Article Text

Abstract
Objective: To evaluate the diagnostic accuracy of cranial ultrasound (CUS) for detection of neonatal arterial territory cerebral infarction in term infants.
Methods: CUS scans from term infants with neonatal magnetic resonance imaging (MRI) evidence of neonatal infarction were reviewed. The scans were grouped by acquisition time after birth: 1–3 days (early) or 4–14 days (late).
Results: Brain MRI showed infarction in the territory of the middle cerebral artery in 43 of 47 infants, anterior cerebral artery in one, and posterior cerebral artery in three. Twelve of the 47 had minor changes on MRI in the white matter in the contralateral hemisphere, and four infants had bilateral infarctions. The early CUS scans were abnormal in 68% of the infants; the late CUS scans were abnormal in 87%. The late CUS scans were correct for laterality and site of lesion in 25/47 (53%) infants. In six infants with smaller lesions of the cortical middle cerebral artery branch or lesions in the posterior cerebral artery territory, the CUS scans were persistently normal.
Conclusion: Normal early CUS scans do not exclude a diagnosis of neonatal stroke, although most scans are abnormal. CUS scans performed after day 3 were abnormal in 87% of infants. CUS scan findings were accurate for lesion laterality and site in 53%, and, in 34%, the scans showed abnormality strongly suggestive of infarction but not always site specific. For optimal prognostic information, infants with clinical histories or CUS scan findings suggestive of infarction should have a neonatal brain MRI scan.
- CUS, cranial ultrasound
- MCA, middle cerebral artery
- MRI, magnetic resonance image
- magnetic resonance imaging
- infarct
- stroke
- ultrasound
- brain
Statistics from Altmetric.com
It is increasingly recognised that arterial cerebral infarction is common among full term infants with normal Apgar scores, who present with seizures in the first 72 hours.1–,7 These infarcts can be shown on diffusion weighted imaging performed soon after the onset of the seizures but can be missed using cranial ultrasound (CUS) and also occasionally with conventional magnetic resonance imaging (MRI).3,8 In contrast, by the end of the first week, the lesions, although becoming less obvious on diffusion weighted imaging, are generally clearly seen on conventional MRI.
The diagnostic value of CUS scanning in this clinical context is controversial. A recent study9 has suggested that signs of cerebral infarction can only be detected from CUS in 30% of cases with evidence of arterial infarction on brain MRI, whereas we and others3,6 have reported that evidence of the lesions is present on CUS in most cases, particularly when the examination is performed a few days after the onset of the presenting symptoms. As CUS is the imaging modality that is most readily available and the first used in neonatal units, it is important to establish how reliable it is in detecting abnormality suggestive of neonatal cerebral infarction. The aim of this study was to assess CUS scans obtained in the first 2 weeks after birth, in full term infants with evidence of cerebral infarction in an arterial territory distribution on brain MRI. More specifically we wished to establish whether (a) the timing of the scan is important, (b) CUS allows the identification of all lesions seen on brain MRI, and (c) the changes seen on CUS are always suggestive of cerebral infarction in an arterial territory distribution.
SUBJECTS AND METHODS
The subjects described in this study were prospectively enrolled full term infants born at or referred to the Departments of Neonatology at the Hammersmith and Queen Charlotte’s Hospital, London, or to the Wilhelmina Children’s Hospital, Utrecht, between 1993 and 2003. Ethical permission for the MRI examination was obtained from the research ethics committee in each hospital, and parental permission was given in each case. Infants were included if they had evidence of cerebral infarction in an arterial territory on brain MRI obtained in the neonatal period and had at least one CUS performed in the first 3 days after birth and one between days 4 and 14.
MRI
Imaging was performed on a 1.0 T Picker HPQ system in London or on a 1.5 T Philips ACS-NT system (Best, the Netherlands), using conventional T1 weighted, T2 weighted, and spin echo inversion recovery sequences. Most infants had more than one MRI scan, but for this study we only assessed scans obtained between one and three weeks after birth. The scans were assessed by independent observers (MR and FG) who were blind to the type or extent of lesion on CUS.
The infarcts were classified according to the arterial distribution of the lesions. The infarcts in the middle cerebral artery (MCA) territory were further subdivided into main branch territory or cortical or lenticulostriate branch territory.
CUS
Infants in both units were scanned with an ATL Ultramark 4 mechanical sector scanner with a multifrequency transducer (5–7.5–10 MHz crystals) using the anterior fontanelle as the acoustic window. Each child was scanned at least once in the first three days after birth, soon after the onset of seizures, and scanned again usually towards the end of the first week (age range 4–14 days). Both early and late CUS images were assessed for normal anatomy, ventricular size, and evidence of focal or diffusely increased echogenicity within the cerebral hemispheres and basal ganglia suggestive of infarction. The scans were also retrospectively evaluated from paper printouts in standard planes by two independent observers (LB and LdV) unaware of the type and the extent of lesion on brain MRI.
Abnormal scans were first classified according to the shape, extent, and localisation of the echogenic area(s) as follows:
triangular wedge shaped echogenic area with a linear demarcation previously reported as typical of arterial cerebral infarction10 (fig 1⇓)
focal non-typical regions of echogenicity mainly within one hemisphere (figs 2B⇓ and 3⇓)
focal unilateral echogenicity limited to the basal ganglia and/or thalami (fig 4⇓)
bilateral echogenicities without a clear predominant focal lesion (fig 2A⇓)

A typical triangular area of echogenicity in the right hemisphere indicating a right main branch middle cerebral artery (MCA) infarction is seen on the mid-coronal 7.5 MHz cranial ultrasound scan (A). The right basal ganglia and thalamus also appear slightly echogenic (arrowhead) but not sufficiently so to be sure of involvement within the infarction. (B) A right main branch MCA territory infarction (arrow) is demarcated on the T1 weighted axial magnetic resonance image. There is increased signal (short T1) along the lateral border of the right lentiform nucleus and low signal (long T1) in the right thalamus (arrowhead). (C) On diffusion weighted imaging, in addition to the right MCA, there is a smaller region of infarction in the left hemisphere that was not detected on ultrasound.
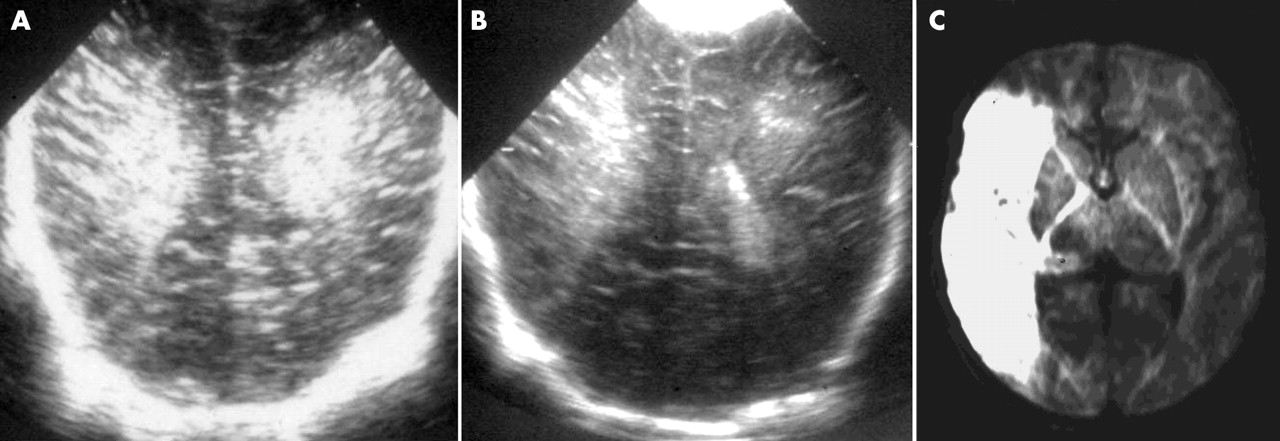
(A) Bilateral hemispheric echogenicity on the overloaded (excessive bony shadowing) 5 MHz coronal ultrasound scan. This example was not used in the analysis. (B) Bilateral abnormality is also seen on the 7.5 MHz ultrasound scan performed at the same time, but now better defined and predominant on the right. (C) A main branch right middle cerebral artery territory infarction only is seen on the axial diffusion weighted magnetic resonance image. A small haemorrhage was seen at the level of the centrum semiovale in the left hemisphere on the magnetic resonance image (not shown) correlating with the echogenicity seen in the left hemisphere on the ultrasound scan.

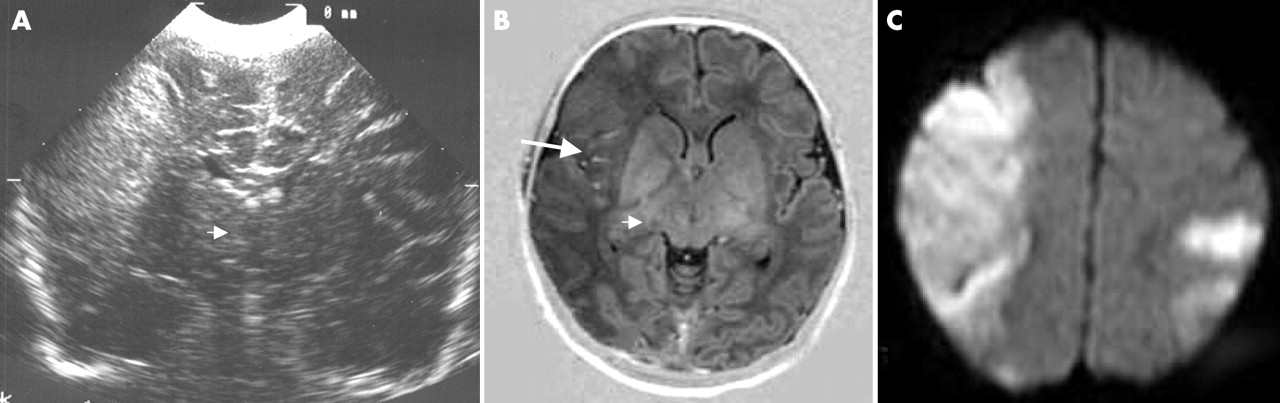
(A,B) Minor patchy echogenicity (white arrows) on the ultrasound scans within the right hemisphere (image tilted to show echogenicity maximally) which would not be considered diagnostic of an infarction. The two axial (C,D) and one parasagittal (E) T2 weighted magnetic resonance images show an infarction in right posterior middle cerebral artery branch territory (black arrows).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Parasagittal (A,B) and coronal (C) ultrasound scans showing a bright area of echogenicity with the left basal ganglia typical of a lenticulostriate infarction. These findings correlate well with the infarction seen in the left lentiform nucleus on the axial T1 weighted magnetic resonance image (D). On the more medial parasagittal ultrasound scan (B), an area of echogenicity is seen in the trigone that does not correlate with an area of infarction on the magnetic resonance image (D).
Minor changes such as small flares or haemorrhages either ipsilateral or contralateral when associated with predominantly unilateral focal changes (triangular or not typical) were also noted.
RESULTS
Forty seven full term infants were enrolled in the study. Forty five of them presented with convulsions in the first days after birth, but in two the infarct was an incidental finding when the infant was scanned on day 2 as part of a normal control group. All but three infants had normal Apgar scores at five minutes (⩾8). None of the 47 infants was receiving extracorporeal membrane oxygenation or had congenital heart disease, and none had long lines or catheters inserted before their initial symptomatology, none had overt infection or disseminated intravascular coagulation, and none had been part of a twin to twin transfusion syndrome.
MRI
Forty three of the 47 infants had an infarct in the territory of the MCA, one in the territory of the anterior cerebral artery, and three in the territory of the posterior cerebral artery. In all 47, conventional and diffusion weighted MR images showed evidence of an acutely evolving lesion. There was no evidence from MRI that the infarcts were established antenatally.
Of the 43 children with MCA infarction, 10 had involvement of the main branch (figs 1B,C⇑ and 2C⇑), 28 had involvement of one or more cortical branches (figs 1C⇑ and 3C–E⇑), and five had lesions localised only to the territory of the lenticulostriate branches (fig 4D⇑).
Thirty one of the 47 infants had entirely unilateral abnormality, 12 had a predominantly unilateral lesion with minor contralateral changes, and four infants had bilateral infarction.
CUS
Forty six infants had an early scan (day 1–3). These scans showed some abnormality in 32 (68%) but were normal in 14 (32%). The CUS performed after day 4 allowed the detection of abnormality in 87% of the infants.
Comparison between late CUS and type of lesion on MRI
Table 1⇓ shows details of the correlation between CUS and MRI. Details of the CUS and MRI scans for each infant are available from the authors.
Correlation between ultrasound performed after day 4 and magnetic resonance imaging (MRI) findings
Typical triangular shape hemispheric ultrasound echogenicity (n = 13; fig 1A, 2B⇑⇑). Twelve children had a typical focal triangular shape in the territory of the MCA; seven of the 12 had a main branch and five a cortical branch infarction on MRI. Another child had a triangular shaped area of echogenicity in the anterior territory on CUS scan and had a lesion in the territory of the anterior cerebral artery on MRI.
Non-typical focal unilateral hemispheric CUS echogenicity (n = 15; fig 3A⇑,B). Fourteen children had non-typical focal CUS echogenicity in the territory of the MCA; three of the 14 had main branch and 11 had cortical branch infarction on MRI. One child had a focal non-typical CUS echogenicity posterior lesion and had a posterior cerebral artery territory infarction on MRI. Although these infants had a dominant unilateral abnormality, other areas of echogenicity were seen that did not always correlate with abnormality on MRI.
Isolated basal ganglia/thalamic CUS echogenicity (n = 7; fig 4A⇑,B). Seven children had isolated basal ganglia/thalamic CUS echogenicity, which was localised to the basal ganglia only in five of the seven, to the head of caudate and thalamus in one, and to the thalamus only in another one. Of the first five, two had a cortical branch territory infarction, and three had lenticulostriate territory infarction on MRI. One child with caudate and thalamic echogenicity on CUS also had a lenticulostriate territory infarction on MRI. Another child had a unilateral thalamic lesion seen on both CUS and MRI. Seven infants with focal basal ganglia/thalamic echogenicity in association with hemispheric echogenicity are included in sections (a) and (b).
“Non-typical” bilateral focal hemispheric CUS echogenicity (n = 6). Six infants had bilateral focal but not triangular echogenicity on CUS suggestive of infarction; all six had a cortical branch infarction on MRI.
Normal CUS (n = 6). Six children had normal CUS scans after day 4. Four of the six had small unilateral cortical branch infarction, and two had a posterior cerebral artery territory infarction on MRI.
Comparison between late CUS and side of lesion on MRI
Table 2⇓ shows details of the correlation.
Correlation between side of lesion on late ultrasound and magnetic resonance imaging (MRI)
Twenty seven children had focal unilateral lesions on CUS: 20 of the 27 also had unilateral focal lesions on MRI, and seven had either contralateral changes (six) or bilateral infarcts (one) on MRI. Eight infants had a predominantly focal unilateral lesion with mild contralateral periventricular changes on CUS: two had unilateral, four had contralateral changes, and two bilateral infarction on MRI. Six children had bilateral focal lesions on CUS: three of the six had unilateral lesions on MRI, and the other three had either contralateral changes (two) or bilateral infarcts (one) on MRI. The later CUS images were correct for laterality and site of lesion in 25/47 (53%) infants.
DISCUSSION
The results of our study show that early CUS in infants with cerebral infarct can detect evidence suggestive of infarction in 68% of cases soon after the onset of seizures. This percentage increases to 87% when the scans are performed after day 4.
Our findings are in contrast with the recent observation that only 30% of CUS images show signs of cerebral infarction in infants with arterial infarcts on brain MRI.9 In that study there are no details of when CUS was performed, but it is reported that, in many cases, it was performed in the referring hospital before transfer, and therefore probably in the first days after birth. Our results show that, even if scans are performed soon after the onset of seizures, the detection rate for some abnormality is as high as 68%.
The six children whose CUS images were still normal after day 4 had relatively small infarcts in the territory of either the posterior cerebral artery or the posterior cortical branches of the MCA. They were all at least 12 months old, and none showed signs of hemiplegia, which is generally obvious by this age.11,12
Only 13 of the 47 patients in our study had the typical triangular shaped area of echogenicity previously reported to be diagnostic of MCA infarction.5,10 The triangular shape was more often, but not always, associated with larger infarcts in the territory of the main branch of the MCA. In contrast, cortical branches were more often associated with non-specific focal lesions that did not have the typical triangular shape.
The correlation between site of lesions on CUS and MRI was also not always good. In 25 of the 47 children (53%), there was concordance of site between MRI and CUS. A limitation of this study is that CUS was performed by various investigators as part of routine investigations and retrospectively evaluated from printouts in standard plans. The advantage of our study is that the CUS images used reflect the quality of those obtained in daily practice in many neonatal units. We accept that a more structured prospective study with all scans obtained by experienced examiners may increase the rate and the accuracy of detection of CUS, especially if scans were routinely obtained through both the anterior and posterior fontanelles.13 Such a study with large numbers would be difficult to achieve, as neonatal stroke is a relatively rare event and most infants are transferred to centres after the onset of symptoms.
Despite the limitations outlined above, we found that CUS does allow the detection of abnormality suggestive of focal ischaemic abnormality in almost all infants with lesions likely to lead to hemiplegia. However, as precise detail of the size and location of an infarct is less reliably determined from CUS, a brain MRI scan should be performed in the neonatal period in all infants with early seizures in order to obtain optimal information for diagnostic and prognostic purposes.
Acknowledgments
We thank Lilly Dubowitz and Jackie Pennock whose especial and ongoing interest in the presentation, investigation, and clinical outcome of neonatal infarction is the basis for this paper. We also thank the staff of the Robert Steiner MRI Unit and the nurses, junior doctors, and consultant colleagues involved in the referral and care of these infants. We appreciate enormously the parental support we have in following regularly the children in this study.
REFERENCES
Footnotes
Competing interests: none declared