Article Text

Abstract
Aim: To evaluate tumour angiogenesis as a predictor of prognosis in retinoblastoma.
Methods: This was a retrospective, non-randomised comparative clinicopathological study. The histopathology from 24 cases of Reese-Ellsworth (RE) group V unilateral retinoblastoma treated by enucleation alone was reviewed. Group I consisted of five patients (four RE group Vb and one group Va) who developed disseminated disease at a mean of 10.4 months after enucleation. The remaining 19 patients constitute group II (18 RE group Vb and 1 group Va), none of whom had developed metastatic disease with a mean follow up of 54 months. None of the 24 patients had evidence of extraocular disease at enucleation. The surgical specimens from patients with unilateral retinoblastoma treated by enucleation at Hospital do Cancer AC Camargo between January 1992 and December 1995 were identified, reviewed and the clinical data recorded. Two subsequent histological sections were prepared. One stained with haematoxylin and eosin for assessment of choroidal and optic nerve invasion, and the other for immunoreaction with an endothelium specific marker (antibody anti-CD 34). The main outcome measures were choroidal and/or optic nerve invasion and quantification of the tumour’s relative vascular area (TRVA) obtained by Chalkley counting.
Results: Choroidal invasion was present in three eyes of group I (all massive) and six eyes of group II (two focal and four massive). Optic nerve invasion was found in two eyes of group I (all post-laminar) and four eyes of group II (three prelaminar and one post-laminar). There was no statistical difference regarding choroidal or optic nerve between the two groups. The TRVA was the only independent variable found to predict disease dissemination (p = 0.008 by Cox analysis). A TRVA equal to or greater than 3.9% had 100% sensitivity and 79% specificity in predicting disease dissemination.
Conclusions: Quantification of angiogenesis, through measurement of the TRVA, can help to identify patients with retinoblastoma at high risk for disease dissemination after enucleation.
- angiogenesis
- retinoblastoma
Statistics from Altmetric.com
There have been many attempts to identify risk factors in patients with retinoblastoma, both for the development of metastatic disease and for the extension of retinoblastoma locally into the orbit.1–15 The majority of these studies are based on the degree or extent to which neoplastic cells have invaded the optic nerve or choroid in enucleated eyes. Many published reports found a positive relation between tumour cell invasion of the optic nerve beyond the lamina cribrosa and an increased risk of disseminated disease.1,2,7,8,10,11,13,14 Other studies have identified massive choroidal invasion with or without scleral involvement alone as a risk factor for disease dissemination; still others suggest that only when both massive choroidal invasion and optic nerve extension beyond the lamina cribrosa are present, is there an increased risk of metastatic disease.1,2,5,7,9,11,12,14,15 Confounding the issue still further, some patients will develop orbital or metastatic disease in the absence of either risk factor, while others with positive risk factors will never develop disseminated disease.2,4,6,10,15,16
Faced with the lack of both sensitivity and specificity for the current risk factors in predicting disease dissemination, some authors question the use of an aggressive regimen of adjuvant therapy in patients whose enucleated eyes may show choroidal and/or optic nerve invasion past the lamina cribrosa but in which the cut end of the nerve is tumour free.4,5,15
It is well known that tumour cells possessing metastatic potential have accumulated mutations allowing them to induce angiogenesis.17–19 Tumour growth is dependent, at least for the most part, on the capacity of neoplastic cells to induce vascular ingrowth.17–22 There is evidence that the more aggressive a neoplastic clone, the greater is its angiogenic potential.17,18,23,24 This greater angiogenic potential or “capacity” can be quantified in different ways, and has been used as a prognostic marker for many human cancers.24–28
The potential to produce factors that will induce vascular growth has already been examined in both retinoblastomas and ocular melanomas.29–33 The detection of angiogenic potential in aqueous and vitreous humours has been proposed as a diagnostic test and antiangiogenic agents have been tested for efficacy in an experimental retinoblastoma tumour model.31,34 A tumour’s ability to induce vascular ingrowth, or tumour angiogenic capacity (TAC) has also been reported to be a strong prognostic marker for metastases in experimental and human choroidal melanoma.32,33
The purpose of this study is to determine whether or not TAC, calculated from one single section of the enucleated tumour specimen, is a reliable prognostic marker for the development of disease dissemination in retinoblastoma patients.
METHODS
This study was approved by the institutional ethics committee of the Hospital do Câncer AC Camargo, São Paulo, Brazil. In order to be certain that any disease dissemination (distant metastasis or orbital disease) in the study patients originated in the enucleated eye, we studied only patients with unilateral intraocular retinoblastoma, treated solely by enucleation. We carried out a retrospective analysis of the medical records of all patients with unilateral retinoblastoma seen at the Ocular Oncology Sector from the Hospital do Cancer AC Camargo, São Paulo, Brazil, from January 1992 to December 1995. Fifty eight patients were identified. Of these, 34 were excluded for the reasons listed in Table 1.
Excluded patients and exclusion criteria
Twenty four patients met the inclusion criteria and had sufficient data to be included in the study. These 24 patients were divided in two groups. Group I consisted of five patients who developed either local orbital disease or metastatic retinoblastoma at a mean of 10.4 months following enucleation (median 10; range 6–13). Group II consisted of the remaining 19 patients who did not develop disseminated disease in a mean follow up of 54 months. The patients are described in Tables 2 and 3.
Group I, patients who developed metastatic or orbital disease following enucleation
Group II, patients who did not developed metastatic or local orbital disease following enucleation
All patients in the study were classified as Reese-Ellsworth group Vb (with the exception of two patients classified as Va, one in each group) at diagnosis and treated by enucleation alone.35 No post-enucleation treatment was given in any case unless disease dissemination was documented.
One haematoxylin and eosin section of the enucleated eyes was examined for optic nerve and choroidal invasion risk factors using the classification proposed by Khelfaoui et al.14 When the maximal tumour height was not in the same plane as the pupil-optic nerve section, additional sections including the optic nerve were studied (Table 4).
Khelfaoui classification
In order to assess TAC, one additional tissue section, subsequent to the one for haematoxylin and eosin, was submitted for immunohistochemistry by the streptavidin-biotin-peroxidase complex method (Dako, Dane). The primary antibody used to highlight endothelial cells was the monoclonal antibody to CD 34 class II (Dako, Dane), at 1:50 dilution. Antigen retrieval was achieved by microwave treating the slides in a 0.01 mM citrate buffer (pH 6.0) at 1300 W for 9 minutes twice. Endogenous peroxidase activity was blocked by incubation of the slides in 0.3% hydrogen peroxide (H2O2) four times, 5 minutes each time. Normal goat serum was used to block non-specific antibody binding. Diaminobenzidine (DAB) 0.06% was used as the chromogen, staining microvessels dark brown. Finally, sections were counterstained with Harris’s haematoxylin. Tissue sections of a normal liver were used as the positive control. Negative control slides were generated by substituting phosphate buffered saline (PBS) solution for the primary antibody.
The CD 34 stained slides were scanned under ×100 magnification to identify the brownest vascular staining areas or “angiogenic hot spots.” The magnification was then increased to ×320. With the use of a 100 point graticule (KPL 16X Karl Zeiss, Germany), the intersections of the brown stained points with the graticule were counted in four fields from the same angiogenic hot spot resulting in a total of 400 points counted. A single investigator (VA), who was unaware of the clinical outcome, performed the histopathological review and measurement of the angiogenic capacity through the quantification of the tumour’s relative vascular area (TRVA).
The TRVA was calculated using the Fallowfield and Cook equation adopted from the previously described method of Chalkley26,36 and used as a measurement of TAC:
Number of intersections of brown pigment with the graticule/number of counted points × 100%
Statistical analysis
The statistical analysis was performed using the NCSS 2000 program (NCSS Statistical Software, UT, USA). Mann-Whitney-Wilcoxon U test and Kolmogorov-Smirnov test were used for two group comparative analysis. The Cox proportional hazard regression model was used to access which variables were independent predictors of metastatic and/or orbital disease using an assumed level of significance of 0.05. The receiver operating characteristic (ROC) curve analysis was used to evaluate sensitivity and specificity of the TRVA as a predictor test for disease dissemination.
RESULTS
In the two groups of patients, the only variable that achieved statistical significance as a predictor of subsequent disease dissemination was the TRVA (Table 5). The mean TRVA was 4.5% in group I (median 4; range 4–6%) and 2.75% in group II (median 2.5; range 1.25–4.75%).
Level of significance of each variable by the Mann-Whitney-Wilcoxon U test and Kolmogorov-Smirnov test
There was no difference between the two groups with regard to age at diagnosis, the greatest tumour diameter, choroidal invasion, or optic nerve invasion (Table 5).
By Cox proportional hazard regression, the only variable that independently predicted the development of orbital and/or metastatic disease was the TRVA (p = 0.008). Neither tumour diameter (p = 0.84), choroidal invasion (p = 0.77), nor optic nerve invasion (p = 0.62) achieved statistical significance.
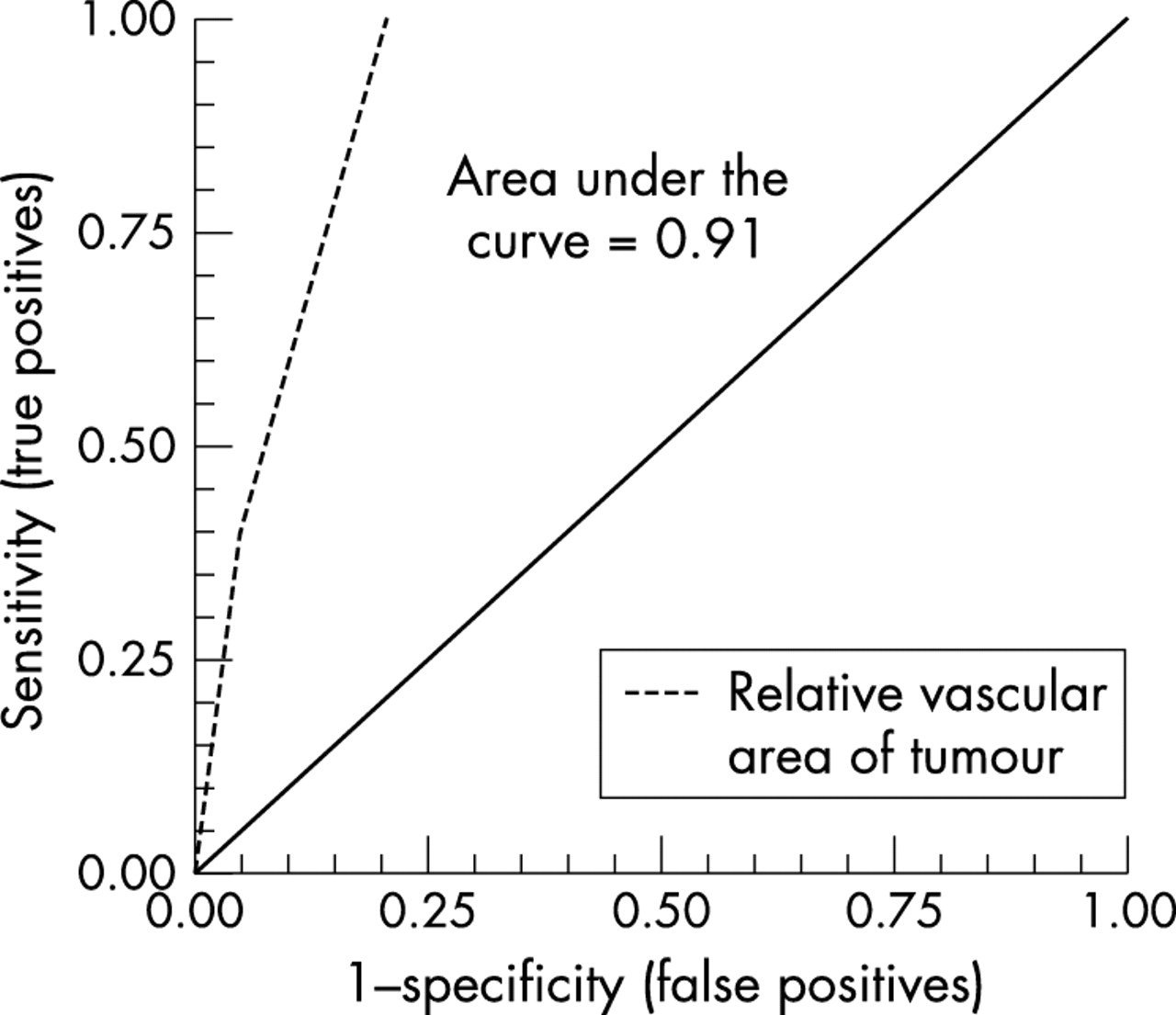
ROC curve analysis was done to access the sensitivity and specificity of this finding. A TRVA of 3.9% was found to be the point of best balance between sensitivity (100%) and specificity (79%) for the risk of developing metastatic and/or orbital disease following enucleation (Fig 1). The area under the curve for the TRVA was 0.91.
{kind=link}
ROC curve for the tumour’s relative vascular area as a predictor of disease dissemination.
Metastatic disease was diagnosed in all five group I patients at mean of 10.4 months, with the maximum time of 13 months following enucleation (Table 2). The shortest follow up for any of the 19 group II patients, who did not develop metastatic and/or orbital disease was 16 months (Table 3). Thus we considered that an adequate follow up was obtained and that none of the tumour free patients in group II was tumour free because they had not been followed for a sufficient period of time. The location of relapsed extraocular disease and final outcome of each group I patients are listed in Table 2. Since only patient 3 in group I and patient 18 in group II were classified as Reese-Ellsworth Va, with the remaining classified as Vb, no conclusions could be drawn with regard to this variable.
DISCUSSION
After enucleation has been performed in patients with retinoblastoma, the ocular pathologist is called on to estimate the risk for metastatic disease to the clinician. Currently, the decision about the use of prophylactic therapy is based on the histopathological presence and extent of tumour cell invasion into the optic nerve and/or choroids.1–15,37–39 Most commonly only patients with optic nerve post-laminar invasion are recommended for prophylactic or adjuvant treatment.37
Retrospectively, we can hypothetically evaluate the precision of optic nerve invasion, choroidal invasion, and the TRVA as criteria to define which patients would need prophylactic treatment in our series. If post-laminar invasion of the optic nerve had been the criterion used in deciding when adjuvant therapy was indicated in this series, three of the five patients who developed disease dissemination (numbers 2, 3, 4 of group I, Table 2) would not have been treated. Patient 19 (group II, Table 3), who did not develop disease dissemination, would have been unnecessarily treated. If massive choroidal invasion alone had been the treatment criterion, two patients in group I (2, 4, Table 2) would not have been treated and unnecessary treatment would have been given to four patients (5, 9, 13, 19 in group II, Table 3). If a TRVA equal to or greater than 3.9% had been used, all patients who did develop disease dissemination would have received adjuvant therapy shortly after enucleation and disease dissemination probably would have been avoided. Using the same criterion, four patients who did not develop disease spread without treatment would have received adjuvant therapy unnecessarily (patients 16–19 in group II, Table 3).
One possible limitation of our study is that only eight of our patients had post-laminar invasion of the optic nerve and/or massive choroidal invasion. This is probably the experience of most centres that treat this rare disease. The low incidence of disease dissemination after enucleation for intraocular retinoblastoma, and the great heterogeneity in its management, can further obscure the importance of optic nerve and choroidal invasion, since some forms of pre-enucleation and post-enucleation treatment can act as protective factors against disease dissemination.12,37 In this series we did not include patients with optic nerve invasion up to the surgical margin nor did we include those with known extrascleral invasion.
Reports of metastatic and/or orbital disease after enucleation in the absence of any current histopathological risk factors do exist, exemplifying their lack of sensitivity. In Kelfaoui’s series, orbital or metastatic disease was detected in 23 of 172 patients, three of them had only minimal choroidal invasion and prelaminar optic nerve invasion.14 Shields et al reported two cases of metastatic disease in the absence of optic nerve or choroidal involvement of any kind.12 MacKay et al also reported two patients with metastatic disease but no evidence of optic nerve and choroidal invasion. These authors assume that an inadequate histological sample was probably the cause.6 In our series, two of the five patients in group I had no optic nerve or choroid invasion and developed orbital disease (Table 2).
Inadequate histological sampling seems to be a major error factor when evaluating prognostic factors. Sampling all the specimens would solve this problem, but it is not practical nor is it adequate for routine use. This is why we chose a test that even when performed in a single tumour slide section can give reliable prognostic information, making it suitable for routine use.
Angiogenesis is a term that defines any new vessel formation from the pre-existing vascular bed.40 Under physiological conditions it is usually limited to development, reproductive and cicatrisation periods.17 Tight control of angiogenesis is lost in some disease processes like rheumatoid arthritis, many retinopathies and cancer.22
Two phases, avascular and vascular, divide the natural history of cancer.19,21 In the avascular phase, tumour growth is greatly limited owing to lack of nutrients and the cells clones are incapable of metastasising. In the vascular phase, there is a shift to an angiogenic phenotype that results in exponential tumour growth.17–20,22,41
There is published evidence of angiogenic capacity as a diagnostic marker in retinoblastoma.29–31 The only study that investigated any correlation between the vascular component and prognosis in retinoblastoma failed to prove it, perhaps because of the choice of an antibody that was not specific for endothelial cells and the use of non-quantitative methodology.9
It is accepted that cancer cells exist in a hypermutable state. This can lead to the accumulation of genetic alterations. If any of these random mutations result in the creation of tumour clones with an increased growth rate and the ability to metastasise, these clones will rapidly become the dominant cell in the tumour.39
The TAC has been shown to be, at least in part, dependent on some of those genetic alterations, such as inhibition of the p53 tumour suppressor gene.42–44 Thus, the complex metastatic process which involve shedding of cells, escaping the host immune system, invasion through vessels walls by the neoplastic cells, extracellular matrix degradation, and recruitment of a vascular supply seems much easier for a highly angiogenic cell lineage.18,19,40
The use of the TRVA (assessed by Chalkley count) as a measurement of the TAC has been shown to be sensitive, reproducible, and objective.25,26,45 This morphometric method to estimate the volume of a three dimensional structure from a thin two dimensional slice was adapted from the work of geologists and metallurgists.36,46 It is based on the Delesse principle: “the planimetric fraction of a section occupied by sections of a given component corresponds to the fraction of the tissue volume occupied by this component.”46
According to the Cox proportional hazards regression analysis, only the TRVA proved to be an independent prognostic predictor for disease dissemination (p = 0.008). Although all patients who developed disseminated disease had a TRVA equal or greater than 4%, four patients in group II who did not subsequently develop disease spread had measurements equal to or above this value (Table 3). Of particular note is patient 19 who had a TRVA of 4.75%, post-laminar optic nerve invasion, massive choroidal invasion, and did not develop metastatic disease. Another interesting issue is that patients 2, 3, and 4 in group I developed their first manifestation of extraocular disease in the orbit. Although this could represent a non-detected microscopic direct extraocular extension present at the time of surgery rather than metastatic dissemination, the TRVA would still be capable of predicting a poor prognosis in these patients. Thus, it is clear that whatever the dissemination mechanism an increased ability to recruit vessels is crucial for tumour growth.
As is the case in many human cancers, probably the most important prognostic predictor in retinoblastoma is still an early diagnosis.10,47–49 Our series contains a higher proportion of patients who developed disseminated disease after enucleation than some similar series.11,12,14 This fact may reflect more advanced intraocular disease in our patients since the average age at diagnosis is greater than the mean for unilateral tumours in other series.37,48 It is logical to assume that since a large tumour has undergone more cellular divisions, its probability of accumulating the genetic alterations required for metastatic spread is increased.
The TRVA seems to be a promising prognostic marker that should be evaluated in a larger sample of retinoblastoma eyes. It holds the promise of improving the accuracy of our prediction in detecting those patients who truly need adjuvant chemotherapy to protect against micrometastatic disease.
Acknowledgments
The authors wish to thank “Instituto Ludwig” and the Department of Pathology from Hospital do Cancer AC Camargo, São Paulo, Brazil, for kindly providing the necessary facilities during part of this research. Also we wish to thank Suely Nanogaki, for the tissue processing. Eduardo Marback was supported by “Conselho Nacional para Pesquisa, CNPq,” Brazil.
REFERENCES
Linked Articles
- BJO at a glance