Article Text

Abstract
Objective: It has been proposed that cerebral blood flow (CBF) response to acetazolamide may be reduced according to the degree of autoregulatory vasodilation in regions with normal oxygen extraction fraction (OEF), whereas the CBF response may be absent in regions with increased OEF where vasodilation may be maximal in response to reduced perfusion pressure. The objective of this study was to test this hypothesis.
Methods: Positron emission tomography (PET) was used to study 30 symptomatic patients with carotid artery steno-occlusive lesions. CBF at baseline and 10 minutes after an intravenous injection of 1 g acetazolamide was measured. The correlation between the change in CBF during acetazolamide administration and the baseline value of OEF in the affected hemisphere was examined.
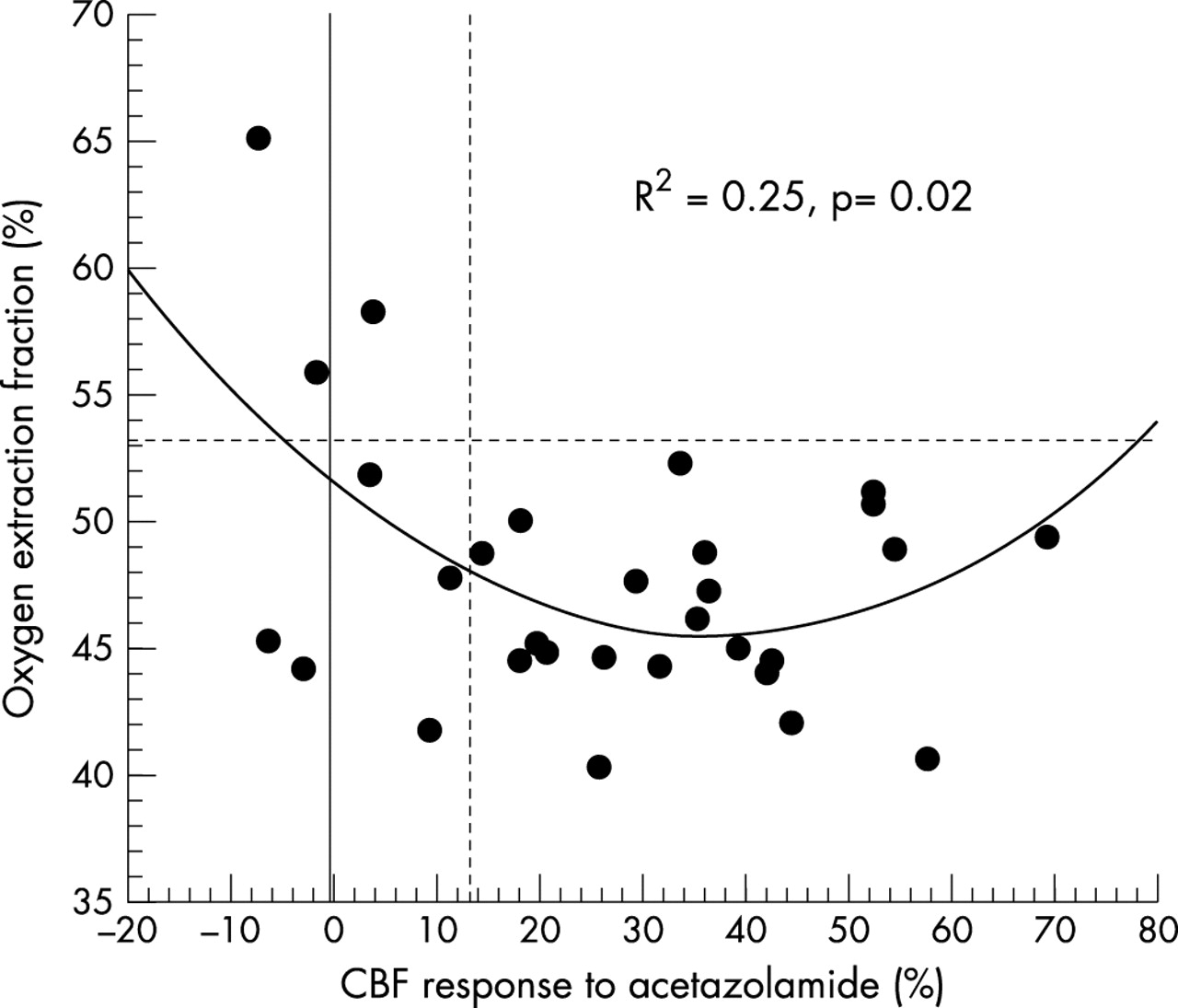
Results: The baseline OEF value was inversely and non-linearly correlated with the percentage change in CBF during acetazolamide administration (R2 = 0.25, p = 0.02). There was an upward trend of OEF with diminishing acetazolamide response below a critical level around zero response. Acetazolamide response less than 6.65% over baseline (sensitivity 100%, specificity 89%, positive predictive value 50%, negative predictive value 100%) was established as most helpful in predicting abnormally high OEF.
Conclusions: The inverse, non-linear relationship between OEF and CBF response to acetazolamide suggests that these two measurements may not identify haemodynamic impairment in the same patients.
- cerebral blood flow
- oxygen extraction fraction
- carotid artery disease
- positron emission tomography
- acetazolamide
- OEF, oxygen extraction fraction
- CBF, cerebral blood flow
- PET, positron emission tomography
- EC-IC, extracranial to intracranial
- CT, computerised tomography
- ICA, internal carotid artery
- MCA, middle cerebral artery
- MR(I), magnetic resonance (imaging)
- TIA, transient ischaemic attack
- CBV, cerebral blood volume
- ROC, receiver operative characteristic
- ROI, region of interest
- CMRO2, cerebral metabolic rate for oxygen
Statistics from Altmetric.com
- cerebral blood flow
- oxygen extraction fraction
- carotid artery disease
- positron emission tomography
- acetazolamide
- OEF, oxygen extraction fraction
- CBF, cerebral blood flow
- PET, positron emission tomography
- EC-IC, extracranial to intracranial
- CT, computerised tomography
- ICA, internal carotid artery
- MCA, middle cerebral artery
- MR(I), magnetic resonance (imaging)
- TIA, transient ischaemic attack
- CBV, cerebral blood volume
- ROC, receiver operative characteristic
- ROI, region of interest
- CMRO2, cerebral metabolic rate for oxygen
In patients with major cerebral arterial occlusive disease, a marginally adequate blood supply relative to metabolic demand (misery perfusion)1 may increase the risk of cerebral ischaemia,2 which suggests that identification and optimal treatment of patients with misery perfusion might help to prevent stroke. Patients with misery perfusion can be identified by increased oxygen extraction fraction (OEF), which is directly measured using positron emission tomography (PET). Recent studies have shown that increased OEF is a powerful and independent predictor of subsequent stroke in patients with symptomatic major cerebral arterial occlusive disease,3–5 and that extracranial to intracranial (EC-IC) bypass can improve cerebral blood flow (CBF) in patients with increased OEF. Thus, the need for a randomised clinical trial of EC-IC bypass for patients with major cerebral arterial occlusive disease and increased OEF has been identified,67 and such a study using PET has been initiated in the US.8
In clinical practice, the CBF response to vasodilatory stimuli, which may reflect the degree of cerebral autoregulatory vasodilation in response to reduced perfusion pressure in patients with major cerebral arterial occlusive disease, can be used as an alternative parameter for predicting stroke risk.29 Several studies using stable xenon enhanced computerised tomography (CT), or xenon133-SPECT, or transcranial Doppler, have revealed that a subgroup of patients with reduced vasodilatory response to acetazolamide or CO2 have an increased risk of stroke.710–13 However, the risk of stroke reported in the subgroup of patients with a reduced vasodilatory response was lower than that in patients with increased OEF, and some studies showed no association between a reduced vasodilatory response and increased risk of stroke.1415 It is uncertain whether the vasodilatory response and OEF are comparable as tests for haemodynamic impairment, because the relationship between OEF and vasodilatory response is unclear.
It has been proposed that a reduction of the perfusion pressure caused by severe atherosclerotic disease of the cerebral arteries may result in a series of compensatory responses.2 Mild reduction of cerebral perfusion pressure causes autoregulatory cerebral vasodilation, which acts to keep CBF constant. At this stage, where OEF is normal, the CBF response to vasodilatory stimuli may be reduced according to the degree of vasodilation. With further reduction in perfusion pressure, the autoregulatory capacity is exceeded and CBF falls passively as a function of pressure. Then the OEF increases, and the CBF response to vasodilatory stimuli may be absent because vasodilatory capacity may be exhausted.29 If this theory is correct, OEF is inversely and non-linearly correlated with CBF response to vasodilatory stimuli. However, no previous study has supported this hypothesis. In contrast, several previous studies have shown an inverse, linear relationship between OEF and CBF response to vasodilatory stimuli.
In previous studies, different techniques were used to measure OEF and vasodilatory response (PET and SPECT /Xe-CT, respectively), which might result in a false linear relationship. The objective of this study was to determine whether OEF is inversely and non-linearly correlated with CBF response to acetazolamide in patients with symptomatic carotid artery steno-occlusive lesions, by measuring both OEF and vasodilatory response with PET.
METHODS
Participants
We studied 30 consecutive patients, mean age 64(6) years, including 26 men and four women, with symptomatic atherothrombotic occlusion or stenosis (>70% diameter reduction) of the internal carotid artery (ICA). All subjects were prospectively selected from patients with occlusion or stenosis of the ICA or middle cerebral artery (MCA), who had been referred to our PET unit for evaluating the haemodynamic effect of major cerebral arterial occlusive disease from our hospital and regional hospitals between October 2000 and February 2002. Inclusion criteria were:
-
occlusion or stenosis (>70% diameter reduction) of the ICA documented by conventional or magnetic resonance (MR) angiography
-
transient ischaemic attacks (TIAs) or minor stroke with mild disability in the arterial distribution distal to the lesion.
Exclusion criteria were:
-
latest ischaemic event within the past month
-
heart failure
-
follow up PET after EC-IC bypass.
Written informed consent was obtained from each subject under the guidance of the Ethics Committee of the Shiga Medical Center.
Four subjects had had a transient ischemic attack (TIA), and 26 had had a minor stroke. In all participants, magnetic resonance imaging (MRI) disclosed only minor abnormalities in the MCA territory or watershed areas of the hemisphere with major arterial disease. In three of the patients with TIA, the MRI was normal. Among 27 patients with infarcts, five had unilateral cortico-subcortical watershed infarcts, 17 had unilateral subcortical infarcts, and five had bilateral subcortical infarcts. None had bilateral lacunar infarctions with extensive white matter lesions. Vascular lesions were documented by using conventional angiography in 25 cases and MR angiography in five cases. Conventional or MR angiography revealed unilateral ICA occlusion in eight cases, unilateral extracranial ICA stenosis in 15 cases, bilateral ICA occlusion in one case, ICA occlusion with contralateral extracranial ICA stenosis in five cases, and bilateral extracranial ICA stenosis in one case. In six persons with bilateral disease, only one side of the vascular lesions was symptomatic. No significant disease of the posterior cerebral artery was seen in any participant. The vertebrobasilar system was angiographically normal in all but two individuals. The characteristics of participants are summarised in table 1. All patients were treated with antiplatelet therapy (aspirin and/or ticlopidine HCl), but the use of additional potentially vasoactive medication such as antihypertensives or statins varied. It is unclear whether and how these medications affect acetazolamide reactivity.
Characteristics of participants
PET measurements
All subjects underwent PET scans with a whole body, Advance (General Electric Medical System, Milwaukee, Wis, USA) PET scanner, which permits simultaneous acquisition of 35 image slices with interslice spacing of 4.25 mm.1617 Performance tests showed the intrinsic resolution of the scanner to be 4.6 to 5.7 mm in the transaxial direction and 4.0 to 5.3 mm in the axial direction. As part of the scanning procedure but before the tracer administration, 68Ge/68Ga transmission scanning was carried out for 10 minutes for attenuation correction. For reconstruction of the PET data, images were blurred to 6.0 mm full width, half maximum in the transaxial direction using a Hanning filter. Functional images were reconstructed as 128 × 128 pixels, with each pixel representing an area of 2.0 mm × 2.0 mm.
Firstly, a baseline H215O study was performed. After intravenous bolus injection of 555 MBq of H215O into the right antecubital vein, a dynamic PET scan lasting three minutes was started at the time of tracer administration with frame durations of 5 seconds × 12, 10 seconds × 6, and 20 seconds × 3. Arterial blood was continuously withdrawn from a catheter in the radial artery using a minipump AC-2120 (Atto, Tokyo, Japan), and the concentration of radioactivity was monitored with a coincidental Pico-Count flowthrough radioactivity detector (Bioscan, Washington, DC, USA),18 and used as an input function for data analysis. After the baseline H215O study, a series of 15O gas studies was performed. C15O2 and 15O2 were inhaled continuously through a mask.17 The scan time was five minutes, and arterial blood was sampled manually from the brachial artery three times during each scan. The radioactivity of the radiotracer in whole blood and plasma was measured with a well counter. Inhalation of C15O with three minute scanning was used to measure cerebral blood volume (CBV). Arterial samples were obtained manually twice during the scanning, and the radioactivity of the radiotracer in whole blood was measured. After the 15O gas study, 1 g acetazolamide was administered intravenously.19 Ten minutes after the administration, a second H215O study was carried out. We performed the H215O study in the three dimensional acquisition mode, and the 15O gas study in the two dimensional mode.
In the 15O gas study, we calculated CBF, cerebral metabolic rate for oxygen (CMRO2), and OEF based on the steady state method.20 CMRO2 and OEF were corrected by the CBV.21 In the H215O study, CBF was calculated using the autoradiographic method with a partition coefficient of 0.9 ml/g.2223
Data analysis
We analysed 10 tomographic planes from 46.25 to 84.5 mm above and parallel to the orbitomeatal line, which corresponded to the levels from the basal ganglia and thalamus to the centrum semiovale. The software for image analysis was programmed by a member of our research team. The region of interest (ROI) was placed on the baseline H215O-CBF images. Each image was examined by placing a total of 10 to 12 circular ROIs, 16 mm in diameter, compactly over the grey matter of the outer cortex in each hemisphere. According to the atlas prepared by Kretschmann and Weinrich,24 the ROIs in all 10 images were included in the distribution of the anterior cerebral artery, MCA, and posterior cerebral artery, as well as the watershed areas between the anterior cerebral artery and MCA (anterior watershed) and between the MCA and posterior cerebral artery (posterior watershed). In five patients with infarction in the cerebral cortex, the ROIs that overlapped a well demarcated area of decreased CMRO2, corresponding to low intensity areas on T1 weighted MR images, were excluded from the analysis. The same ROIs were transferred to the other images. The mean hemispheric values in each hemisphere were calculated as the average of the values for the MCA, anterior watershed, ROI, and posterior watershed ROI, and each was weighted by region size.25
We calculated the percentage difference between the CBF value obtained after acetazolamide administration and the value at baseline (Δ%) as Δ% = [CBF value (acetazolamide) − CBF value (baseline)] / [CBF value (baseline)] × 100 (%). We assumed that the resulting value reflected the percentage change caused by acetazolamide administration. The mean (SD) value of the CBF response to acetazolamide in the 32 hemispheres of 16 healthy volunteers (eight men and eight women) aged 30 (10) years was 35.8 (11.4)%. The lower 95% limit defined in normal subjects was 12.3%.
Normal control values of the OEF were obtained from seven healthy volunteers (four men and three women) aged 47(7) years, who had normal routine neurological examinations and MRI scans. According to the OEF data, the 30 patients were divided into those with increased OEF and those with normal OEF. The mean OEF value in the 14 hemispheres of the normal subjects was 44.5 (3.8)%. Absolute hemispheric values beyond the upper 95% limit defined in normal subjects (above 52.9%) were considered abnormal. Previous studies have shown that increased OEF determined by this method is an independent predictor of stroke risk in patients with symptomatic major cerebral arterial occlusive disease.34
No subject showed a significant change in PaCO2 during PET scanning, and the changes in the physiological data during acetazolamide administration were small in all participants. Data analysis was performed by one investigator who was blinded to the clinical status of the participants.
Statistical analysis
The relationships between the changes of CBF induced by acetazolamide administration and the baseline values of OEF and CBV in the hemisphere ipsilateral to the symptomatic ICA lesion were analysed using linear or non-linear regression analysis. Sensitivity, specificity, positive predictive value, and negative predictive value were calculated for comparison of the quantitative acetazolamide test with the OEF method. Cohen’s kappa statistic was used as a chance corrected measure of agreement between the two methods. The receiver operative characteristic (ROC) curve analysis was used to select the best threshold for CBF response to predict increased OEF.
RESULTS
In the participants studied, the baseline OEF value was inversely and non-linearly correlated with the percentage change in CBF during acetazolamide administration (R2 = 0.25, p = 0.02); OEF = 51.5 − 0.332(Δ%) + 0.005(Δ%2). Although a vertical upward trend of OEF with diminishing acetazolamide response below a critical level around zero response suggested an exponential rather than a polynominal function, (fig 1), an exponential function did not significantly fit the data.
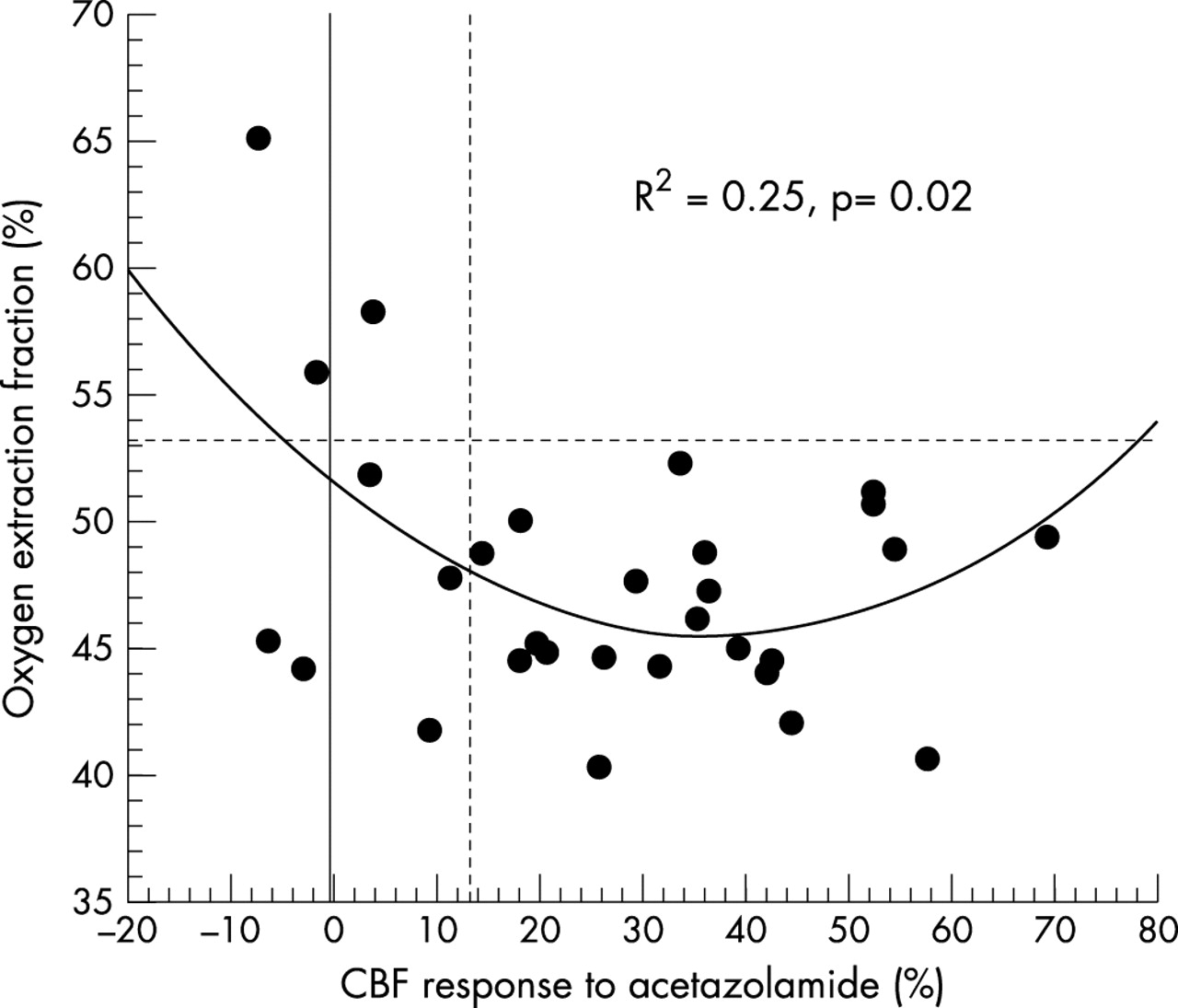
Scatterplot relating the degree of change in cerebral blood flow (CBF) in response to acetazolamide administration to the oxygen extraction fraction (OEF) baseline value in the cerebral cortex ipsilateral to the symptomatic carotid artery disease. The dashed lines show the lower (for CBF response to acetazolamide) or upper (for OEF) 95% limits for the controls.
The three hemispheres in which the OEF was high compared with the threshold value determined in the healthy controls also showed a decreased CBF response (less than 12.3%) after acetazolamide administration (sensitivity, 100%), and 22 of the 27 hemispheres with a normal OEF value showed a normal CBF response (specificity, 81%) (fig 1). The Cohen’s kappa analysis showed good agreement (kappa = 0.47).
The ROC curve analysis showed that the degree of agreement between these two methods was best when we adopted 6.65% as the threshold value of reduced CBF response (kappa = 0.62). The use of reduced CBF response to predict increased OEF showed a 100% sensitivity, 89% specificity, 50% positive predictive value, and 100% negative predictive value.
The CBF response to acetazolamide showed a significant negative linear relationship to the CBV value at baseline (R2 = 0.50, p<0.0001). The baseline OEF value was positively and non-linearly correlated with the CBV value at baseline (R2 = 0.22, p = 0.032), OEF = 87.7 − 23.6 (CBV) + 3.34 (CBV2), and the three hemispheres in which the OEF was high also showed high CBV (fig 2). An exponential function did not significantly fit the data. The CBF response to acetazolamide was not correlated with age (R2 = 0.001, p = 0.87).

{kind=link}
{kind=link}
Scatterplots relating the cerebral blood volume (CBV) baseline value to (A) the degree of the change in cerebral blood flow (CBF) in response to acetazolamide administration; or (B) the baseline value of OEF in the cerebral cortex ipsilateral to the symptomatic carotid artery disease. The dashed line shows the upper 95% limit of OEF for the controls.
DISCUSSION
This study showed that OEF was inversely and non-linearly correlated with CBF response to acetazolamide in patients with symptomatic carotid artery steno-occlusive lesions. There was a vertical upward trend of OEF with diminishing acetazolamide response below a critical level around zero response. An exponential function was expected to fit the data set, and was considered to be meaningful in terms of the resulting equation, but the fitting was not statistically significant. Alternatively, a polynominal function did significantly fit the data, probably because OEF varied in the normal range of acetazolamide response. The significant negative linear relationship between the CBF response to acetazolamide and CBV suggests that the CBF response to acetazolamide may be reduced according to the degree of autoregulatory vasodilation.26 On the other hand, OEF was positively and non-linearly correlated with CBV, which suggests that OEF may increase after the degree of autoregulatory vasodilation reaches a near maximal level. These relationships among autoregulatory vasodilation, reduced CBF response to acetazolamide, and increased OEF may cause the inverse, non-linear relationship between OEF and acetazolamide reactivity.
The relationship between OEF and acetazolamide reactivity shown in this study indicates that these two methods are not comparable for detecting patients with haemodynamic impairment. Acetazolamide reactivity less than 6.65% over baseline predicted abnormally high OEF with 100% sensitivity but only a 50% positive predictive value (kappa = 0.62). This relatively low positive predictive value may be unavoidable, because a reduced CBF response to acetazolamide does not necessarily accompany decreased CBF and thereby lead to increased OEF. The combination of decreased CBF and reduced vasodilatory capacity may improve accuracy in detecting patients with increased OEF.27 However, in symptomatic patients with carotid artery disease, focal ischaemic changes ranging from selective neuronal damage to infarction may decrease CMRO2 and CBV not only in the ischaemic region but also in distant regions through deafferentation.28 Such patients may show complex changes of CBF, CMRO2, OEF, and CBV that may be caused by both reduced perfusion pressure and ischaemic changes.2930 Increased CBV caused by reduced perfusion pressure may coexist with parallel decreases of CBF and CMRO2 caused by ischaemic changes in patients with infarction. Therefore, in regions with reduced CBF also, a reduced CBF response to acetazolamide does not necessarily accompany increased OEF. These factors are probably the major causes of the low positive predictive value observed here.
Several studies have investigated the relationship between OEF and CBF response to vasodilatory stimuli.72731 Our major interest in this study was the mean hemispheric value of OEF, which has been shown to be an independent predictor for subsequent ischaemic stroke.35 Few studies have analysed the relationship by using data consisting of one mean hemispheric value from each patient. One study, which used quantitative CBF measurement with xenon133 and CO2, showed that reduced CBF response to vasodilatory stimuli could be sensitive to increased OEF, because no subjects with increased OEF had a normal CBF response; but a threshold value that included all individuals with increased OEF also included many participants with normal OEF (low positive predictive value).31 These findings are comparable with the results in this study. To date, in most previous studies as well as the present study, the number of subjects has been small and there has possibly been some bias in the selection. In addition, the incidence of patients with increased OEF is in general low (less than 20%).23 Therefore, further studies including a larger number of participants will be required to determine whether the OEF method and vasodilatory response are comparable for detecting patients with haemodynamic impairment. However, the high sensitivity and low positive predictive value of a reduced CBF response to acetazolamide compared with increased OEF appears to be in accord with the finding of recent studies—that is, a subgroup of patients with severely decreased CBF response to acetazolamide have a high risk of developing a stroke that is lower than the risk in patients with increased OEF.101213
If the accuracy of its measurement of the vasodilatory response is similar to that of PET,32 the quantitative acetazolamide test, together with other methods to measure CBF, may be useful as an alternative to PET OEF methods for identifying patients who may benefit from EC-IC bypass surgery, when nil response is used as the criterion for reduced response. To test this hypothesis, a randomised clinical trial of EC-IC bypass for patients with decreased CBF and severely reduced CBF response to acetazolamide using SPECT is ongoing in Japan.
In conclusion, in subjects with symptomatic carotid artery steno-occlusive lesions, OEF was inversely and non-linearly correlated with CBF response to acetazolamide. There was an upward trend of OEF with diminishing acetazolamide response below a critical level around zero response. This relationship suggests that these two methods may not identify the same patients as having haemodynamic impairment.