Article Text

Abstract
BACKGROUND Cognitive-MRI correlations have often been studied in disorders in which there are multiple cognitive deficits and widespread cortical atrophy, such as Alzheimer's dementia. In such circumstances, the interpretation of any single cognitive-structural correlation is equivocal. Only by measuring differing cognitive functions and a wide range of brain structures in patients with a varying distribution of lesions or atrophy can specific brain-cognitive relations be determined in neurological disorder.
METHOD In the present study, a clear set of anatomical criteria and detailed MRI segmentation procedures were applied to measure whole brain, and left and right frontal, temporal lobe, anterolateral and medial temporal volumes, as well as thalamic cross sectional areas in 40 patients with organic amnesia (from various diseases) and 10 healthy controls.
RESULTS Within the total patient group, anterograde memory measures correlated significantly with medial temporal, hippocampal, and thalamic measurements. A spatial memory measure correlated significantly with hippocampal volume, and temporal context memory with frontal volume. After a factor analysis of the cognitive measures, the association between anterograde memory and hippocampal volume was corroborated. Forgetting rates and subjective memory evaluations did not show any significant MR correlations and, of executive tests employed, only card sorting categories correlated significantly with frontal volume.
CONCLUSION Loss of volume in key brain structures (for example, hippocampus, thalamus) is detectable on quantitative MRI, and this loss of volume correlates significantly with impaired performance on measures of anterograde memory function. Correlations with hippocampal volume did not indicate a specific role in either recall or verbal memory, as opposed to recognition or visual memory.
- magnetic resonance imaging
- volumetrics
- amnesia
- memory
- executive function
Statistics from Altmetric.com
Previous studies have reported significant correlations in patients with Alzheimer's disease and epileptic and aging subjects between hippocampal volume and measures of anterograde memory. These memory measures have included the Wechsler memory quotient,1WMS-R visual reproduction and two verbal memory measures,2a dementia rating scale measure of memory,3 and delayed verbal recall tasks,4-7 recognition memory,8and spatial memory.9 Kohler et al 6 also obtained a significant correlation between parahippocampal volume and a delayed visual recall task, and Jernigan and Ostergaard10 found a correlation between a mesial temporal measure and both recognition memory and word priming. However, the interpretation of all these studies is greatly limited by the restricted number of measurements that were made. If the brain is generally atrophied and there is widespread cognitive impairment, as in Alzheimer's dementia, there are likely to be many statistically significant correlations between measures of any atrophied structure and tasks demonstrating impaired cognitive performance. Only by measuring differing cognitive functions, as well as a wide range of brain structures, preferably in patients with focal lesions in various sites, can specific relations between cognitive performance and structural brain volumes be demonstrated.
In our accompanying paper,11 structural brain volumes from MRI were analysed for (1) repeatability of measurement, and (2) comparisons across certain patient groups— namely, patients with Korsakoff's syndrome, herpes encephalitis, or focal frontal lesions. In the present paper, we report investigations on the relation between MR volume measurements and performance on specific cognitive tasks. More specifically, we examined correlations between regional brain volumes and measures of anterograde memory, context memory, and executive function in 40 patients with memory disorder. We hypothesised that:
(1) Anterograde memory measures—recall and recognition—would correlate with measures of medial temporal and thalamic volume.
(2) Executive test performance would correlate with measures of frontal volume.
(3) Context memory performance would show a differential pattern of association—we predicted that spatial memory would correlate with hippocampal volume,12 whereas temporal context memory might correlate with measures of either frontal,13thalamic,14 15 or medial temporal14 volume.
Methods
MRI ACQUISITION AND ANALYSIS
Patients were scanned on a Siemens Magnetom SP 63 1.5 Tesla scanner or on a General Electric 1.5 Tesla Signa scanner. Quantitative analyses were performed on T1 weighted volume acquisitions with voxel sizes of 2.34×0.98×0.98 mm3 (Magnetom) and 1.20×0.93×0.93 mm3 (Signa). There were no significant differences between the findings from either scanner.11 An interactive computer analysis package16 was employed, making use of a multislice two dimensional hierarchical segmentation program, a two dimensional polyline tool for drawing a sequence of connected straight lines, and a three dimensional plane cutting tool.16 Measurements were made of intracranial and whole brain volume as well as left and right frontal, temporal lobe, anterolateral temporal, medial temporal, hippocampal, and parahippocampal volume. Thalamic area was measured on a proton density slice, and a “thalamic index” was this area expressed as a ratio of third ventricular volume. Further details of the methods employed, including the definitions used for boundaries of anatomical structures, are given in an accompanying paper.11 Figures 1 and 2illustrate frontal lobe and temporal lobe segmentations respectively.

Coronal, sagittal, and axial T2* segmentations of the frontal lobe in a healthy control subject and (lower right) a three dimensional projection (surface rendered) of the lateral surface of the frontal lobe.
{kind=link}
{kind=link}
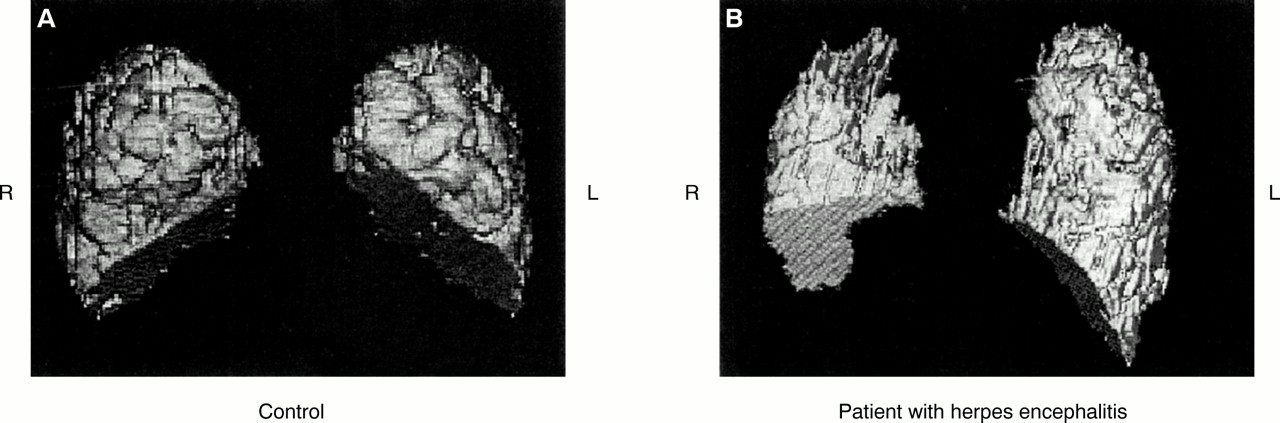
Three dimensional projections of the inferior surfaces of the left and right temporal lobes from (A) a control subject and (B) a patient with herpes encephalitis indicating right anterior-medial loss of volume in the patient.
COGNITIVE TASKS
Background intelligence measures
The national adult reading test revised (NART-R)17was used to estimate premorbid IQ, and the Wechsler adult intelligence scale-revised (WAIS-R) was used as a measure of current intelligence.18
Anterograde memory tests
A general memory index (or quotient) (GMQ) and delayed recall index (quotient) (DMQ) were obtained from the revised Wechsler memory scale (WMS-R).19
In a word recall test subjects were presented with a 16 word list, which they were required to recall after a “filled” interval of 30 seconds.20 After completion of this free recall task, subjects were given a forced choice word recognition test for the same words.20
In a picture recognition test, 32 line drawings were presented to subjects (in two sets of 16 each, presented 45 minutes apart); and a yes-no recognition test was administered 10 minutes after presentation of the second set.21
Verbal and visual Brown-Peterson tests involved the presentation of three words or a sequence of three Corsi blocks, respectively and, after a filled delay, recall was tested at 5 or 15 seconds.22
Forgetting tests22 involved measurements of forgetting rates on picture, word, and design recognition memory tasks between 1 minute, 15 (or 10) minutes, and 30 (or 20) minutes after performance across patient groups had been matched as closely as possible with the controls' scores at the initial delay interval. This was done by “titrating” the exposure time of stimuli.22 A picture recall task was also employed with delays of 20 seconds, 10 minutes, and 20 minutes.22
A subjective memory questionnaire23 asked subjects to evaluate their own memories on a standard rating scale.
Temporal and spatial context memory tests
On testing during the picture recognition test (Kopelmanet al 21 and above), subjects were also asked if they had seen each line drawing in the first series of pictures (presented 55 minutes earlier) or the second (10 minutes earlier). From items correctly recognised as having been seen before, the proportion which were also correctly attributed to the correct series was calculated (temporal context score).21 The line drawings had been located at the top or the bottom of a flash card, and at recognition testing, subjects were also required to identify which position (top or bottom) they had been in, the proportion correct constituting a spatial context score.21
Frontal/executive tests
FAS verbal fluency,24 card sorting categories and percentage perseverative errors,25 and cognitive estimates,26 were employed as measures of executive function.27
SUBJECT GROUPS
Forty patients with severe memory disorder were studied. These patients had previously been included in a series of cognitive studies.20-23 Patients had been selected for having predominantly focal lesions producing memory impairment on clinical, CT, and (where relevant) EEG criteria.
There were 15 patients who, on clinical criteria, were thought to have pathology in the diencephalon. These included 13 patients who had an alcoholic Korsakoff's syndrome, of whom 12 had either a documented history or residual signs of a Wernicke episode preceding their amnesia. These comprised 11 patients from the accompanying study11 and a further two patients with Korsakoff's syndrome who (unlike the other 11) also showed some anterior temporal lobe atrophy on naked eye inspection of their MRI scans. In addition, we included two patients who manifested an amnesic syndrome after surgical excision and irradiation of a pituitary adenoma.28 Plotting the radiotherapy planning fields against these patients' MR scans indicated that the structures affected by>90% of the irradiation included the anterior thalamus, the mammillary bodies, the mammillothalamic tract, and fornix, and these structures may also have been affected by ischaemia during surgery.28
A “temporal lobe” group (n=14) of patients included nine patients with probable or definite (antibody confirmed) herpes encephalitis, included in our parallel study.11 They also included four patients with hypoxic brain damage. Relative to healthy controls, these four patients showed significant atrophy in right hippocampal (t=2.65, p<0.025) and total hippocampal (t=2.17, p=0.05) volume. One further patient had a prolonged history of complex partial seizures with bilateral temporal lobe foci evident on EEG with CT/MRI evidence of mesial temporal lobe sclerosis.
In a frontal group (n=11), there were six patients with focal frontal lesions (two bilateral; three right unilateral; one left unilateral), also included in the parallel study.11 There were also five patients who had had a bilateral frontal tractotomy, using yttrium rods. Two weeks after treatment, these patients had neuropsychological testing and an MR scan, because it has been shown29 that their cognitive deficits can be attributed to their frontal lesions at this point, and not to any underlying affective disorder or medication.
Table 1 shows the mean cognitive scores of a healthy control group (n=10)11 and the total patient group (n=40). The patient group was significantly impaired on memory measures (p<0.0001) as well as on three out of four executive tests. There were no significant differences across the individual patient groups on NART-R, full scale IQ, GMQ, IQ-DMQ, FAS verbal fluency, card sorting categories, percentage perseverations, or cognitive estimates.
Background neuropsychological test scores
Results
Correlations are presented from the total patient group (n=40)—that is, excluding the controls. Correlations were performed both before and after correcting for intracranial volume using the formula of Jack et al.30 As discussed elsewhere,11 we found that this formula was of uncertain legitimacy in correcting smaller brain structures. Consequently, we present the correlations from the actual, obtained brain readings with comments on the effect of correction.
Table 2 shows the pattern of correlations between the measures of anterograde memory performance and volumes of those brain structures expected to correlate with memory performance. There were significant correlations between the memory indexes or quotients (GMQ and DMQ) and all these MR measures. In addition, there were further significant correlations between the other (recall and recognition, verbal and visual) memory tasks and various medial temporal, hippocampal, or thalamic measures. In general, the correlations tended to be strongest and most consistent with total hippocampal volume. Correlations with total parahippocampal volume were in the same direction as hippocampal volume and were significant for GMQ (r=0.55, p<0.05) and picture recognition (r=0.50, p<0.05). Correcting for intracranial volume eliminated the significant correlations with whole brain volume (rcorrected=0.18 (GMQ), 0.15 (DMQ), NS), but had negligible or no effect on all the other correlations in table 2.
Anterograde memory tasks: correlations with MR measures
Although our patient subgroups were relatively small, there were some significant correlations in our lesion subgroups in the expected direction with GMQ/DMQ: in the diencephalic patients (n=15) between DMQ and thalamic area (r=0.58, p<0.05) and thalamic index (r=0.62, p<0.05); in the patients with temporal lobe lesions (n=14) between GMQ and total temporal lobe volume (r=0.63, p<0.05); and in the patients with frontal lobe lesions (n=11) between GMQ and total frontal lobe volume (r=0.73, p<0.02).
By contrast, there were no significant correlations in the total patient group between regional MR volumes and any of our measures of forgetting rates (differences between scores at the initial and final delay) or between MR volumes and our measure of subjective memory evaluations.
Table 3 shows that our temporal context memory measure correlated significantly with whole brain, total frontal, left frontal, and right frontal volume, but it did not correlate significantly with the temporal lobe or thalamic measures. By contrast, the spatial context memory measure correlated significantly with total medial temporal and with total hippocampal volume (and also with total parahippocampal volume: r=0.63, p<0.02), but not with the other measures.
Temporal and spatial context memory tasks: correlations with MR measures
Among the executive tasks, card sorting categories correlated significantly with the total frontal (r=0.39, p<0.05), left frontal (r=0.37, p<0.05), right frontal (r=0.39, p<0.05), and whole brain (r=0.42, p<0.01) volume, but there were no other significant correlations between the other executive tasks and the structural measures.
These correlations were uncorrected for multiple comparisons because the investigation was hypothesis driven. Consequently, it was the pattern of correlations in which we were particularly interested. Moreover, strict Bonferroni corrections are likely to be overconservative particularly where measures are not independent of one another (for example, whole brain, temporal lobe, medial temporal, and hippocampal volumes). However, to exclude the possibility that the significant correlations reported in tables 2 and 3 had arisen by chance, a factor analysis using principal components31 32was carried out on the test scores from those two tables. Table 4 shows that three main factors emerged from this, together with their respective factor loadings. Factor 1, accounting for 49.6% of total variance, seemed to be a general memory factor. Factor 2, accounting for a further 13.7% of total variance, seemed to be a working memory27 or short term forgetting22 factor. Factor 3, accounting for 11.9% of total variance, seemed to be related to verbal recognition memory.
Table 5 shows the intercorrelations between factor 1 (general memory) and the principal brain regions measured on MRI. There were significant correlations with total lateral temporal, total medial temporal, total thalamic, and total hippocampal volumes, but not with total frontal volume. Most importantly, the correlation between factor 1 (memory) and total hippocampal volume was r=0.70 (p=0.0016). This correlation was unchanged after hippocampal volume had been corrected for intracranial volume, and it confirms that the significant correlations reported above between individual memory tests and hippocampal volume are most unlikely to have arisen by chance. However, none of the correlations between factors 2 or 3 and regional brain volumes attained statistical significance.
Correlations between factor 1 (general memory) and main brain regions measured
In summary, there were significant correlations between anterograde memory test scores and structural MR measures in critical brain regions. There was also a double dissociation between the temporal context memory score (associated with frontal volume) and the spatial context score (which correlated significantly with hippocampal volume). Factor analysis demonstrated a general memory factor, which showed a highly significant (p<0.002) correlation with hippocampal volume. However, of our executive tests, only card sorting categories correlated significantly with frontal volume. Forgetting rates and subjective memory evaluations did not show any significant MR correlations.
Discussion
Statistically significant correlations were obtained between measures of anterograde memory and specific brain structures. These correlations emerged most strongly for the general and delayed memory indexes (GMQ and DMQ). They were most striking and consistent for the hippocampal measurements, but they were also present across our thalamic measurements.
These significant correlations are most unlikely to be chance findings. Firstly, while various recall and recognition measures of anterograde memory showed a pattern of significant correlations with medial temporal and thalamic measurements, as predicted above, other variables (such as forgetting rates and subjective memory evaluations) did not show any significant correlations with the MR measurements. Secondly, the diencephalic, temporal lobe, and frontal lobe subgroups of patients showed the expected pattern of correlations between GMQ/DMQ and thalamic, temporal lobe, and frontal lobe measures, respectively. Thirdly, there was a double dissociation between temporal context memory and spatial context memory, such that the temporal context measure correlated significantly with frontal volume but not with hippocampal volume, whereas spatial context memory correlated significantly with hippocampal but not frontal volume. This result is consistent with many (although not all) findings from previous lesion studies.12 21 33-35 Finally, a factor analysis of the anterograde and context memory measures disclosed a general memory factor which showed a highly significant (p=0.0016) correlation with hippocampal volume.
By contrast, our executive tasks did not correlate significantly with frontal volume with the exception of card sorting categories. However, parallel fluorodeoxyglucose (FDG) PET studies in these same patients have shown significant correlations between executive test scores and measures of frontal brain metabolism.36 There are probably two main explanations for this apparent discrepancy: (1) volume measures of particular regions within the frontal lobes may be required to show correlation with performance on executive tests, and (2) other studies show that PET is particularly sensitive to alterations in frontal lobe function.37 38
Aggleton and Saunders39 have described three parallel projections between medial temporal structures and the thalamus. Hippocampal projections, originating in the subiculum, travel through the fornix to the anterior thalamic nuclei and (via the mammillothalamic tract) to the mammillary bodies. Secondly, there is a dense projection from the entorrhinal cortex to the lateral dorsal nucleus of the thalamus, and lighter projections to the anterior and medial dorsal nuclei of the thalamus. Thirdly, there is a projection from the perirrhinal cortex to the medial dorsal nuclei of the thalamus, but not to the lateral dorsal nucleus. In a series of papers, Reed et al 36 40-42 have reported FDG-PET findings consistent with such interconnections via the fornix and retrosplenium, and others have also reported related findings.43-45 It seems that medial temporal structures and the thalami both make important contributions to memory formation, and are tightly interconnected, but they are differentially damaged by diseases such as Korsakoff's syndrome or herpes encephalitis. The specific role and importance of the hippocampi in memory acquisition remains controversial,46 47 some authors arguing that they are critical only in recall (as opposed to recognition) memory,48 or in the formation of complex associations,47 49 or in the retention of verbal (rather than visual) material.6 The present findings confirm that hippocampal loss of volume does indeed have critical effects on memory formation. However, there was no evidence that hippocampal atrophy had specific effects on recall rather than recognition memory or on verbal rather than visual material.
In summary, we have obtained a clear pattern of correlations between structural brain measurements and cognitive tasks, showing that hippocampal and thalamic measurements correlated significantly with anterograde memory measures (recall and recognition), and that temporal context memory correlated significantly with frontal volume whereas spatial context memory correlated with hippocampal volume.
Acknowledgments
This research was funded by a Wellcome Trust project grant to MDK and BK, and by European Union grant 950845 (Biomorph) to AC and colleagues.