Article Text

Abstract
Objective To assess whether the brain MRI results obtained during hypothermia identify the later brain injury observed in asphyxiated newborns after therapy is completed.
Patients and methods Asphyxiated newborns treated with hypothermia were prospectively enrolled in this study if they had at least one MRI performed during hypothermia treatment and then another MRI performed around day 10 of life.
Results A total of 129 MRI scans were obtained from 43 asphyxiated newborns treated with hypothermia. Sixty per cent developed brain injury; all the brain injuries observed on the late scans were already present on day 2–3 of life during hypothermia, and the extent of injury was similar between the early and late scans. The brain MRI on day 2–3 of life had a sensitivity of 100% (95% CI 84% to 100%) and a specificity of 100% (95% CI 77% to 100%) to identify the presence and extent of later brain injury.
Conclusions The brain MRIs performed during hypothermia already permit an accurate definition of the presence and extent of brain injury that later develop in asphyxiated newborns despite treatment. These results may have research and clinical implications for the care of these newborns.
- Neonatology
- Imaging
- Neurology
Statistics from Altmetric.com
What is already known on this topic
-
For asphyxiated newborns treated with hypothermia, brain MRIs are typically obtained after treatment is completed to identify the extent of brain injury and to try to predict later outcomes.
-
Questions remain as to whether the brain injuries observed by MRI during hypothermia are definitive or reversible.
What this study adds
-
The brain MRIs performed during hypothermia already permit an accurate identification of the extent of injury that later develop in asphyxiated newborns despite treatment.
-
The early diagnosis of brain injury has important clinical and research implications for the care of these newborns.
Introduction
Therapeutic hypothermia is the most widely accepted neuroprotective strategy to minimise brain injury in term asphyxiated newborns.1–5 The existing literature on the brain imaging of asphyxiated newborns treated with hypothermia6–13 usually uses the brain imaging performed after the completion of the hypothermia. The available studies mainly address the incidence and type of brain injury observed following treatment, and their predictive value for subsequent neurological impairment.9 ,11 ,13 Other studies have investigated the value of some common MRI parameters at one time-point for these newborns.6–8 ,12 However, these studies do not provide the optimal earliest timing for performing brain imaging in these newborns so as to accurately define their developing brain injuries despite treatment.14–16 The optimal earliest timing of imaging has been studied extensively in asphyxiated newborns before the cooling era,17–19 but not in the cooling era. Only one previous study evaluated the usefulness of brain MRI findings performed during cooling for these newborns,20 although it only included 12 asphyxiated newborns treated with hypothermia.
The present study was designed to assess the brain imaging findings during hypothermia in a larger group of asphyxiated newborns treated with hypothermia and to compare these results with the brain imaging findings obtained around day 10 of life to determine if the MRIs performed during hypothermia may already identify the presence and extent of brain injury that develops despite hypothermia.
Patients and methods
We conducted a prospective cohort study of term asphyxiated newborns admitted to our neonatal intensive care unit (NICU) from 2008 to 2014, who met the criteria for induced hypothermia.1 ,2 ,4 The eligible patients received whole-body cooling to an oesophageal temperature of 33.5°C, initiated by 6 h of life and continued for 72 h. Nine of these patients were already included in a previous report;20 additionally, 34 new patients were included in this study. The research protocol was approved by the institutional review board and informed parental consent was obtained in all cases.
Clinical data were collected prospectively for each patient, which included gestational age, birth weight, sex, Apgar score at 10 min, rate of intubation and chest compression at birth, arterial cord pH, initial infant blood gas pH and later outcome. The initial background pattern of amplitude-integrated electroencephalogram was assessed on admission.2 ,21 The initiation of hypothermia in hours of life was calculated and recorded.
Asphyxiated newborns were imaged by MRI once or twice during hypothermia treatment, and then again later around day 10 of life and sometimes around 1 month of age. Patients were included in this study only if they were enrolled within the first 6 h of the hypothermia treatment. MRI scans were performed at the different time-points if the newborns were haemodynamically stable at the time of the MRI and if the team to transport them safely to and back from the MRI at the different time-points was available.
The patients receiving hypothermia had their therapy maintained during the MRI scan without any adverse events.22 Any ventilation, pressor support or sedation was maintained during the MRI scanning process, and additional sedation was avoided. The MRI scans were performed using a 3T Siemens Symphony (Siemens, Erlangen, Germany) or a 3T Philips MR Systems Achieva (Philips Medical Systems, Best, The Netherlands) scanner. Each MRI study included a T1-weighted magnetisation-prepared rapid acquisition of gradient echo (TR/TE, 1600/2.2 ms; matrix size, 192×192; FOV, 180 mm; 160 sagittal sections with a section thickness of 1.0 mm), a T2-weighted fast spin-echo (TE, 123 ms; matrix size, 256×256; FOV, 220 mm; 110 axial sections with a section thickness of 1.0 mm), and a single-shot spin-echo echo-planar diffusion-weighted (b=750 s/mm2) isotropic image (TR/TE, 8400/84 ms; matrix size, 128×128; FOV, 220 mm; 50 axial sections with a section thickness of 2.2 mm). Paediatric neuroradiologists, who were blind to the clinical conditions of the infants, interpreted the MRI images on the day of the imaging. Each MRI was scored using an MRI scoring system.23 This MRI score provided a quantitative evaluation of the presence and extent of the brain injury.
Statistical analysis was performed to assess the clinical differences between the newborns developing or not developing brain injury. A χ2 test was used for the categorical data and a Mann–Whitney U test for the continuous data. A p value <0.05 was considered significant.
The MRI scores obtained around day 10 of life were used as the reference to determine the extent of the brain injury for each patient.24 ,25 An analysis was performed by comparing the MRI scores obtained at each timing to the MRI scores obtained around day 10 of life. Only exact equal MRI scores between the two time-points was defined as being correct. Sensitivity and specificity were calculated for each MRI timing to determine how accurately each MRI timing identified/confirmed the extent of the brain injury. We also calculated κ to quantify the degree of agreement between the MRI scores obtained at each timing and the MRI scores obtained around day 10 of life.
Results
A total of 129 MRI scans were obtained from 43 asphyxiated newborns treated with hypothermia. Sixty per cent developed brain injury and 40% did not. Among the newborns developing injury, 19% had an injury predominantly in the basal ganglia, 42% had an injury predominantly in the white matter and 39% had an injury extending to the basal ganglia, white matter and cortex. Several newborns displayed unexpected findings, including subdural haematoma (14%), intraventricular haemorrhage (5%) and venous sinus thrombosis (2%).
Most clinical data were not different for the asphyxiated newborns who developed or did not develop brain injury (table 1). The newborns developing injury presented more often with a severe encephalopathy on admission (p=0.01).
Clinical characteristics of the asphyxiated newborns treated with hypothermia
Forty-two per cent of the newborns had a brain MRI performed on day 1 of life, 100% on day 2–3 of life, 100% around day 10 of life (range: day 7–13 of life) and 58% around 1 month of age (range: day 28–38 of life) (see online supplementary appendix). Forty-three per cent of these newborns did not demonstrate any injury, neither on the early nor later scans. Sixty per cent developed injury; all the brain injuries observed on the scans around day 10 of life (on the conventional T1-/T2-weighted imaging) were already present on day 2–3 of life (especially visible on the diffusion-weighted imaging), and the extent of injury was similar between the early and late scans (figure 1). The brain imaging performed around day 10 of life did not reveal any new injury that had not been seen on the MRI scans performed on day 2–3 of life. The brain MRIs performed on day 1 of life tended to underestimate the complete extent of the later injury. The brain MRIs performed around 1 month of age confirmed the extent of injury seen on day 2–3 and around day 10 of life, and did not show any evidence of new injury that had not been seen on the previous scans.
{kind=link}
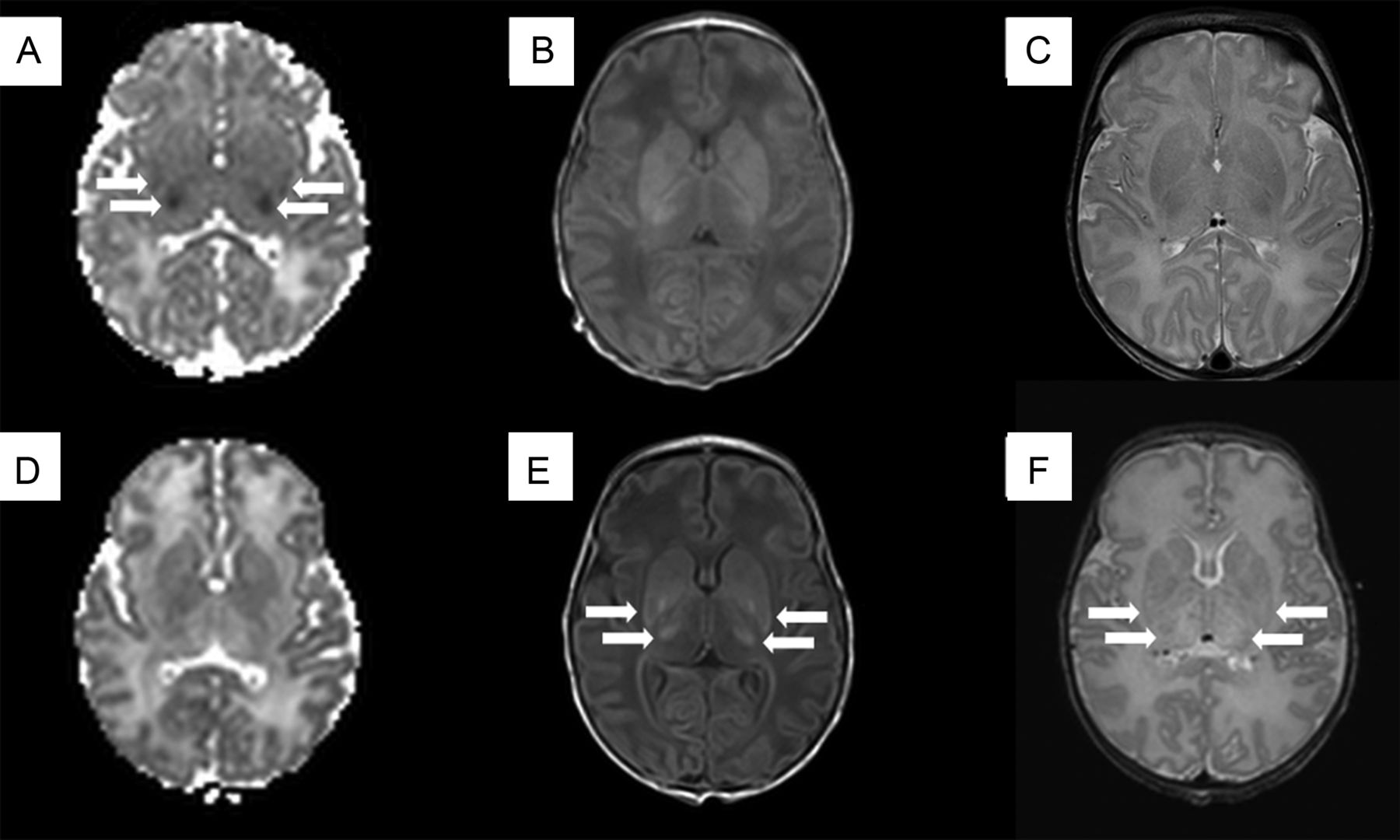
Brain MRIs of a term asphyxiated newborn treated with hypothermia, performed on day 2 of life (A–C) and on day 9 of life (D–F). For each MRI exam, the first column shows the apparent diffusion coefficient (ADC) maps, the second the axial T1-weighted imaging and the last column the axial T2-weighted imaging. The MRI on day 2 of life for this patient shows a restricted diffusion involving the thalami and lentiform nuclei (arrows). On day 9 of life, the ADC map ‘normalises’, while findings become more and more evident on the subsequent T1-weighted and T2-weighted imaging (arrows).
We then compared the MRI scores obtained at each timing to the MRI scores obtained around day 10 of life (table 2). The brain MRIs obtained on day 1 of life had a sensitivity of 45% (95% CI 18% to 75%) and a specificity of 100% (95% CI 60% to 100%) for identifying the presence and extent of later brain injury. The brain MRIs obtained on day 2–3 of life had a sensitivity of 100% (95% CI 84% to 100%) and a specificity of 100% (95% CI 77% to 100%). The brain MRIs obtained around 1 month of age had a sensitivity of 100% (95% CI 75% to 100%) and a specificity of 100% (95% CI 66% to 100%) to confirm the extent of injury measured around day 10 of life. The agreement between brain MRIs obtained on day 1 of life and brain MRIs around day 10 of life was quite low with κ at 0.41 (95% CI 0.02 to 0.80). However, we observed perfect (κ=1) agreements between brain MRIs obtained on day 2–3 of life and brain MRIs on day 10 of life, as well as between MRIs obtained on day 10 of life and those around 1 month of age.
Sensitivity and specificity of each timing to detect the extent of brain injury in asphyxiated newborns treated with hypothermia, compared with day 10 of life
Discussion
In most of the imaging studies of asphyxiated newborns treated with hypothermia,6–9 ,11–13 brain MRI is typically obtained just after cooling, between day 4–7 of life. In most cases, this timing is due to practical reasons, since it falls within the window of time after the induced hypothermia is complete and before the transfer to another care centre. It has also been reported to be convenient, as therapeutic hypothermia has been reported to slow the diffusion abnormalities on MRI in asphyxiated newborns.6 ,10 ,26 However, in the era before hypothermia, this timing was not considered to be the ideal time to obtain the brain imaging of asphyxiated newborns; abnormalities of diffusion may be less evident than in the first few days of life, and abnormalities on anatomical imaging may still be difficult to visualise, especially in mild forms of neonatal encephalopathy.17–20 In this present study, brain MRIs performed on day 2–3 of life during hypothermia for 43 newborns demonstrated the whole extent of injury as observed on the late scans around day 10 of life. These results confirmed that the brain MRI scans obtained during hypothermia already accurately identify brain injuries that develop in asphyxiated newborns despite hypothermia.20 Diffusion-weighted changes were subtle within the first 24 h of life, but became apparent and better defined on day 2–3 of life. Abnormalities on day 2–3 of life were mainly seen on the diffusion-weighted imaging, and abnormalities on day 10 of life were mainly based on T1-/T2-weighted imaging. Interestingly, the brain MRIs performed around 1 month of age confirmed the extent of injury seen around day 10 of life and did not show any new injury that had not been observed around day 10 of life, justifying the hypothesis that day 10 of life could be used as the reference.
Being able to diagnose brain injury already during cooling has clinical implications. Obtaining MRI scans during hypothermia, especially if the result corresponds to a later injury usually diagnosed after cooling, could bring more information to the discussion between caregivers and parents, especially in severe cases when some parents choose palliative care rather than pursuing an intensive care treatment. As an anecdote, one of the newborns included in this study was born with severe meconial aspiration and asphyxia; he developed severe respiratory distress and pulmonary hypertension and required high ventilatory settings and heavy sedation to allow adequate ventilation. Due to the sedation, his amplitude-integrated electroencephalogram, which initially showed a moderate encephalopathy on admission, became a severe grade. The question of whether extra-corporeal membrane oxygenation should be used was raised, considering the difficulties in oxygenating this newborn. The caregivers had an ethical discussion, since they shared different opinions about what was the reasonable option to propose to the parents (ie, extra-corporeal membrane oxygenation or withdrawal of care), especially considering the severe encephalopathy and the high risk of brain injury. In this case, a brain MRI was performed on day 2 of life, which showed minimal brain injury in the white matter; so, extra-corporeal membrane oxygenation was offered as an option to the parents, and the newborn survived and presented afterwards with only the minimal injury seen on the day 2 of life MRI. Our study with a large group of asphyxiated newborns treated with hypothermia suggests that brain MRIs should be considered as an important element in the discussion, along with the newborn's history, the clinical exam and the amplitude-integrated encephalogram evolution. The long-term prognostic value of MRIs remains to be determined by correlating these findings with long-term development. However, first observations have shown that the predictive value of these MRI scans for identifying subsequent neurological impairment does not seem to be affected by therapeutic hypothermia.11 Obtaining MRI scans during hypothermia and again around day 10 of life may also provide some indications about the timing of the hypoxic events.24 ,25 Early scans may exclude antenatal brain injury.20 For our 43 newborns scanned during hypothermia on day 2–3 of life, the diffusion-weighted imaging were abnormal and not yet pseudonormalised, and injuries were not yet obvious on T1-/T2-weighted imaging, suggesting that none of these patients presented with antenatal brain injury.
The ability to diagnose brain injury during cooling also has potential research implications. Studies that examine the adjustments of existing cooling guidelines or the use of adjunctive treatments for neonatal encephalopathy (eg, xenon, erythropoietin) are becoming available, with a goal to further increase the proven benefits of hypothermia and, thus, improve future neurodevelopmental outcome.27 The current tools used to identify the newborns at risk include clinical signs, the neurological exam and the assessment of brain activity by an amplitude-integrated electroencephalogram,2 ,28 although none of these tools has a high sensitivity for identifying newborns at risk. Our study suggests that the brain MRIs performed during hypothermia on day 2–3 of life have a high sensitivity and agreement for identifying the presence and extent of brain injury. These results may prove to be of importance for selecting the most appropriate candidates for trials of adjunctive or alternative therapies and show more quickly the benefits of these treatments.27
Obtaining an MRI during hypothermia may appear technically challenging. However, after the appropriate training of NICU staff, maintaining hypothermia during a brain MRI as well as the other treatments (ie, ventilation, inotrops and others) has been demonstrated to be safely and reliably feasible for most asphyxiated newborns.22 Nevertheless, we have noted some practical challenges to obtaining such MRIs compared with MRIs after cooling. These challenges include obtaining consent from parents within a short time-frame, the rapid coordination necessary between the NICU and the radiology department, the stabilisation of the newborns who might be highly unstable within the first 72 h of life and the safe transport to and back from the MRI unit. Today, in a busy NICU environment—in which the caregiving team is getting smaller compared with the increasing numbers of hospitalised newborns—sending a complete team to the MRI with one newborn may be challenging to organise in a few hours on day 1 of life. However, by day 2–3 of life, the potential impact of such an imaging study probably outweighs the challenges. For the 43 newborns scanned during hypothermia on day 2–3 of life, treatments as well as hypothermia were maintained during the MRI scan without any adverse events.
Our sample of 43 patients was collected prospectively, but did not include all the consecutive newborns admitted to the NICU who were treated with hypothermia. Thus, it did not permit us to compare our results with those of previous studies that reported on the incidence of the different types of brain injury in this population.9 ,11 ,13
For the present study, we wanted to focus on the reading of the conventional sequences by the neuroradiologists so as to determine how accurate they were in determining later injury. The neuroradiologists were scoring the imaging on the day it was performed; they were allowed to compare with the previous imaging when available and they always indicated in their reports whether the injury increased, decreased or remained stable on later scans. So for example, if the MRI was performed on day 2 of life, the neuroradiologist would read the MRI on day 2 of life, but would also have access to the MRI on day 1 of life if one was done at this timing. Around day 10 of life, the neuroradiologist would read the MRI on day 10 of life, but would also have access to the MRI on day 2 of life for comparisons. A total of four different neuroradiologists scored the different imaging. Inter-rater reliability was not assessed, which is one of the main limitations of the present study.
In conclusion, brain MRIs performed during hypothermia already permit an accurate definition of the presence and extent of brain injury that has developed in asphyxiated newborns despite treatment. These results should stimulate the caregivers of these newborns to discuss and rethink the current practice concerning the timing of MRIs obtained for diagnostic purposes. For these newborns, brain MRIs could probably be obtained during hypothermia and/or around day 10 of life, depending on the clinical settings and the feasibility of obtaining brain MRIs during hypothermia. After appropriate training, scanning asphyxiated newborns during hypothermia on day 2–3 of life is feasible in most of these newborns without any adverse events. Scanning during hypothermia may have important clinical and research implications for the future care of these at-risk newborns.
Acknowledgments
The authors thank the families and their newborns for participating in this study. Special thanks to the NICU nurses, NICU respiratory therapists and MRI technicians who have made this study possible.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors This manuscript has been contributed to, seen and approved by all the authors. EB coordinated and supervised data collection, carried out the analyses, drafted the initial manuscript and approved the final manuscript as submitted. XT brought his expertise to the statistical analysis of this article, critically reviewed the manuscript and approved the final manuscript as submitted. CS-M and her colleagues reviewed all the brain MRIs of the newborns included in this study, critically reviewed the manuscript and approved the final manuscript as submitted. MS brought his neurology expertise to the analyses, critically reviewed the manuscript and approved the final manuscript as submitted. PW conceptualised and designed the study, reviewed and revised the manuscript, and approved the final manuscript as submitted.
-
Funding PW receives research grant funding from the FRSQ Clinical Research Scholar Career Award Junior 1, New Investigator Research Grant from the SickKids Foundation and the CIHR Institute of Human Development, Child and Youth Health (IHDCYH), and The Research Institute of the McGill University Health Center/Montreal Children's Hospital.
-
Competing interests None.
-
Ethics approval The research protocol was approved by the Local Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.