypertrophic cardiomyopathy.20 Verapamil was administered to 22 patients and invasive haemodynamic measurements were obtained in the cardiac catheterisation laboratory. In 21 patients (mean age 5.8 months with a range of 0.3–23 months) they could document a negative inotropic effect with a fall in cardiac index from 4.6±1.2 to 4.1±0.9 L/min/m2 and a fall in BP by 8 points from a mean of 88±16 to 82±14 mm Hg and a reduction in the left ventricular outflow tract gradient. The acute infusion of 0.1 mg/kg followed by 0.007 mg/kg/min was tolerated by all. One patient who was in the ICU for severe congestive heart failure and labile BP experienced increasing hypotension during the initial infusion but a later trial the following day was well tolerated without adverse events. In most reports the usual verapamil dose administered to infants with SVT ranged from 0.1 to 0.2 mg/kg with higher doses of 0.3 mg/kg described in older children. Current recommendations for intravenous verapamil state a dose of 0.1–0.2 mg/kg for children.21 22
Based on the available literature, and our own experience, we believe that intravenous verapamil should not be regarded as absolutely contraindicated in infants younger than 1 or 2 years of age in the treatment of fascicular VT. Young infants <6 weeks of age or infants with significant myocardial dysfunction are at increased risk of adverse events during administration of intravenous verapamil and extreme caution is required in this group. We propose that for young infants verapamil should be administered by slow intravenous infusion at a dose of 0.1 mg/kg over at least 10 min, repeated to a total of 0.2 mg/kg, rather than by intravenous bolus, and that calcium be available at the bedside. Close monitoring in an emergency room or intensive care setting is essential. Careful clinical examination of the infant, blood gas analysis and echocardiographic assessment should be employed prior to drug administration, and if abnormal, concurrent inotropic support, and transfer to a tertiary centre with potential extracorporeal membrane oxygenation (ECMO) backup should be considered in these cases.
Conclusion
Fascicular VT is rare in infants but needs to be differentiated from SVT because of the treatment implications. If adenosine is not effective in reverting presumed SVT, this diagnosis should be considered.
Identifying features of fascicular VT are RBBB, superior or right axis deviation, ventriculoatrial dissociation (though not always present) and fusion or capture beats.
Intravenous verapamil can be used safely as first-line treatment for fascicular VT in young children with preserved ventricular function. It should be given as a slow infusion of 0.1 mg/kg/dose over at least 10 min with close monitoring and calcium should be available for resuscitation. If there are features of low cardiac output or ventricular function is more than mildly impaired on echocardiography, transfer to a tertiary care facility is recommended, where circulatory support (including ECMO) should be immediately available.
Acknowledgments
The authors gratefully acknowledge Charlene Nell for assistance with manuscript preparation from the Department of Cardiovascular Services, Green Lane Cardiovascular Services, Auckland City Hospital, Auckland, New Zealand
References
Footnotes
Contributors JK and JS conceptualised this article and drafted the initial manuscript. AB, FM and TH identified the cases presented, supplied the relevant clinical information and reviewed the article for accuracy. They also revised it critically for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval The Research Governance Committee approval for this report was obtained from Auckland and Waikato District Health Boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Next of kin consent obtained.