
Abstract
SUMMARY: Failure to detect FCD and similar lesions encountered in patients with tuberous sclerosis can have significant clinical consequences, such as preventing surgical intervention for medically refractory epilepsy and misguiding prognostic information regarding cognitive development. Here, we show the beneficial effects on detection of FCD and cortical tubers when using a magnetization transfer T1 sequence for children with seizures who underwent MR imaging at our institution.
ABBREVIATIONS:
- EEG
- electroencephalogram
- FCD
- focal cortical dysplasia
- MT
- magnetization transfer
- MTI
- magnetization transfer imaging
Detection of focal cortical dysplasia in children by MR imaging can be difficult for a variety of reasons. First, findings can be masked in patients in whom myelination is still ongoing. Second, artifacts such as patient motion can mask lesions of FCD. Third, lesions maybe very subtle or go undetected when seen on only 1 conventional MR imaging sequence.
Focal cortical dysplasia is a common reason for drug-resistant epilepsy in children.1 Resection of FCD in a child with refractory focal epilepsy can result in seizure control and improve development.2
There are 3 types of FCD, as described in 2011 by the International League Against Epilepsy: type I with abnormal radial/tangential cortical layering, type II with abnormal cortical lamination in combination with dysmorphic neurons, type III with abnormal cortical lamination in combination with a principal lesion (hippocampal sclerosis, tumors, vascular malformations).3 Cortical tubers of tuberous sclerosis, a hereditary neurocutaneous disease,4 can be indistinguishable from FCD type II.5
Magnetization transfer enhances signal differences between water molecules that are free and mobile and those that are bound to the less mobile protons on T1-weighted images. An off-resonance radio-frequency impulse saturates protons bound to macromolecule tissue.6 When tissue integrity is altered, transfer of saturation effects between bound and free protons is disrupted, causing a bright signal on this sequence.6⇓–8
Here, we illustrate the beneficial effects of using MT T1 in the MR imaging of children with seizures.
Case Series
All MR imaging studies were performed on a 1.5T scanner (Signa; GE Healthcare, Milwaukee, Wisconsin). The study was approved by the institutional review board. Cases were chosen from the departmental neuroradiology teaching file. Specifically, only cases in which the diagnosis could have been definitely or easily missed without the use of magnetization transfer imaging in children were chosen. Imaging sequences at 1.5T considered for this report were the following: axial T2 (2-mm section thickness; TR, 4400 ms; TE, 80 ms); FLAIR (5-mm section thickness; TR, 10,000 ms; TE, 120 ms); for patients with epilepsy, a sagittal 3D spoiled gradient-echo T1 (TR, 12 ms; TE, 5 ms; NEX, 1; flip angle, 20°); and for patients with tuberous sclerosis, a sagittal spin-echo T1 (5-mm section thickness; TR, 430 ms; TE, 15 ms). The MT sequence parameters were the following: TR, 600 ms; TE, 15 ms; 256 × 192; 5 mm skip 1 mm; NEX, 2; MT offset, 600 kHz. The duration of the MTI sequence at 1.5T was ∼4 minutes. Figures were annotated by using the cross-reference function on the PACS system to accurately label lesion location across those different sequences that best showed the lesion besides the MTI sequence. Due to size limitations in this article, only 1 comparison sequence can be shown for most cases below; further imaging examples can be requested by contacting the authors.
Case 1
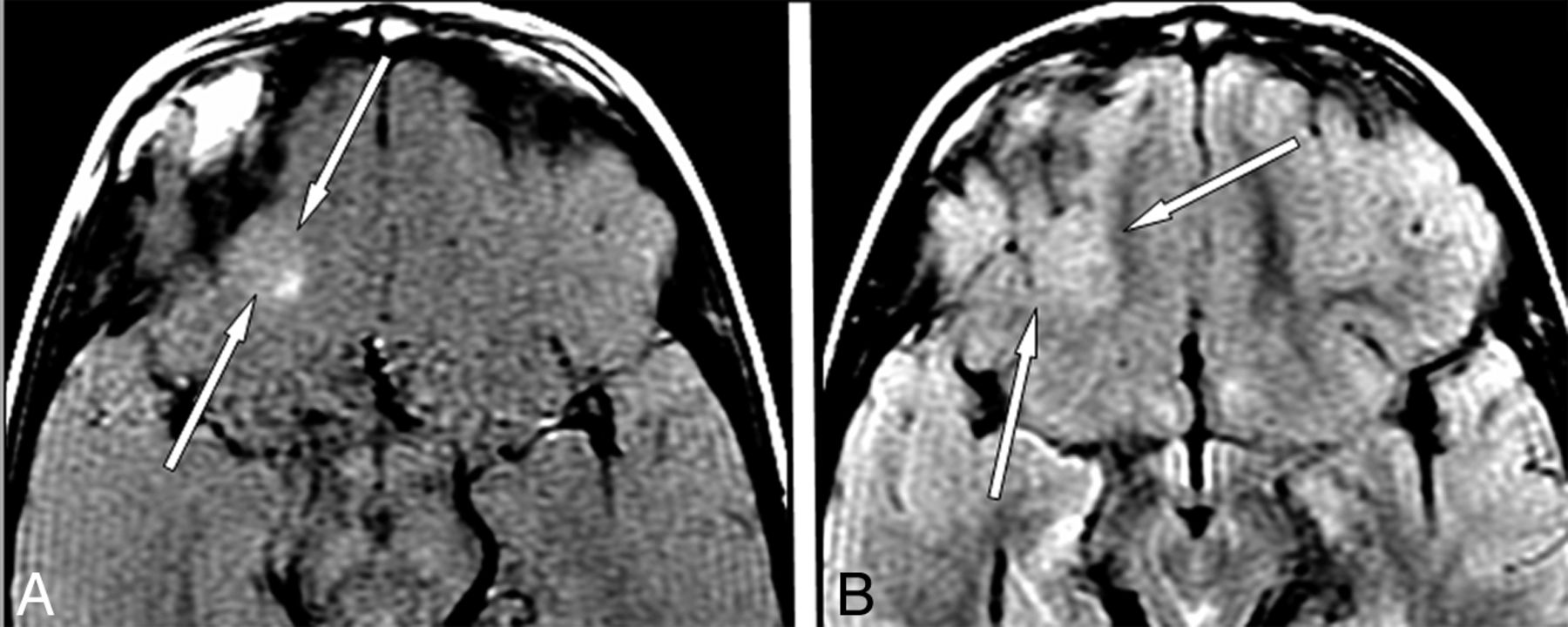
A 10-month-old boy presented with cardiac rhabdomyoma (Fig 1). The usefulness of MT is that the cortical dysplasia is only seen on MT T1 and not readily identified on any other sequence because of a background of immature frontal subcortical white matter.

A 10-month-old boy with cardiac rhabdomyoma. MR imaging axial T1 with MT (A) and axial T2 (B). There is a bright lesion on T1 with MT in the medial posterior left frontal cortex, representing a cortical tuber (long arrows, A). This abnormality cannot be reliably detected on the axial T2 image (B) and other sequences (not shown) with a background of incomplete myelination. The findings are compatible with cortical tuber of tuberous sclerosis (diagnosis confirmed clinically).
Case 2
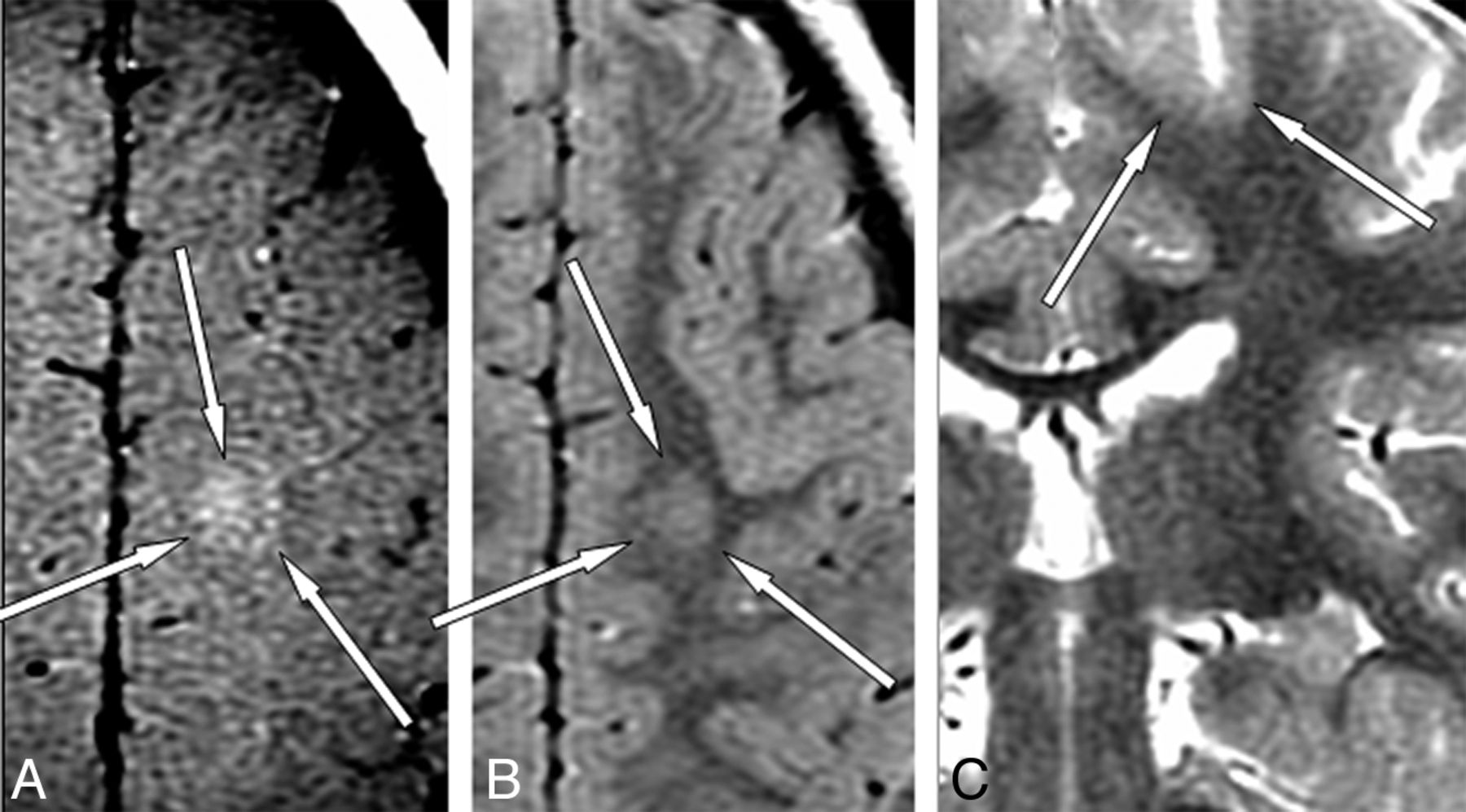
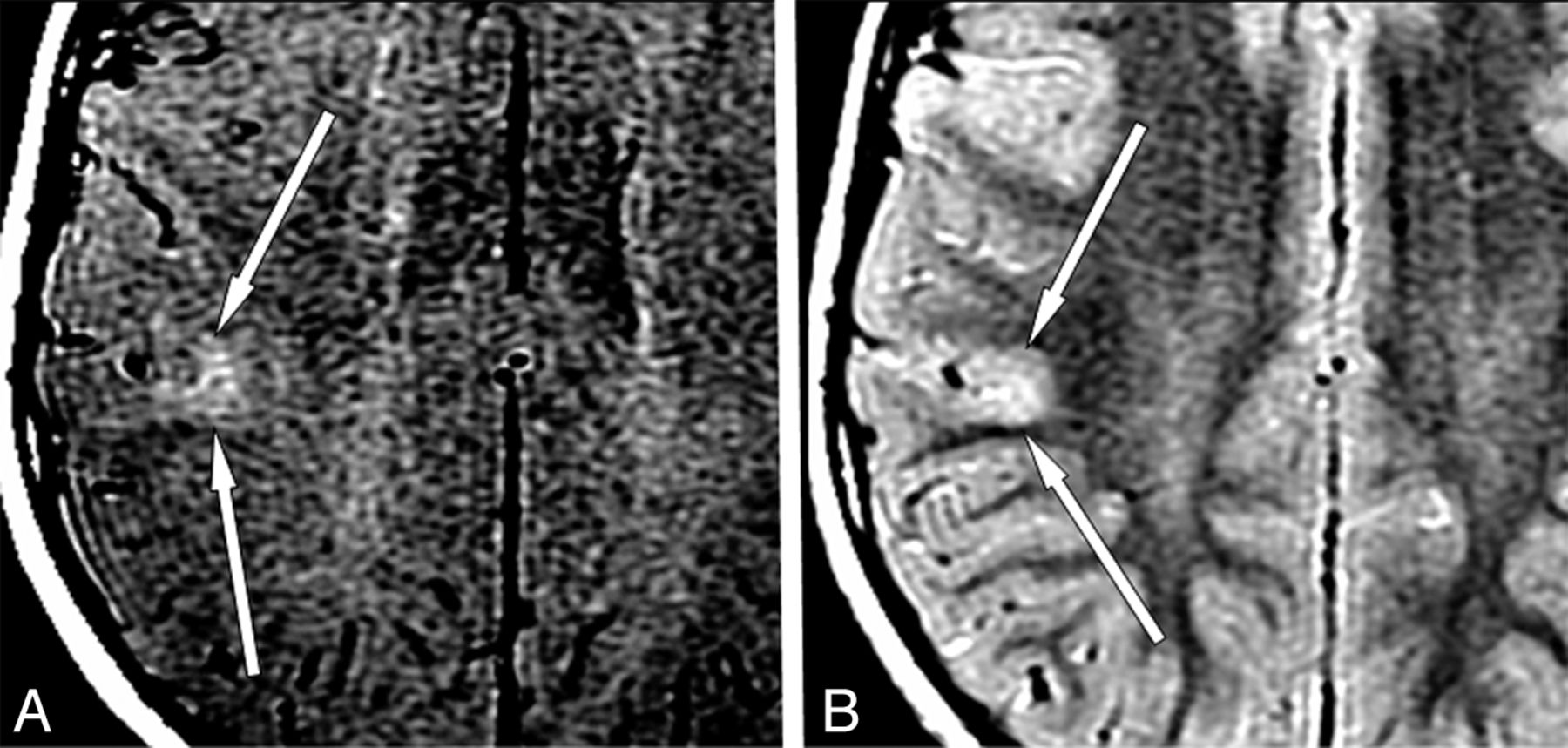
A 3-year-old boy presented with increased seizure activity (Fig 2). The usefulness of MT is that cortical dysplasia is best seen on MT T1 and not readily seen on any other sequence. Specifically, on axial FLAIR images the lesion resembles an area of volume-averaging.

A 3-year-old boy with increased seizure activity. MR imaging axial T1 with MT (A), axial FLAIR (B), and coronal T2 (C). Hyperintense lesion on T1 MT in the medial aspect of the left posterior frontal lobe (arrows, A) is seen. On axial FLAIR images, the lesion (arrows, B) is not readily identified and could be mistaken for volume-averaging. When one cross-references the lesion seen on T1 MT to the coronal T2 image (arrows, C), the lesion remains very subtle. The findings are compatible with focal cortical dysplasia (surgically confirmed).
Case 3
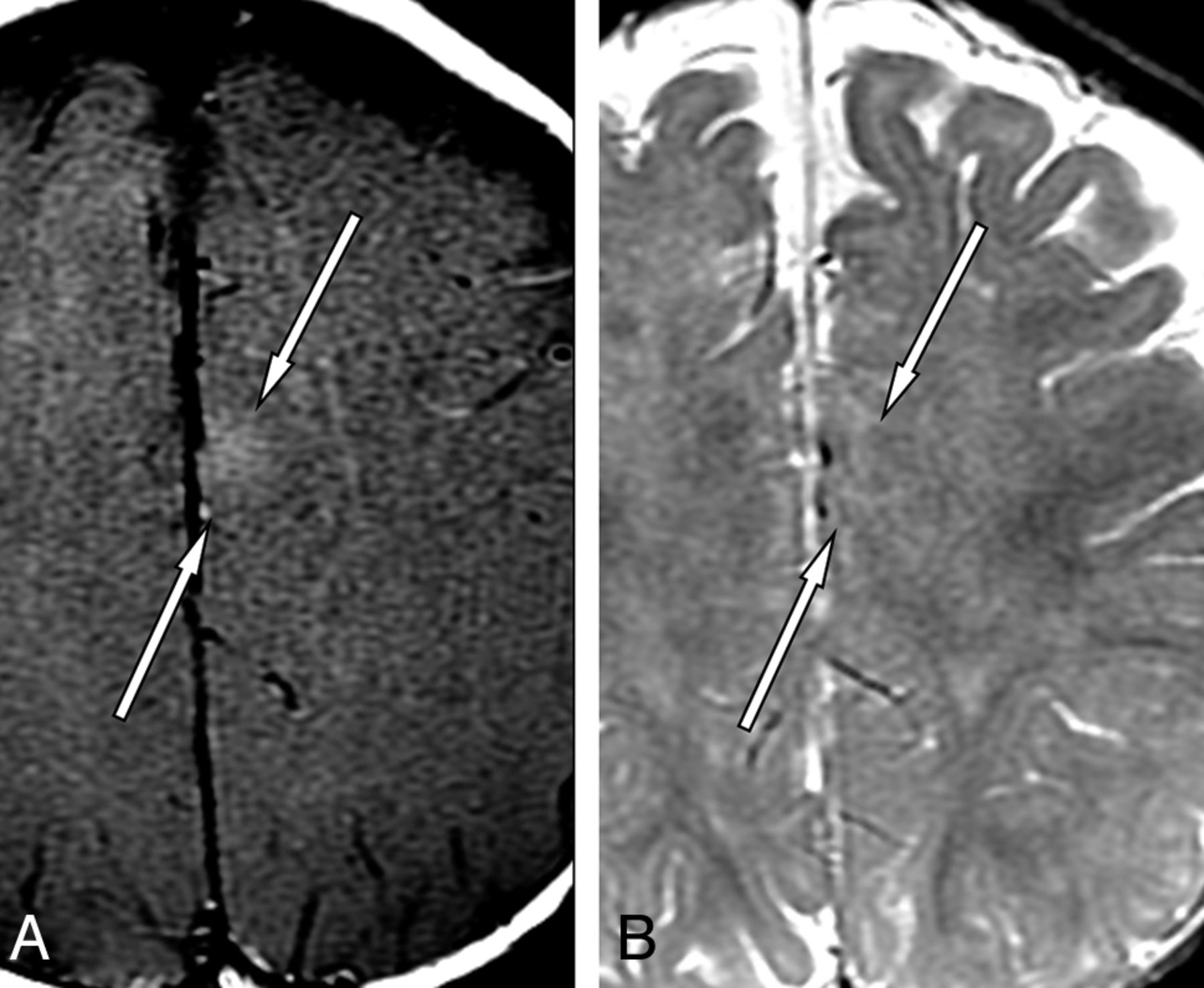
A 9-year-old boy presented with newly diagnosed seizures and a right anterior frontal focus on EEG (Fig 3). The usefulness of MT is that cortical dysplasia is best seen on MT T1 and is not readily identified on any other sequence because of its subtle nature and masking by superimposed artifacts from patient motion.

A 9-year-old boy with seizures and a right anterior frontal focus on EEG. MR imaging axial T1 with MT (A) and axial T2 (B). T1 with MT shows a linear hyperintense lesion in the right frontal lobe, extending from the subcortical white matter toward the ventricular wall (arrows, A). On the axial T2 image, the lesion is less well-visualized (arrows, B). The findings are compatible with focal cortical dysplasia (diagnosis confirmed clinically).
Case 4
A 12-year-old girl presented with tuberous sclerosis (Fig 4). The usefulness of MT is that T1 with MT shows superior detection of cortical tubers compared with other sequences in a maturely myelinated brain, preventing underestimation of the extent of brain involvement.
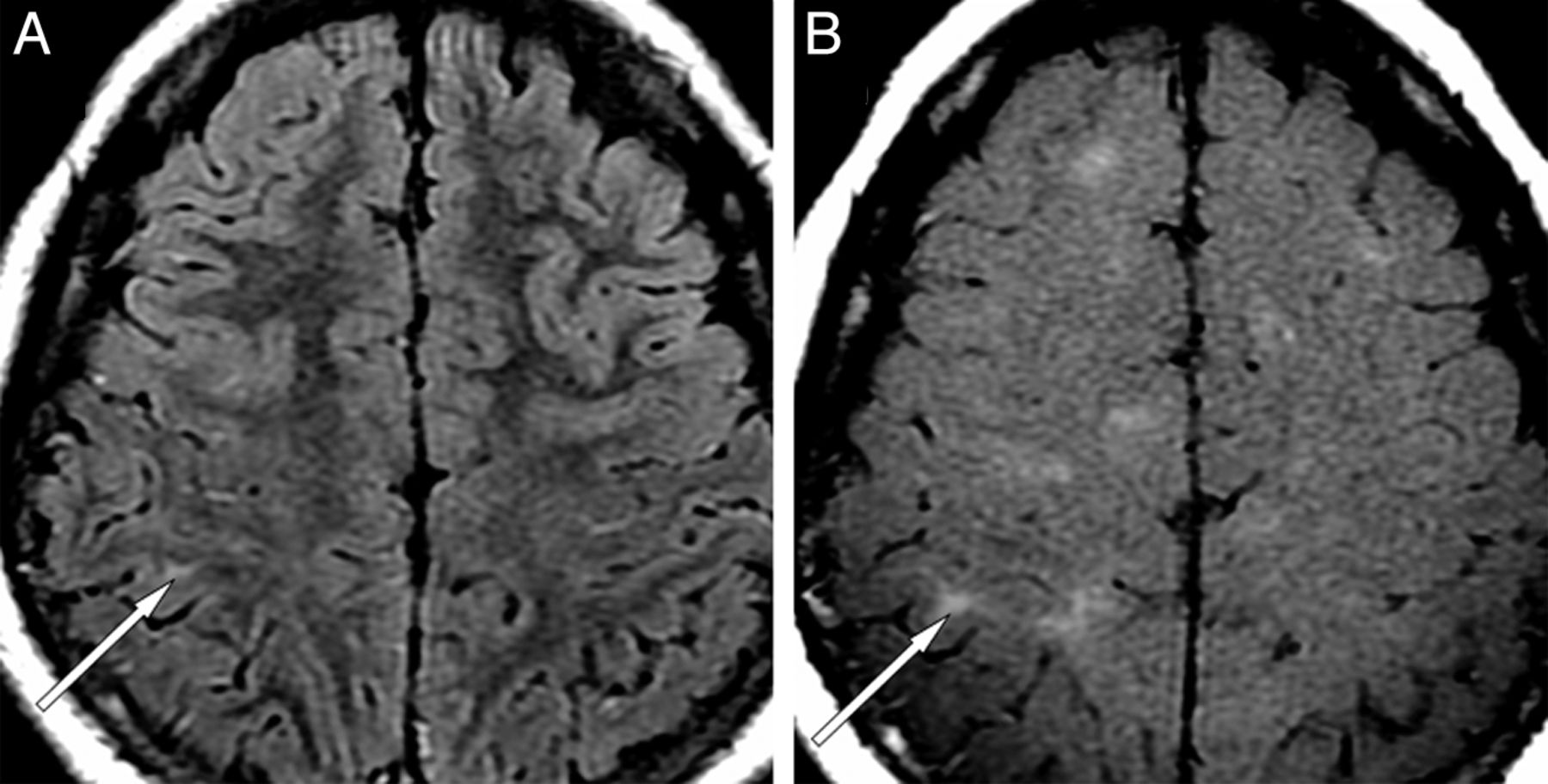
A 12-year-old girl with tuberous sclerosis. MR imaging axial FLAIR (A) and axial T1 with MT (B). When cross-referencing the multiple bright lesions on the T1 with the MT image (B, not marked by arrows), only 1 shows a bright signal correlate on FLAIR (arrows, A and B). Without the T1 with MT sequence, disease burden in this patient would be significantly underestimated (diagnosis made clinically).
Case 5
A 4-year-old boy presented with afebrile seizures (Fig 5). The usefulness of MT is that cortical dysplasia is best seen on MT T1. The lesion is more subtle on at least 1 other MR imaging sequence and could easily be missed.

A 4-year-old boy with afebrile seizures. Sequential images on MR imaging axial T2 (A), axial T1 with MT (B), and coronal T2 (C). On axial T2, there is very subtle increased thickness of the left posterior frontal lobe cortex with mild blurring of the gray-white matter junction (arrows, A). MR imaging axial T1 with magnetization transfer shows a corresponding distinct area of hyperintense signal with an irregular shape, located predominantly subcortically (arrows, B). The coronal T2-weighted image shows a gray-matter isointense linear lesion extending from the thickened cortex to the wall of the left lateral ventricle (arrows, C). The findings are compatible with focal cortical dysplasia (surgically confirmed).
Case 6
A 3-year-old boy presented with increasing seizure activity (Fig 6). The usefulness of MT is that cortical dysplasia is best seen on MT T1 and could be missed on the other sequences because of its location just above the orbit, which could be mistaken for susceptibility artifacts at the skull base.
A 3-year-old boy with increasing seizure activity. MR imaging axial T1 with MT (A) and axial FLAIR (B). There is a small hyperintense lesion in the supraorbital lateral inferior right frontal lobe on T1 with MT (arrows, A). Axial FLAIR image shows local increased cortical thickness in this area and subtle hyperintense signal (arrows, B). The findings are compatible with focal cortical dysplasia (not surgically confirmed).
Case 7
A 7-year-old boy presented with new seizures and EEG abnormality in the right temporal parietal area (Fig 7). The usefulness of MT is that cortical dysplasia is best seen on MT T1 and could be missed on other sequences because of its very small size and bright FLAIR signal only on a single section.

A 7-year-old boy with new seizures and an EEG abnormality in the right temporal parietal area. MR imaging axial T1 with MT (A) and axial FLAIR (B). T1 MT shows a small bright lesion in the right posterior frontal cortex (arrows, A). FLAIR image shows a focal hyperintense signal and minimal thickening of the frontal cortex without signal changes in the adjacent subcortical white matter (arrows, B), only seen on a single axial section in each sequence. The findings are compatible with focal cortical dysplasia (surgically confirmed).
Discussion
In children younger than 2 years of age, it can be difficult to identify localized or transmantle FCD on a background of immature white matter. Gray-white matter junction blurriness can be normal at certain stages of ongoing myelination. Cortical thickening may be seen on T2, proton attenuation, FLAIR, and T1-weighted images as partially myelinated white matter that becomes transiently isointense to the cortex during development.3 The benefit of using MT T1 in children with incomplete myelination is that it offers an additional opportunity to detect FCD that could otherwise be obscured (Fig 1).
Lesions of FCD may not be detectable on T1, T2, and FLAIR images because of volume-averaging and motion artifacts (Figs 2 and 3).
It has been shown that the number of lesions in tuberous sclerosis and the risk of retardation are positively related.9 Early manifestation of refractory seizures may necessitate lesion visualization for surgical resection (Fig 4).10 Pinto Gama et al4 reported that MT T1 was superior to other MR imaging sequences in detecting lesions of tuberous sclerosis. Girard et al8 reported that some lesions of tuberous sclerosis were only seen on the MT T1 sequence.
FCD can be very subtle and is more likely to be detected radiologically when it is evident on >1 imaging sequence and/or its signal profile relative to surrounding tissue is enhanced (Figs 5⇑–7).
As a limitation to the use of T1 with MT, all the cases presented here were imaged at 1.5T, and in this context, the addition of the MT to the T1 sequence appears to be beneficial for children with seizures.
Conclusions
We believe that MT T1 should be included in MR imaging protocols for children with epilepsy and/or the possibility of tuberous sclerosis to increase the chance of lesion detection and more reliable assessment of disease extent.
References
- Received May 7, 2012.
- Accepted after revision June 25, 2012.
- © 2013 by American Journal of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MR Imaging Detection of CNS Lesions in Tuberous Sclerosis Complex: The Usefulness of T1WI with Chemical Shift Selective Images
- Enhanced MR Conspicuity of Type IIb Focal Cortical Dysplasia by T1WI With CHESS: Two Case Reports
- Radiologic and Pathologic Features of the Transmantle Sign in Focal Cortical Dysplasia: The T1 Signal Is Useful for Differentiating Subtypes