Article Text

Abstract
AIMS To evaluate the efficacy and safety of the Ahmed glaucoma valve implant in Chinese eyes with complicated glaucomas.
METHODS This retrospective study reviewed the final intraocular pressure, visual outcome, and incidence of complications in all patients with the Ahmed glaucoma valve implant performed at the Prince of Wales Hospital, Hong Kong, between June 1996 and November 1998.
RESULTS A total of 65 eyes from 60 patients were treated with the Ahmed glaucoma implant. At a mean follow up (SD, median) of 21.8 (9.2, 28.0) months (range 6–37 months), the mean intraocular pressure was reduced from 37.0 (SD 12.1) mm Hg before the implant surgery to 16.1 (12.4) mm Hg at the last follow up after surgery. The success rate of intraocular pressure control of <22 mm Hg was achieved in 73.8% of operated eyes. Transient postoperative hypotony with shallow anterior chamber occurred in 10.8% of cases. The most common postoperative complication was the formation of encapsulated bleb (24.6%).
CONCLUSIONS The Ahmed glaucoma valve implant appears to be effective and relatively safe for treating complicated glaucomas in Chinese eyes. The success rate is comparable with those reported in non-Asian eyes. Formation of postoperative encapsulated bleb is, however, more commonly encountered.
- Chinese
- glaucoma
- glaucoma drainage device
Statistics from Altmetric.com
Glaucoma drainage devices (GDD) provide an alternative treatment in complicated and refractory glaucoma cases.1-6 A GDD with valve is designed to reduce the incidence of postoperative hypotony. The Ahmed glaucoma valve (AGV) implant (New World Medical, Rancho Cucamonga, LA, USA) was introduced in 1993. It has a built in Venturi valve, which offers a set resistance to the aqueous outflow. A folded silicone elastomer membrane forms the valve with its free edge forming a one way outlet. The valve will open at a specific level of intraocular pressure (IOP), thus reducing the chance of hypotony in the early postoperative period.7Initial clinical experiences with this implant have demonstrated that postoperative hypotony was less common than the non-valved GDD.8 However, the valve may be a potential site for obstruction by inflammatory debris,9 especially in Asian eyes that are known to have more severe tissue reactions than white people.10 11 Aung and Seah reported good outcome of GDD in Asian eyes. However, the GDD used in their series were non-valved (Baerveldt and Molteno glaucoma implants).12 Huang and associates reported good effectiveness of the AGV implant in their series but the majority of their patients were non-Asian and racial difference was not taken into account in their risk factor analysis.13 Only little information regarding the safety and efficacy of the valved glaucoma drainage implant in the treatment of refractory glaucoma in Chinese eyes is available in the literature. This retrospective study aims at reviewing the surgical outcome in terms of the IOP, visual acuity, and incidence of complications in all patients receiving AGV implant surgery at the Prince of Wales Hospital, Hong Kong, between June 1996 and November 1998.
Patients and methods
A retrospective review of the records of all patients who received AGV implant surgery for glaucomas not responsive to medical and non-implant surgical treatments in the specified period was performed. All surgeries were performed by two of us (JSL and DSL) and no other GDD were used during the study period.
The superotemporal quadrant was used for the implant fixation in all eyes. For aphakic patients, anterior vitrectomy was performed before AGV implant was fixed. A fornix based conjunctival flap and Tenon capsule was dissected to allow insertion of the plate of the implant into the sub-Tenon space 8 mm behind the corneal limbus. Before insertion of the plate, the valve of the implant was primed by irrigating the lumen of the tube with balanced salt solution (BSS, Alcon, Fort Worth, TX, USA). The plate was fixed to the sclera with two 9-0 black nylon sutures (Ethicon, Ethilon). The tube was shortened to the desired length with its sharp bevel facing anteriorly. An anterior chamber (AC) paracentesis wound was created at the peripheral cornea and sodium hyaluronate 1% (Healon, Pharmacia and Upjohn) was injected to prevent sudden collapse of the AC when the sclerostomy was made. The tube of the implant entered the AC parallel to the iris plane through the sclerostomy made with a 23 gauge syringe needle. The tube was fixed to the sclera with one 9-0 black nylon suture. The anterior part of the tube was covered with a donor corneoscleral graft, which was then fixed to the sclera with 10-0 black nylon sutures. The conjunctiva was closed with 8-0 Vicryl sutures. The sodium hyaluronate in the AC was removed as much as possible through the paracentesis site. No adjunctive antimetabolite was used in any of the cases.
Topical 0.3% ofloxacin (Tarivid, Santen, Osaka, Japan) and 1% prednisolone acetate eye drops (Pred Forte, Allergan, Irvine, CA, USA) were given four times daily for 6 weeks. Postoperative examination included visual acuity test, IOP measurement using the Goldmann applanation tonometer, detailed slit lamp and fundus examination on day 1 and regularly as indicated thereafter. Extraocular movement was examined and diplopia symptoms were specifically asked for.
Absolute success in IOP control was defined as IOP less than 22 mm Hg and greater than 5 mm Hg without medication. Qualified success was defined as IOP less than 22 mm Hg and greater than 5 mm Hg with the use of antiglaucomatous medication(s). Failure in IOP control was defined as IOP equal to or greater than 22 mm Hg on maximally tolerated medications or those who required re-implant or cyclodestructive procedures. Hypotony was defined as IOP less than 5 mm Hg on any single visit.
Results
A total of 65 eyes from 60 patients with complicated glaucomas not responsive to conventional medical and non-implant surgical treatments received AGV implant surgery at the Prince of Wales Hospital during the period from 1 June 1996 to 30 November 1998. The follow up period ranged from 6 to 37 months with a mean (SD, median) of 21.8 (9.2, 28.0) months.
Sixty four eyes were from Chinese patients and one eye was from a white patient. The mean age was 49.9 (21.2) years (range 1–86). There were 25 females and 35 males. The characteristics of the patients and the preoperative diagnosis are summarised in Table 1. The most common diagnosis was neovascular glaucoma (NVG) (33.8%).
Characteristics of patients and preoperative diagnosis
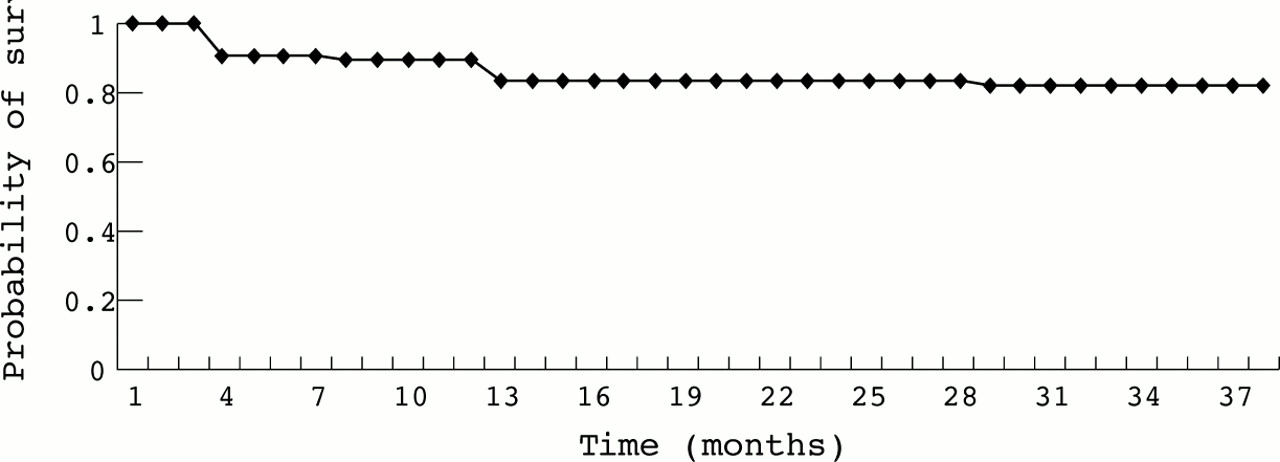
The mean preoperative IOP was 37.0 (SD 12.1) mm Hg. Postoperatively, the mean IOP was decreased to 13.2 (10.3) mm Hg on day 1, 18.4 (10.7) mm Hg at 3 months, and 18.0 (14.1) mm Hg at 1 year of follow up (89.2% eyes ⩾1 year follow up). The absolute success rate for IOP control was 43.1% and qualified success rate 30.7% at the most recent follow up (mean 21.8 (SD 9.2), median 28.0 months). The Kaplan-Meier survival curve shows the probability of success with time (Fig 1). The mean IOP was maintained at 16.1 (12.4) mm Hg (Fig 2). There was no statistically significant difference between the preoperative IOPs in the successful group and the failure group (p = 0.737) (two tailed Student'sttest).

Kaplan-Meier curve showing probability of survival with time.

{kind=link}
{kind=link}
Scattergram of the preoperative versus the final intraocular pressure (IOP). The line of equivalence is also shown.
The final best corrected visual acuity improved by more than one Snellen line in nine (13.8%) and decreased by more than one Snellen line in 14 (21.5%) eyes. Of the 14 eyes who had worse visual acuity compared with the preoperative level, six actually became no light perception. All these six eyes had vague light perception before the operation and with progressive diabetic retinopathy or uncontrolled IOP. One of these blind eyes had caused intractable pain to the patient and the eye was enucleated. Two of these blind eyes became phthisical. The main causes for the decrease in vision in the remaining patients were progressive cataract and bullous keratopathy. Only one was due to the uncontrolled glaucoma.
No significant intraoperative complications were encountered in all patients under review. Postoperative complications occurred in 35 (53.8%) eyes. Some eyes had more than one complication (Table 2). The common postoperative complications encountered in this study were encapsulated bleb (24.6%). Eyes with encapsulated bleb had persistently raised IOP for more than 10 weeks postoperatively and the bleb was distended with the overlying conjunctiva tightly stretched over it. The mean time (SD, median) for the development of encapsulated bleb was 3.8 (2.5, 3.0) months. Ten of them received needling with mitomycin C procedure as previously described by us.14 Six had surgical excision of the fibrous tissue. The IOP was successfully controlled after intervention in 14 of them. Other complications included hyphaema (13.8%), corneal decompensation (12.3%), and shallow AC with hypotony (10.8%). Eight of the nine eyes (13.8%) with hyphaema had NVG and one was on long term aspirin. The hyphaema settled spontaneously in all cases without surgical intervention. Two eyes also developed vitreous haemorrhage on subsequent follow up because of progressive proliferative diabetic retinopathy. Closed vitrectomy and endolaser treatments were performed for the persistent vitreous haemorrhage and diabetic retinopathy. Postoperative shallow AC and hypotony developed in seven eyes (10.8%). Reformation of AC was performed in two of them. Choroidal detachment also occurred in these seven eyes. All of them except one resolved spontaneously without suprachoroidal fluid drainage. Corneal decompensation was also a common postoperative complication in this study (12.3%). The cause of the corneal decompensation could be the result of tube endothelial touch, prolonged high IOP, pre-existing endothelial pathology, or a combination of the three. Three patients had the tip of the tube touching the cornea and one touching the iris. Repositioning was performed in all of them. Tube obstruction occurred in four patients; two by blood clot, one by vitreous, and one by iris tissue. The obstructions were successfully cleared by tube irrigation, anterior vitrectomy, and repositioning of the tube respectively. Migration of the whole implant with tube extrusion from the AC during the early postoperative period occurred in four patients necessitated removal. These belonged to the first 20 patients operated in this series when the two surgeons were going through their learning curves. Broken and improperly anchored sutures of the plate were found in all of them. One of these cases also had mild presumed infection around the plate. Although the culture result was negative, there was moderate amount of discharge surrounding the plate. The infection cleared up after the implant was removed. These patients had cyclodestructive procedures performed to control the IOP after removal of the implant. Other reported postoperative complications such as motility disturbance, malignant glaucoma, and pupillary block glaucoma were not encountered in our series.13 15 Obstruction due to malfunction of the built in valve was not observed in any of the case under review. The five explanted AGV implants in our series were examined by irrigating balanced salt solution into their tubes. Normal flow of the fluid through their valves was observed.
Postoperative complications
Discussion
Glaucoma drainage implants have been used successfully for the treatment of complicated glaucomas including NVG; aphakic and pseudophakic glaucoma; glaucomas with multiple filtering procedures; post penetrating keratoplasty glaucoma; paediatric glaucoma; and uveitic glaucoma.1-6 One of the common early postoperative complications is overdrainage resulting in shallow AC, hypotony, and choroidal detachment.16 17 There are various types of glaucoma drainage device available in the market. Some devices have a set resistance mechanism to minimise overdrainage in the early postoperative period. Those without set resistance mechanism may require either a two staged procedure or ligature technique. The AGV implant employs a built in Venturi valve to provide resistance to aqueous flow.7
In our study, the AGV implant was able to decrease the mean (SD) preoperative IOP from 37.0 (12.1) mm Hg to 18.4 (10.7) mm Hg at 3 months and 18.0 (14.1) mm Hg at 1 year postoperatively. The total success (absolute and qualified) rate achieved was 73.8%. Most case series reported success rates between 67% and 94%, depending on the their criteria for success.17 18 The AGV implant used in this study achieved an IOP lowering effect slightly less than that reported by Huang and associates using the same implant in 159 eyes of complicated glaucoma patients.13 Using similar criteria of success, they reported a success rate of 87% at the most recent follow up examination. The IOP lowering effect is also slightly lower than the non-valved glaucoma implant in Asian eyes reported by Aung and associates (85.5%).12 One of the possible reasons is that we have a much higher percentage of cases of NVG. Neovascular glaucoma was the most common preoperative diagnosis (33.8%) in our series and it also carries the highest failure rate in our study (54.5%). No other types of glaucoma were found to have associated with such a high failure rate in our series. It has been well shown that NVG is associated with a much higher risk of failure than other types of glaucoma.13 16 19-21 If we exclude the cases of NVG in our series, the success rate would become 92.3%. On the other hand, we did not demonstrate the level of the preoperative IOP to be a poor prognostic factor for success for the procedure as reported in another study.13 The most common medications used to lower postoperative IOP in our series were topical β blocker and topical carbonic anhydrase inhibitor. They converted 30.7% of the eyes from failure to qualified success.
The rate of early postoperative hypotony was similar to other series of non-valved glaucoma implant (5–16.5%).17 22 23 This may be due to the fact that most surgeons used either a two staged operation or suture occlusion technique in their cases. Another possible explanation is non-functioning of the valve in vivo.24 In a comparison with Huang's series using the same implant, their rate of postoperative hypotony was lower (8%).13 This might be explained by the difference in the definition used. We defined hypotony as IOP <5 mm Hg on any single follow up visit but they defined as IOP <5 mm Hg on two consecutive visits. The AGV implant has the advantage of achieving a lower rate of overdrainage without having to perform a two staged operation or to modify the surgical technique.
The hypertensive phase reported to be as high as 20–40% incidence in other implant series was not distinct in our series.18 25Although the mean IOP at 3 months was slightly higher than that at 1 year, it might have been modified by the medications and the needling procedure with mitomycin C. In fact some of these eyes might be going through the hypertensive phase and did not require needling procedure at all but retrospectively we could not identify which eyes belonged to this group.
Tube erosion through the conjunctiva was uncommon in our study. Only two eyes had erosion of the tube through the patch graft that finally required a regraft. This may be due to the fact that frozen corneoscleral patch graft was used to cover the exposed part of the tube. The corneoscleral rim was obtained from donor graft tissue remnant following corneal transplant. The use of this corneoscleral graft has several advantages. It is cheap and easily available; it possesses high tensile strength and thus offers excellent protection against tube erosion; moreover, the transparent portion of the corneal portion allows direct visual assessment of the patency of the implant tube.26 27
The unique features of our study were the use of one single type of glaucoma implant, the AGV implant, and 98% of our patients were of Chinese ethnic origin. The results in terms of the IOP control, the visual outcome, and the complication rate in our series were satisfactory. The majority of the postoperative complications were transient and resolved either spontaneously or with simple surgical procedures. Only two patients had total blindness directly caused by failure of IOP control by the AGV implant. Although the rate of encapsulated bleb was relatively high in our cases, this complication could be managed with needling and adjunctive mitomycin C.14 The procedure was simple and was performed on an outpatient basis under the slit lamp microscope and the results in our series were encouraging. The frequent occurrence of encapsulated bleb in our studied cases might signify a more aggressive tissue healing process in the Chinese race. Investigations into the prevention of this complication including the use of pharmacological agents or adjunctive measures and better design of the plate of the glaucoma implant might further improve the surgical outcome. In conclusion, the Ahmed glaucoma valve implant is effective and relatively safe for complicated glaucomas in the Chinese population.
Acknowledgments
Financial and proprietary interest: Nil.
Financial support: Supported in part by the Mr W K Lee Eye Foundation and the Mr I K Ho Eye Foundation, Hong Kong.