Article Text

Abstract
Background: Measurements of the subarachnoid space during routine cranial sonography may provide an indirect method of monitoring brain growth in preterm infants.
Methods: The width of the subarachnoid space was measured on coronal views during head sonography. Initial scans (within five days of birth) were compared with follow up scans.
Results: A total of 361 scans were performed on 201 preterm infants. The mean width of the subarachnoid space was < 3.5 mm for 95% of initial scans. It was slightly larger in neonates born closer to term, the equivalent of an increase of 0.02 mm/gestational week (95% confidence interval 0 to 0.10 mm) for initial scans. When the scans of all infants, born at 24–36 gestational weeks who were 36 weeks corrected gestational age were compared, the mean (SD) subarachnoid space was 60% larger for follow up scans than for intial scans: 3.2 (1.38) v 1.95 (1.35) mm (p = 0.002) or the equivalent of a mean increase of 0.20 mm/week (95% confidence interval 0.15 to 0.30 mm) for follow up scans. At 36 weeks corrected gestational age, mean head circumference was not different between those having initial or follow up scans (33.0 (2.0) v 32.2 (1.9) cm; p = 0.31).
Conclusions: The mean subarachnoid space is normally < 3.5 mm in preterm infants. The difference between initial and follow up scans suggests reduced brain growth in extrauterine preterm babies.
- preterm
- brain
- subarachnoid space
- ultrasonography
Statistics from Altmetric.com
Premature infants often undergo cranial sonography during their stay in the neonatal nursery, and the width of the subarachnoid space can be easily measured during this examination. In the preterm population, measurement of the subarachnoid space may represent an indirect method of assessing and monitoring brain growth during a period of rapid brain development. Although normal data are available for older children,1, 2 to date there are no normal values for the width of the subarachnoid space in the preterm population.
The aims of this study are twofold. Firstly, we describe the technique used to measure the subarachnoid space, and secondly we present results from a population of preterm infants during their stay in hospital.
METHODS
Infants born at less than 37 weeks gestation between 1 October 1998 and 31 October 2000 who were admitted to our nursery and had undergone cranial ultrasonography were included in this prospective study. In our unit, all infants less than 30 weeks of gestation have routine cranial ultrasound examination on days 5 and 28 of life, and on other occasions as clinically indicated. In addition to sector scanning, linear array scans with a high frequency (high resolution) transducer are routinely used to assess the meningeal space, superior sagittal sinus, cortex surface, and cerebral parenchyma.
All scans were performed using the ATL 3000 (Advanced Technological Laboratories, Bothell, Washington, USA) ultrasound machine. The width of the subarachnoid space was measured on coronal views through the anterior fontanelle using a 10 MHz linear array transducer. A generous amount of coupling gel was applied to the transducer surface, and all ultrasonograms over the anterior fontanelle were performed without pressure.
Electronic calipers were positioned in a perpendicular fashion from the lateral edge of the superior sagittal sinus to the surface of the brain, and the width measured to within 0.1 mm (fig 1). This was repeated on both right and left sides.

Coronal scan of an infant at 33 weeks of gestational age. The subarachnoid space is measured in perpendicular fashion, with electronic calipers, from the edge of the triangular sagittal sinus to the surface of the cortex. The right subarachnoid space is 0.17 cm, and the left is 0.21 cm, resulting in a mean measurement of 1.9 mm. Note that the skin line of the scalp is evident (arrow), indicating that there is no effective pressure from the transducer.
Only normal scans showing no demonstrable intracranial pathology were included in this study. Because of concerns about the effects of corticosteroids on brain growth,3 scans from babies treated with corticosteroids after birth were excluded. “Initial scans” were those performed within 5 days of life. All subsequent scans were termed “follow up scans”. Thus, some infants had more than one repeat scan included in the study.
Head circumference was measured on the day of the ultrasound scan using a paper tape to obtain the greatest occipitofrontal diameter. In instances when this was not done (96 occasions), the head circumference documented in the clinical notes closest to the date of the ultrasound examination was used (mean (SD) difference of 4.0 (5.5) days).
Intraobserver variation was calculated from measurements acquired by one observer (radiology registrar) from two sets of scans from each of 10 infants. Interobserver variation was caculated from measurements by 12 observers (registrars, consultant radiologist, and sonographers) on a set of scans from each of three infants.
Data were analysed using Statview version 5.0.1 (SAS Institute, North Carolina, USA). All values are given as mean (SD) or mean and 95% confidence intervals. Measurements from the right and left side or from babies of different sexes were compared using Student's t tests. The relation between gestational age and width of the subarachnoid space or head circumference was determined using linear regression analysis. A higher order regression analysis did not improve the fit of the data.
RESULTS
After eliminating from the analysis infants who had received postnatal steroids or who had intracranial pathology, 361 scans were performed on 201 infants (104 boys, 97 girls). Mean (SD) birth weight was 1431 (510) g and mean (SD) gestation was 30 (2.5) weeks. Initial scans were performed at a mean age of 4.7 (2.8) days.
There was no difference in the width of the subarachnoid space between sexes. Because there was no significant difference in the width of the subarachnoid space over the right and left cerebral hemispheres (mean difference, 0.6 mm; p = 0.16), a mean width of the subarachnoid space was calculated for each study. Interobserver coefficient of variation was 0.08 (0.04), and intraobserver coefficient of variation was 0.09 (0.06).
On initial cranial sonograms, premature infants had a mean subarachnoid space width of 1.56 (0.95) mm. The width was less than 3.5 mm in over 95% of cases (fig 2). The subarachnoid space measured on initial scans increased by 0.02 mm with each week of increased gestational age (95% confidence interval 0.00 to 0.10 mm). The mean width of the subarachnoid space on follow up scans was 1.94 (1.23) mm. When considering follow up scans only, the subarachnoid space width increased by 0.20 mm with each week of increased gestational age (95% confidence interval 0.15 to 0.30 mm) (fig 2). Thus, in babies who had reached 35–37 weeks of gestation, mean subarachnoid space measurements were 60% larger in those having follow up scans than in those having initial scans (3.21 (1.38) v 1.95 (1.35) mm; p = 0.002).
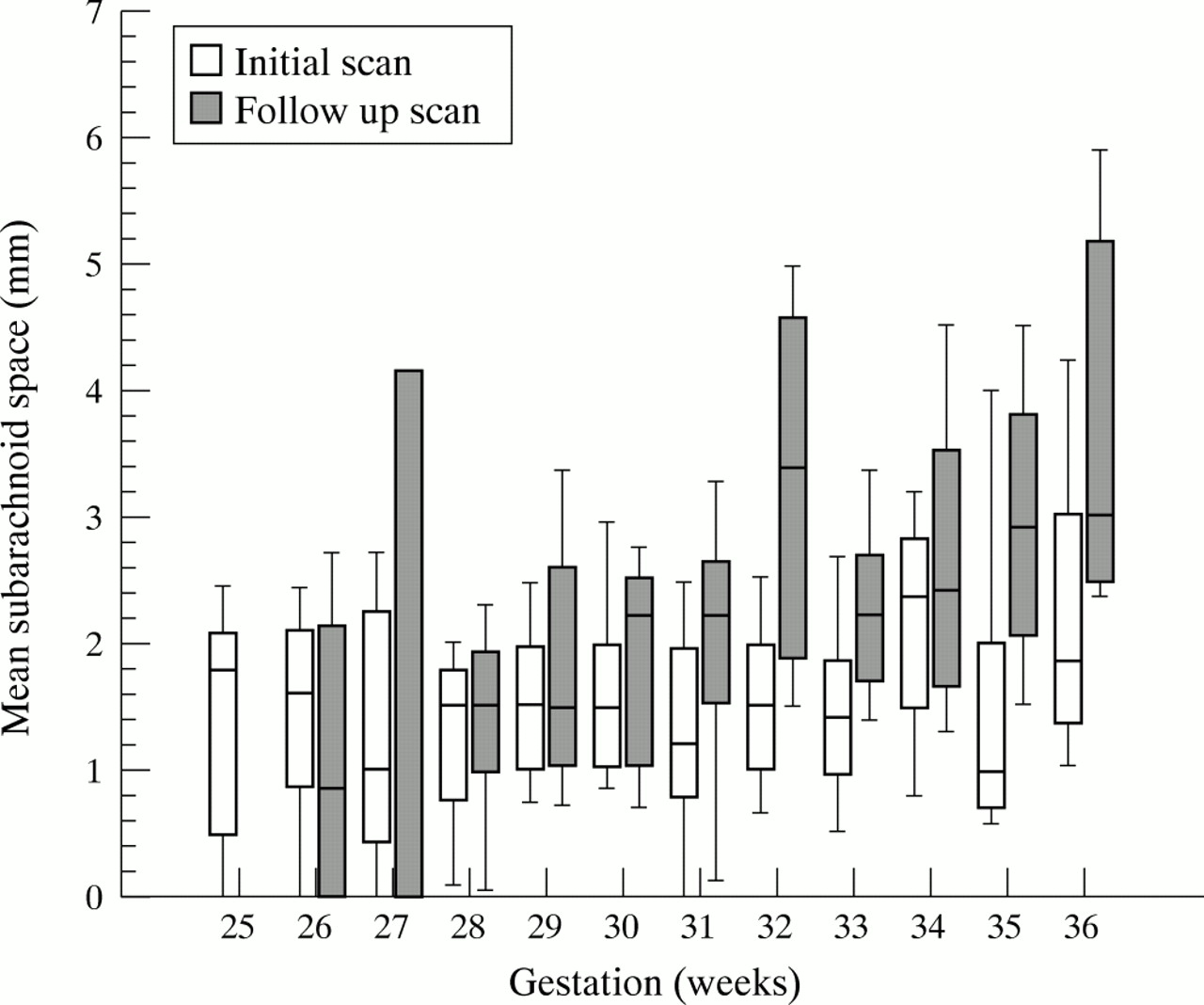
Box plot of subarachnoid space measurements at each gestational week of age. Bars show interquartile range, the middle line indicates the median, and whiskers indicate the 10th and 90th centiles. For initial scans, n = 201 (range 6–29 for each week), for follow up scans, n = 160 (range 3–22 for each week).
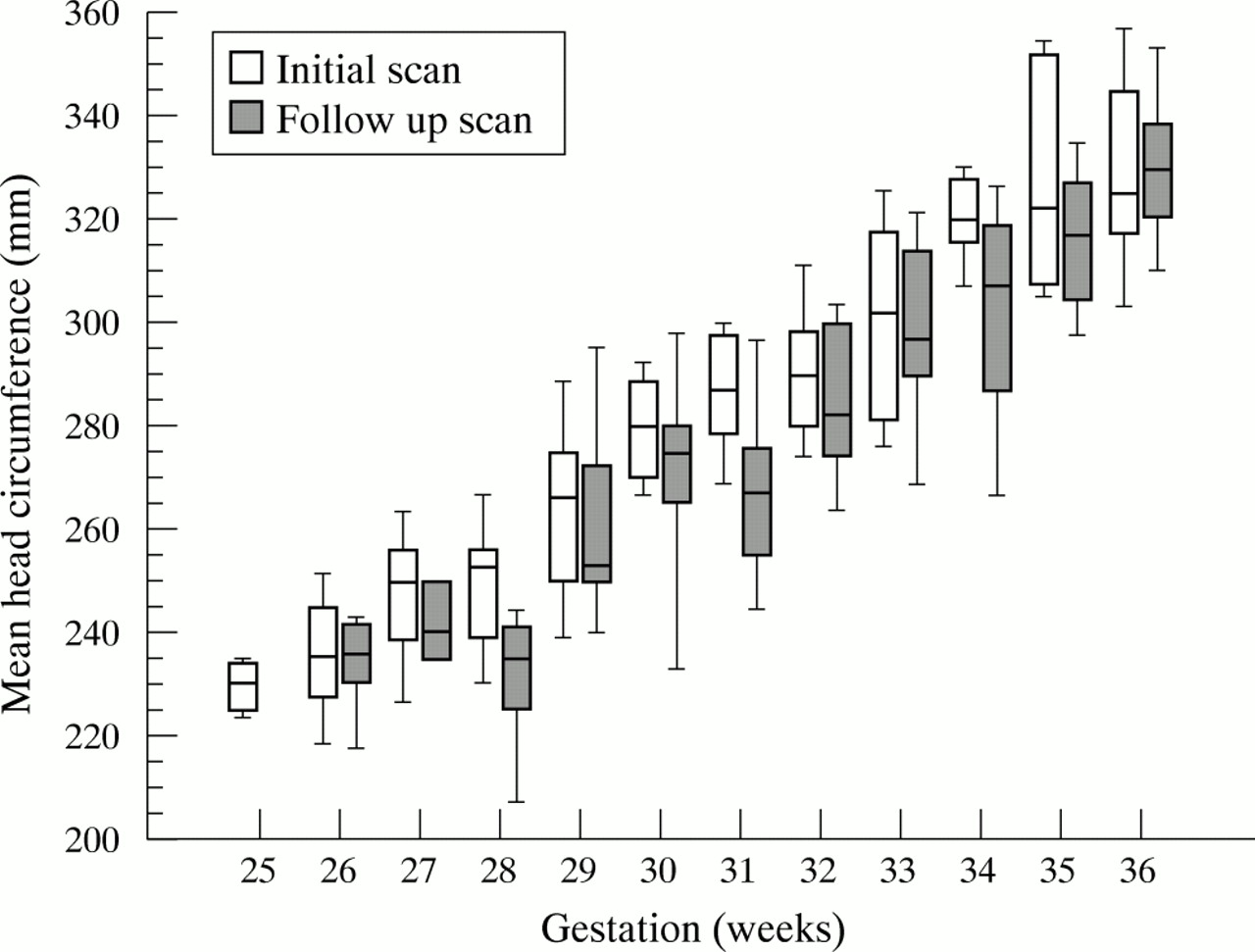
The increment in head circumference per week of gestation was not different between infants having initial scans and follow up scans (9.97 mm/week (95% confidence interval 9.17 to 10.78 mm) v 10.09 mm/week (95% confidence interval 8.88 to 11.31 mm)). Head circumference measurements were within the normal range for each week of gestational age4 and were not different between babies having initial and follow up scans at 35–37 weeks gestation (33.0 (2.0) v 32.2 (1.9) cm; p = 0.31) (fig 3).
{kind=link}
{kind=link}
{kind=link}
Box plot of head circumference measurements at each gestational week of age. Bars show interquartile range, the middle line indicates the median, and whiskers indicate the 10th and 90th centiles. For initial scans, n = 196 (range 6–25 for each week), and for follow up scans, n = 156 (range 4–25 for each week).
DISCUSSION
Our results are, to our knowledge, the first reported normal values for the width of the subarachnoid space in preterm infants. In addition, we have shown a clear difference in the width of the subarachnoid space between initial and follow up scans in infants of the same postmenstrual age.
In our unit, linear array scans complement sector scans in that they provide more detailed information on the meningeal space, the subarachnoid space, and the cerebral cortex.5 Measurements of the subarachnoid space using sonography were first reported in 1982, but there are few studies showing values in infants with no underlying intracranial pathology. Libicher and Troger1 studied 89 infants (none of whom were preterm or newborn) and found that the width of the subarachnoid space was less than 4 mm in 95% of cases. Frankel et al2 reported findings for 82 newborn infants: the width of the subarachnoid space was less than 3.5 mm in 95% of cases. Our findings for preterm infants are consistent with these studies of older infants. It is possible that head shape and position when scanning may affect the measurements. Shape is difficult to quantify; all infants in the study were scanned while supine.
For our preterm population, head circumference measurements and increment in head circumference with gestation were within established normal ranges.4 It therefore seems likely that measurement of the subarachnoid space represents an indirect method of assessing and monitoring brain growth. This measurement can be easily obtained during cranial ultrasound examination, an investigation that is performed routinely in most neonatal units.
The difference between the width of the subarachnoid space in initial and follow up scans probably reflects the difference between intrauterine and extrauterine existence. Preterm infants receiving intensive care had larger subarachnoid spaces which increased in width at a faster rate than those of newborn preterm infants of the equivalent gestational age. Possible causes for this difference include decreased brain growth, increased volume of cerebrospinal fluid around the brain, or a combination of the two mechanisms. Production of cerebrospinal fluid is unlikely to explain this difference, as there was no difference in head size and head growth between initial and follow up measurements and hence between intrauterine and extrauterine existence. Our results therefore suggest that, for preterm infants, there is less brain growth during extrauterine existence than there would have been had the infant remained in utero. Magnetic resonance imaging of the brain of premature infants performed at term has shown that the cortical surface area is reduced.6 However, decreased cortical surface area appears to be associated with decreased brain volume only in the presence of periventricular leucomalacia.7 Our study excluded infants with known intracranial pathology including periventricular leucomalacia. Our results may therefore reflect brain growth of the “apparently normal” preterm infant.
Previous studies have suggested that head size is closely related to brain size in newborns,8 and slow head growth in preterm infants is associated with poor neurodevelopmental outcome.9 The increase in head circumference along centiles has therefore been widely regarded as a reassuring indicator of adequate postnatal brain growth in preterm infants. Our data suggest that such reassurance may not be warranted. Despite normal postnatal head growth, preterm infants in this study had wider subarachnoid spaces probably reflecting smaller brains than infants of the same postmenstrual age whose growth had continued in utero. Thus ultrasonographic measurement of subarachnoid space width may be more useful than measurement of head circumference for assessing adequacy of postnatal brain growth in preterm infants.
Our finding of poor brain growth in apparently normal growing preterm infants may reflect impaired nutrition in the extrauterine, as opposed to the intrauterine, environment during the period of rapid brain growth that occurs before term.10 Corticosteroids are also known to decrease brain growth in preterm rats3 and may be associated with adverse neurodevelopmental outcome in preterm infants.11–13 We therefore excluded from our study infants treated with corticosteroids after birth. Unfortunately, in this study, data were not available on exposure of infants to corticosteroids before birth. However, measurements of subarachnoid space width may be useful in future studies to monitor brain growth of preterm infants who have received corticosteroids before or after birth.
In conclusion, measurement of the subarachnoid space is a straightforward investigation in preterm infants. Our normal data should be useful in the evaluation of intracranial pathology in premature infants. Measurement of subarachnoid space width may also be useful in association with measurement of head circumference for monitoring brain growth. Our data suggest that growth of the brain in preterm infants growing ex utero may be slower than it would have been had the infant remained in utero.
Acknowledgments
We acknowledge the help of Sylvia Rae, Christine Sharp, Paul Dukes, Norbert Yee, and other sonographers and registrars who contributed to this study.