Article Text

Abstract
Background: Hypothermia has been shown to be neuroprotective in animal models of hypoxia-ischaemia. It is currently being evaluated as a potentially therapeutic option in the management of neonatal hypoxic-ischaemic encephalopathy. However, significant hypothermia has adverse systemic effects. It has also recently been found that the stress of being cold can abolish the neuroprotective effects of hypothermia. It is hypothesised that selective head cooling (SHC) while maintaining normal core temperature would enable local hypothermic neuroprotection while limiting the stress and side effects of hypothermia.
Objective: To determine whether it is possible to induce moderate cerebral hypothermia in the deep brain of the piglet while maintaining the body at normothermia (39°C).
Methods: Six piglets (<48 hours old) were anaesthetised, and temperature probes inserted into the brain. Temperature was measured at different depths from the brain surface (21 mm (Tdeep brain) to 7 mm (Tsuperficial brain)). After a 45 minute global hypoxic-ischaemic insult, each piglet was head cooled for seven hours using a cap circulated with cold water (median 8.9°C (interquartile range 7.5–14)) wrapped around the head. Radiant overhead heating was used to warm the body during cooling.
Results: During SHC it was possible to cool the brain while maintaining a normal core temperature. The mean (SD) Tdeep brain during the seven hour cooling period was 31.1 (4.9)°C while Trectal remained stable at 38.8 (0.4)°C. The mean Trectal−Tdeep brain difference throughout the cooling period was 9.8 (6.1)°C. The mean Tskin required was 40.8 (1.1)°C. There was no evidence of skin damage secondary to these skin temperatures. During cooling only one piglet shivered.
Conclusions: It is possible to maintain systemic normothermia in piglets while significantly cooling the deeper structures of the brain. This method of cooling may further limit the side effects associated with systemic hypothermia and be feasible for premature infants.
- EEG, electroencephalography
- HI, hypoxic-ischaemic
- SHC, selective head cooling
- Trectal, rectal temperature
- Tscalp, scalp temperature
- Tdeep brain, temperature at ∼21 mm brain depth
- Tmid-brain, temperature at ∼14 mm brain depth
- Tsuperficial brain, temperature at ∼7 mm brain depth
- Tskin, skin (thigh) temperature
- Tcap, cap (circulating water) temperature
- selective head cooling
- hypothermia
- hypoxia-ischaemia
- piglet
- normothermia
Statistics from Altmetric.com
- EEG, electroencephalography
- HI, hypoxic-ischaemic
- SHC, selective head cooling
- Trectal, rectal temperature
- Tscalp, scalp temperature
- Tdeep brain, temperature at ∼21 mm brain depth
- Tmid-brain, temperature at ∼14 mm brain depth
- Tsuperficial brain, temperature at ∼7 mm brain depth
- Tskin, skin (thigh) temperature
- Tcap, cap (circulating water) temperature
Hypothermia after an hypoxic-ischaemic (HI) insult is neuroprotective in both human adults1,2 and neonatal animal models.3 Hypothermia is currently being applied in several large randomised studies to determine whether it is neuroprotective in human infants. A recent study of hypothermia after perinatal asphyxia in newborn infants showed a reduction in the number of children with cerebral palsy, except in those with the most severe brain injury.4 However, there are several worrying systemic effects of hypothermia, including potentially adverse effects on the cardiovascular, respiratory, immune, and haematological systems.5 Although safety data from pilot human studies have not shown any major deleterious effects after 72 hours of cooling,4,6,7 the deeper the hypothermia, the more these side effects may become manifest. We have shown experimentally that the stress of being cold can nullify the neuroprotective effects of hypothermia.8 Therefore cooling only the head while maintaining normal core temperature has been proposed as a method of limiting further the stress and side effects of hypothermia.
Until now the main suggested application of hypothermia (within neonatal medicine) has been in the treatment of term infants with severe birth asphyxia,9 which accounts for one to two per 1000 live births in the United Kingdom. This condition is a major cause of both perinatal mortality and long term neurodisability.10 This approach has unfortunately missed the largest neonatal population suffering from long term neurodisability, which is the surviving preterm infant.11 Within this group, hypothermia has not been suggested as a neuroprotective treatment because of strong evidence that it is associated with both increased morbidity and mortality.12,11
Although the aetiology of preterm brain injury is not entirely clear,13 many of these infants will have damage secondary to HI,14 and hence hypothermia, if applied safely, could have a neuroprotective role.
Until recently, there have been only two ways of inducing cerebral hypothermia in infants (either total body cooling or head cooling combined with mild systemic hypothermia), both of which are associated with systemic hypothermia.
We have previously shown (using the Cool Care head cooling system; Olympic Medical, Seattle, Washington, USA) that it is possible to cool the brain to 5°C lower than core temperature15 while allowing mild systemic hypothermia (Trectal 35°C), and that, once established, the Trectal−Tdeep brain gradient is stable for at least 24 hours. However, this degree of systemic hypothermia would not be acceptable in preterm infants.
The aim of this study was to determine whether it is possible to perform pure selective head cooling (SHC) and cool only the brain while maintaining total body normothermia, using both cooling and warming temperatures that could feasibly be applied in the preterm infant after HI.
METHODS
Animal preparation
All work was carried out under Home Office licence in accordance with United Kingdom guidelines. Six crossbred Landrace/Large White piglets with postnatal age <48 hours and median weight of 1550 g (range 1170–1890) were obtained from an approved farm on the morning of the study. The piglets were maintained and monitored before, during, and after a severe, transient HI insult in accordance with the procedures reported previously.16
Anaesthesia and ventilation
Unrestrained animals were anaesthetised with 2.0% halothane and nitrous oxide in a closed Perspex box, followed by transfer to an open incubator (Giraffe; Datex-Ohmeda, Hatfield, Hertfordshire, UK) for endotracheal intubation and mechanical ventilation (SLE 2000; SLE, South Croydon, Surrey, UK) with 0.7% halothane, 65% nitrous oxide, and ∼35% oxygen. Ventilation settings were adjusted to keep end tidal carbon dioxide between 4.5 and 5.5 kPa during the study (except during the insult, when these settings were not changed). Before and after the HI insult, the inspired oxygen fraction was adjusted to maintain transcutaneous oxygen saturation between 95% and 98% (Masimo SET; Masimo Corporation, Irvine, California, USA). Nitrous oxide was discontinued 30 minutes before the insult, but halothane was continued until after the insult when head cooling was started. At this point, intravenous anaesthesia was initiated with a bolus dose of 4 mg/kg propofol and 30 μg/kg fentanyl followed by maintenance infusions of propofol (4–12 mg/kg/h) and fentanyl (10 μg/kg/h) for the seven hours of cooling until rewarming began. Pancuronium bromide (100 μg/kg) was given as required during cooling to prevent prolonged shivering.
Vascular access and fluids
An ear vein was cannulated, and a 3.75% dextrose/0.45% saline infusion was started at 10 ml/kg/h before the insult. After the insult, 5% dextrose/0.45% saline was run at 5 ml/kg/h to keep blood glucose within the desired range of 3–10 mmol/l (measured using Precision Plus glucose electrodes; Medisense UK Ltd, Abingdon, Oxfordshire, UK). Umbilical arterial and venous catheters were inserted to allow repeated blood gas sampling (Radiometer, Crawley, West Sussex, UK) and the infusion of fluids and drugs.
Cardiac monitoring
Continuous mean arterial blood pressure was measured from the umbilical artery catheter, and three lead electrocardiographic monitoring (IVY Biomedical, Branford, Connecticut, USA) was undertaken. During the insult, no lower limit for mean arterial blood pressure was set (unless it was associated with progressive bradycardia); otherwise a pressure <40 mm Hg during the study period was treated with up to two 10 ml/kg boluses of 0.9% saline followed, if it remained unsatisfactory, by inotropic support with dopamine (range 5–20 μg/kg/min).
Temperature monitoring
Temperatures were recorded from a rectal probe (Trectal) inserted to 6 cm from the anal margin and from surface probes placed on the thigh (Tskin) and scalp (Tscalp) (400 series; Yellow Springs Instrument Co, Yellow Springs, Ohio, USA). To measure intracerebral temperature at different depths, one temperature probe (containing three thermocouples 7 mm apart) was inserted into the brain at a depth of 2.2 cm from the brain surface (IT18-3 thermocouple; Physitemp Instruments Ltd, Clifton, New Jersey, USA). The deepest thermocouple recorded Tdeep brain (depth ∼21 mm), the most superficial probe recorded Tsuperficial (∼7 mm depth), and the probe in between recorded Tmid-brain (∼14 mm depth). The probe was embedded into a 1.0 cm diameter disc moulded from dental acrylic, which was sealed into an artificially made lateral fontanelle caudal to the bregma (as the newborn piglet has no patent fontanelle). Each probe was calibrated to within ±0.1°C, over a temperature range 20–40°C, against a certified mercury-in-glass thermometer (Zeal, London, UK). The rectal, skin, scalp, and intracerebral temperatures were recorded and stored at one minute intervals. The piglets were kept in an open incubator with sides 30 cm tall (Giraffe Incubator; Datex-Ohmeda). During the baseline period, the normal piglet core temperature of 39°C was maintained by an overhead radiant heater with a variable output from 0% to 100%, positioned 80 cm above the piglet. During cooling, an insulating shield (Olympic Medical) incorporating reflective aluminium foil was placed over the piglet’s head, to ensure that the overhead heater warmed only the exposed body below the neck.
Electroencephalographic (EEG) monitoring
Single channel parietal (interelectrode distance of 3 cm) EEG was recorded during the insult and cooling-rewarming periods (Oxford Medilog 9000; Oxford Medical Systems Ltd, Abingdon, Oxfordshire, UK), as were amplitude integrated EEG recordings (Lectromed CFM monitor 60110; Olympic Medical).
Head cooling cap
A custom made cooling cap (Cool Care System; Olympic Medical) with a network of circulating water channels was used in this study. The volume of water held in the cap was ∼75 ml, and water circulated through the cap at 750 ml per minute. The cap was fitted around the head and snout, avoiding contact with the neck. A disposable nappy was firmly secured over the cap to act as an outer insulating layer. The temperature of the circulating water was adjustable between 5 and 26°C as required throughout the cooling period.
After insertion of all the monitoring equipment, the piglet was placed in a prone position and rested for a 60 minute stabilising period. The piglets were then subjected to a 45 minute HI insult16 followed by cap cooling for seven hours, followed in turn by passive cerebral rewarming. Cooling was started by circulating cooled water through the cap, initially set at 6°C, with the overhead heater turned on. Overhead heating power output was adjusted to maintain Trectal at 39°C—that is, normothermia for pigs. The desired steady state was achieved by adjusting the cap temperature to that which allowed the maximal overhead heating to maintain a stable rectal temperature of 39°C (the cap water temperature that stabilised the rectal and deep brain temperatures over the seven hour period was 8.9°C (7.5–14), median (interquartile range)). After seven hours, cerebral rewarming was started by turning off the circulating water flow but leaving both the cooling cap and overhead reflective barrier in situ.
Acute cerebral HI
The inspired oxygen concentration was reduced abruptly to 4–6% to reduce the real time EEG record to a background amplitude of <7 μV. The insult was terminated after 45 minutes, and the piglet resuscitated with an increased inspired oxygen fraction until transcutaneous oxygen saturation was maintained at 95–98%.
Histopathology
At the conclusion of the experiment, the brains were perfusion fixed, and, with the temperature probes in situ, left in 4% formaldehyde for seven days. The probes were then removed and the brain processed routinely for preparation of paraffin embedded blocks. The position of the temperature probe in each animal was confirmed from serially cut sections.
Data analysis
Data were stored and analysed using the software package Statview version 5.0.1 (Adept Scientific, Letchworth, Hertfordshire, UK). For comparisons of discrete variables within and between groups, Student’s t test (paired or unpaired) was used to compare parametric data, and Wilcoxon signed rank test for non-parametric data. Regression analysis was used to analyse associations between variables. p<0.05 was considered significant (two tailed testing).
RESULTS
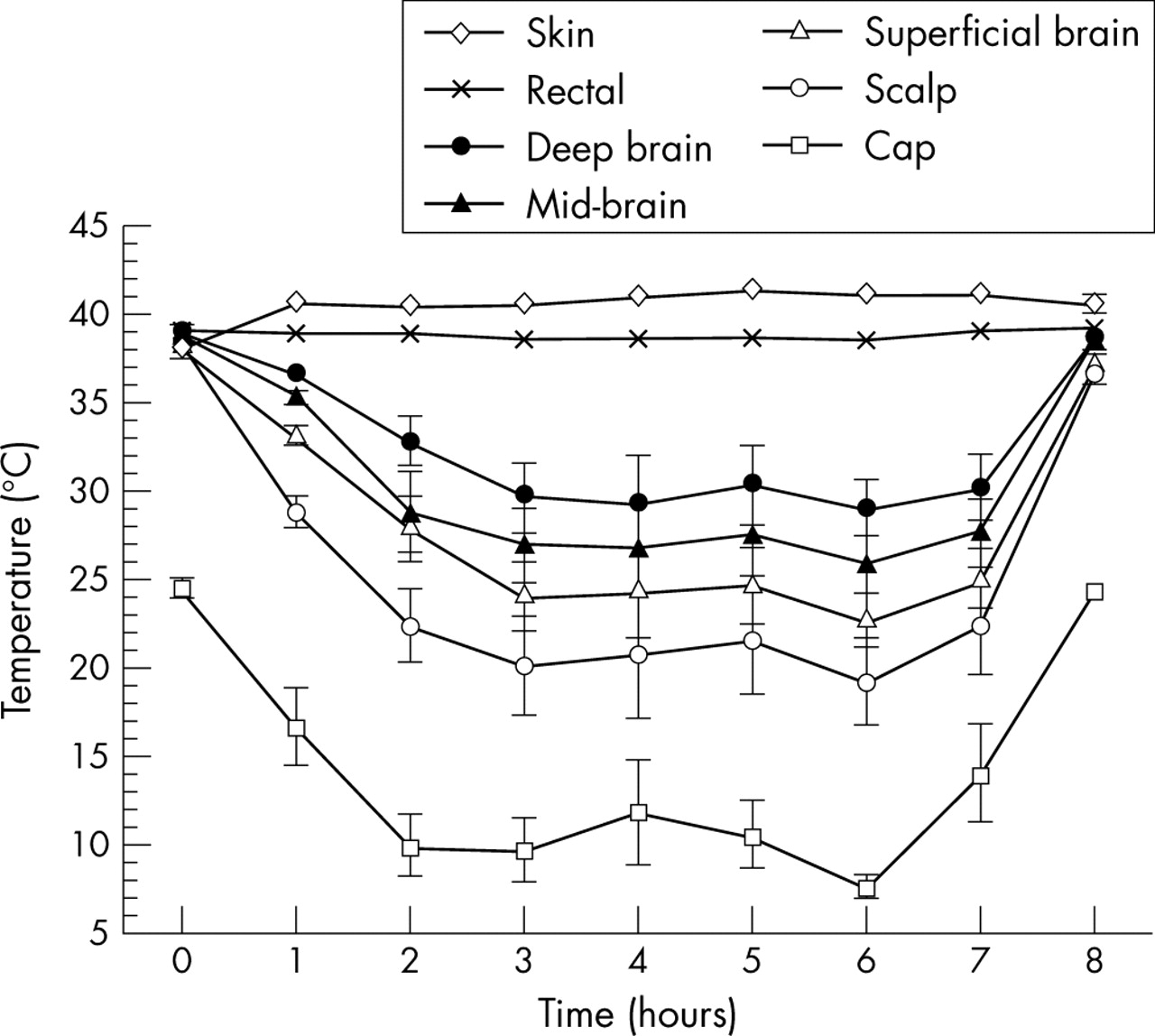
During SHC, it was possible to cool the brain while maintaining a normal systemic temperature (fig 1⇓). The mean (SD) Tdeep brain during the seven hour cooling period was 31.1 (4.9)°C while Trectal remained stable at 38.8 (0.4)°C. The mean Trectal–Tdeep brain difference throughout the cooling period was 9.8 (6.1)°C. A temperature gradient developed across the brain from superficial to deep structures during cooling. Mean Tscalp measurements were the lowest at 22.7 (6.2)°C, while Tsuperficial brain was 25.9 (5.4)°C.
{kind=link}
Temperature data from different sites in piglet brain during the seven hours of cooling, showing the temperature difference between rectal and deep brain. Values are mean (SE).
The ability to maintain this gradient did not decrease with time, and at the end of cooling it was still maintained at a mean of 9.4 (4.1)°C (table 1⇓). The ability to create this gradient was not influenced by either the size of the piglet or the severity of the HI insult (data not shown).
Temperature (°C) during the cooling-rewarming period
To maintain systemic normothermia and prevent hypothermia, it was necessary to use higher levels of radiant heat than previously reported. The mean Tskin required was 40.8 (1.1)°C compared with 38.1°C at baseline. We observed no evidence of skin damage secondary to these higher skin temperatures.
The mean (SD) time for Tdeep brain to return to normothermia after discontinuation of head cooling was short (36 (11) minutes), with a rate of temperature rise of ∼0.25°C per minute.
Table 2⇓ shows cardiovascular and physiological variables during the cooling-rewarming periods. Heart rate was not significantly different from baseline levels during the period of cooling, but was significantly higher than baseline at the end of the HI insult (p = 0.03). Blood pressure was not significantly different at any time point of the experiment (although three of the animals required more than two boluses of volume, and two of these required an infusion of dopamine to maintain a normal blood pressure).
Physiological variables during the cooling-rewarming period
During the cooling period, only one piglet shivered and required pancuronium (this was despite a Trectal of 39.2°C).
Histopathological analysis confirmed the position of the temperature probes in the basal ganglia and showed no evidence of either bleeding or injury to the superficial brain tissue.
DISCUSSION
We have recently shown in newborn piglets that it is possible to cool Tdeep brain to a lower temperature than Trectal after an HI insult (using cap temperatures of 6–24°C) while inducing mild systemic hypothermia.15 We have since confirmed that this method of achieving moderate cerebral hypothermia (brain temperature 30.1°C) along with mild total body hypothermia is effective at inducing neuroprotection in our piglet model of HI injury.3
However, the use of total body hypothermia is not thought to be safe in the care of newborn preterm infants, as there is a clear link between hypothermia and increased mortality in this group.12
The depth and duration of hypothermia that is necessary to induce neuroprotection is uncertain. Most human infant studies that are in progress induce hypothermia for 72 hours, which is based solely on experimental studies on fetal sheep.17 However, human adult studies of therapeutic hypothermia have shown a beneficial effect of 12 hours of hypothermia,1 and experimentally in newborn pigs only three hours of hypothermia is neuroprotective if started immediately after an HI insult.18
Previous studies have reported attempts at SHC with normothermia. Laptook et al19 attempted to selectively cool the brain only in a piglet model of HI but required ice cold water (1°C) and a warming blanket set at 45°C to maintain rectal temperature at normothermia. Despite these extreme temperatures, which would not be acceptable in neonatal practice, they could not lower brain temperature below 35°C. Moreover, when hypoxia was applied during SHC, the deep brain temperature rose markedly and the Trectal–Tdeep brain gradient fell to about 1°C. Iwata et al20 also found that, in normothermic pigs, they were only able to induce mild selective cerebral hypothermia before an HI insult if the coolant temperature around the head was 0°C. Further attempts at inducing cerebral hypothermia using coolant temperatures of 10°C were not successful unless rectal temperature was allowed to fall by 1°C, and, even in this instance, deep brain temperature did not fall below 35°C. Neither of these experiments was performed after HI, and we have shown previously that the gradient between rectal and brain temperature is reduced after an HI Insult.21 In this study, however, using the Cool Care System and radiant overhead heating, we have been able to induce moderate cerebral hypothermia, producing cerebral temperatures that have been previously shown to be neuroprotective in our model.3
Several observations from these data require further comment. Firstly, no fall in heart rate was seen during this method of cooling. This is in contrast with our previous experience with head cooling associated with systemic hypothermia, when we found a fall in heart rate to 60% of normothermic values.3 This may have potential importance as it is thought that one of the mechanisms of hypothermic neuroprotection is reduced metabolic demand. Secondly, we have previously reported that stress may reduce the effectiveness of hypothermia as a neuroprotective treatment, and hypothermia has been shown to induce intense shivering and raised stress levels in the newborn pig.8 During combined SHC and mild systemic hypothermia, all piglets shivered and required paralysis to stop it.3 It was interesting that only one piglet in this study shivered and needed paralysis. Hence in five out of six piglets, there were no physiological attempts at thermogenesis despite the profoundly cold cerebral tissue, confirming that body skin temperature is the main sensory input for thermoregulation. Thirdly, this method of cooling does not appear to confer any beneficial effect on the cardiovascular system recovering from HI injury, as the proportion of pigs (50%) requiring inotropic support in this study was similar to that previously reported.
A concern regarding the safety of this method of SHC is the need to increase radiant heat to achieve skin temperatures as much as 2°C higher than core temperature. This increased heat input could lead to high evaporative water loss in a preterm human infant. However, this requirement for increased heat input may be species specific, as the pig has a thick epidermis with coarse hair and hence requires more heat to permeate through this barrier. In this model, there was no evidence of skin injury. Also in this particular set of experiments, our aim was to try to cool the brain as much as technically possible. In a true study of the protective effects of cerebral hypothermia, we would only aim to do this by 3–4°C (rather than the 9.8°C achieved in this study). Consequently less cooling and therefore less heating would be required. Another concern is the need to induce profound superficial cerebral hypothermia to achieve moderate hypothermia in the deep structures of the brain. Parkins et al,22 using a cold perfusion model of selective cooling in the canine brain, found that only temperatures below 12°C led to brain pathology from hypothermia per se. In our current study, histological examination found no evidence of cortical brain injury. This is in contrast with our previously reported results in which significant cortical damage was found after an HI insult at only six hours normothermic survival.23 In the present method of cerebral hypothermia, there appears to be a wide variation in the extent of deep cerebral hypothermia (SD 4.9°C). We previously speculated in our model paper of SHC combined with mild systemic hypothermia21 that this variation was due to multiple factors, including the severity of the HI insult and variations in cerebral blood flow (unpublished data).
The final concern about the safety of this method of SHC is the potentially deleterious effects of rapid changes in cerebral temperature during rewarming. Despite attempts to slow the rate of rewarming by keeping the cap full of cold water in situ (as a heat sink), cerebral temperature had returned to normothermia in all pigs in less than one hour, and these large abrupt changes in cerebral temperature of 0.25°C/min were accomplished solely by turning off the cooling machine. In the absence of measurements of deep brain temperature, these fluctuations would have gone unnoticed.
It is by no means certain that it is possible to selectively cool the newborn human brain (especially as there is as yet no way of measuring brain temperature safely). Corbett and Laptook24 were unable to show in the normal human adult a reduction in brain temperature of more than 0.4°C using localised head cooling leading to scalp temperatures of 16°C. Mellergard25 attempted to selectively head cool human adults and was unable to cool the deep brain at all using an “ice cap” surrounding the head. In fact, his studies showed that epidural temperature only fell by 1°C (whereas in our study we were able to reduce superficial brain temperature (7 mm deep) to 16°C below core temperature). A paper describing numerical modelling of heat exchange in the newborn human head postulated that it would not be possible to cool any tissue in the brain deeper than 2 cm from the scalp.26 This model did not take into account heat loss from arteriovenous heat exchange, which is known to be important.27 The fact that we were able to create a mean temperature gradient between Trectal and Tdeep brain of 9.8°C at this depth is very encouraging. One can speculate that it should be easier to cool a small, more immature brain with lower cerebral blood flow, as in the premature baby, than that of a large term infant.
The use of hypothermia as a treatment in premature brain injury requires further study in experimental models before its use in human infants. The aetiology of preterm perinatal brain injury is less clear than in the term infant, but HI plays an important role, not only in those injuries sustained around the time of birth,13 but also those sustained in the postnatal period. Until now, hypothermia has not been studied with any vigour in preterm models of brain injury because it was felt that the systemic effects would counteract any potential benefit. The piglets used in this study were healthy, born at term, and with brain maturation similar to that of a term human infant, and so cannot be used in this instance as a model of the preterm brain for the assessment of the neuroprotective effects of hypothermia. However, from a practical point of view, the head size and weight of the piglets in this study were of human preterm infant proportions. The head circumference of a newborn piglet is 26 cm, which is equivalent to a preterm infant at 27 weeks gestation. Our findings that it is possible to cool the brain without cooling the body will hopefully stimulate research into the benefit of hypothermia in the field of preterm brain injury.
CONCLUSION
We have shown in this study that it is possible to maintain systemic normothermia while significantly cooling the deeper structures of the brain after an HI insult. This method of cooling may further limit the side effects associated with systemic hypothermia and may be feasible for use in premature infants in experimental studies.
Acknowledgments
We are grateful for financial support from SPARKS (UK), The Laerdal Foundation for Acute Medicine, and the Wellcome Trust. We are also grateful to Olympic Medical for lending us the Cool Care System, Masimo Corporation for the pulse oximeter, Datex-Ohmeda for the Giraffe incubator, and Radiometer for the use of a blood gas analyser.
REFERENCES
Footnotes
Competing interests: none declared