Article Text

Abstract
OBJECTIVE The direct calculation of cerebral perfusion pressure (CPP) as the difference between mean arterial pressure and intracranial pressure (ICP) produces a number which does not always adequately describe conditions for brain perfusion. A non-invasive method of CPP measurement has previously been reported based on waveform analysis of blood flow velocity measured in the middle cerebral artery (MCA) by transcranial Doppler. This study describes the results of clinical tests of the prototype bilateral transcranial Doppler based apparatus for non-invasive CPP measurement (nCPP).
METHODS Twenty five consecutive, paralysed, sedated, and ventilated patients with head injury were studied. Intracranial pressure (ICP) and arterial blood pressure (ABP) were monitored continuously. The left and right MCAs were insonated daily (108 measurements) using a purpose built transcranial Doppler monitor (Neuro QTM, Deltex Ltd, Chichester, UK) with software capable of the non-invasive estimation of CPP. Time averaged values of mean and diastolic flow velocities (FVm, FVd) and ABP were calculated. nCPP was then computed as: ABP×FVd/FVm+14.
RESULTS The absolute difference between real CPP and nCPP (daily averages) was less than 10 mm Hg in 89% of measurements and less than 13 mm Hg in 92% of measurements. The 95% confidence range for predictors was no wider than ±12 mm Hg (n=25) for the CPP, varying from 70 to 95 mm Hg. The absolute value of side to side differences in nCPP was significantly greater (p<0.05) when CT based evidence of brain swelling was present and was also positively correlated (p<0.05) with mean ICP.
CONCLUSION The device is of potential benefit for intermittent or continuous monitoring of brain perfusion pressure in situations where the direct measurement is not available or its reliability is in question.
- cerebral perfusion pressure
- transcranial Doppler
- non-invasive monitoring
Statistics from Altmetric.com
The concept that the difference between arterial (ABP) and intracranial pressure (ICP) represents cerebral perfusion pressure (CPP)1 is well established in clinical practice. Identification of secondary brain insults2 and a clear dependence between average CPP and outcome after severe head injury, demonstrated in the 1970s and 1980s,3 have contributed to the formulation of CPP oriented therapy.4 In our centre CPP oriented management was rigorously introduced in 1995, with a critical threshold of CPP set by consensus at a target value of 70 mm Hg. CPP has ceased to be a significant predictor of outcome.5
This may provoke suspicions that the concept of CPP as a number (CPP=ABP−ICP) is not always adequate and assessment of cerebral perfusion, based on cerebral blood flow (CBF) or brain oxygenation, would be more appropriate. Unfortunately, existing methods for the measurement of CBF are not suitable for continuous bedside monitoring. Non-invasive technology for the measurement of brain oxygenation based on near infrared spectroscopy is still unreliable6 and direct measurements are extremely localised.
Transcranial Doppler ultrasonography offers non-quantitative measurements of CBF. Changes in global CBF can be monitored continuously and non-invasively using blood flow velocity,7 provided that the diameter of basal cerebral arteries does not change. Exploring this concept, many independent authors have emphasised that specific patterns of transcranial Doppler waveform follow the state of inadequate cerebral perfusion caused by a decrease in CPP.8-10 Although converting this specific distortion of blood flow velocity waveform to CPP is difficult,8 10 this step seems to be necessary as most therapeutically used protocols are still based on a value of CPP expressed as a number. A non-invasive method for the assessment of CPP using transcranial Doppler blood flow velocity waveform has been described previously.10 Using this methodology, the prototype bilateral transcranial Doppler machine with a built in algorithm to assess CPP using an externally measured value for ABP has been designed (Neuro Q TM Deltex Ltd, Chichester, UK). The prototype has been used in a prospective study to address questions about the accuracy of non-invasive CPP estimation, and the significance of side to side differences in non-invasive CPP.
Clinical material and methods
PATIENTS
With the approval of the local ethics committee non-invasive CPP was assessed daily using the prototype device based on transcranial Doppler ultrasonograph (Neuro-QTM) in 25 patients with closed traumatic brain injury. Only patients with diffuse cerebral injury or with focal lesions mild enough not to require a surgical procedure were studied. The patients were admitted to the Neuroscience Critical Care Unit in Addenbrooke's Hospital, Cambridge, United Kingdom, from June to December 1998.
There were 21 men and four women; the mean age was 36 (range 18 to 76).
All patients were sedated, paralysed, and ventilated to maintain adequate oxygenation and mild hypocapnia (30–35 mm Hg of arterial blood CO2 partial pressure). Intravenous fluids and inotropic support were used to maintain a target CPP above 70 mm Hg. The ICP was kept below 25 mm Hg by vigorous management, which was possible in all but one patient (who died).
The core temperature was kept in a normal range (35°C-37°C). Cooling measures were used only to avoid hyperthermia. Active hypothermia was not pursued. Brain CT was pragmatically analysed and graded using a simplified system based on the classification of Marshall et al.11
The following radiographic features were scored:
-
Disappearance of sulci
-
Effacement of ventricles
-
Reduction of the white-grey matter difference—that is, disappearance of the white-grey matter difference in more than 50% of the slices.
-
Basal cistern compression.
The sum of these factors produced a rudimentary swelling score from 0 to 4.
MONITORING
In all patients systemic and cerebrovascular circulation was monitored.
Cardiovascular dynamics were routinely assessed using an ABP line (radial or dorsalis pedis arteries), central venous and pulmonary artery pressure monitoring, ECG, and pulse oximetry.
A fibreoptic transducer (Camino, Camino Lab, San Diego, CA, USA) or Codman microsensor (Codman, Randolph, MA, USA) was inserted intraparenchymally into the right frontal region and fixed to the skull with a bolt to measure ICP.
The MCA blood flow velocity was measured daily, beginning on the day of admission and continuing until the ICP bolt was removed. Special care was taken to perform the recording during a stable period of ventilation and haemodynamics (for 30 minutes minimum; periods of recording were randomly distributed throughout the day). The MCAs were bilaterally insonated using two probes mounted on an adjustable frame (Neuro QTM- prototype, Deltex Ltd, Chichester, UK). The signal was detected from a depth varying from 4.5 to 6 cm. Data showing obvious artefacts (abrupt and sudden modification in the recording related to arterial line flushing, loosening of cables, electrical interference, etc) were excluded.
For final analysis, recordings obtained only from sedated, paralysed patients with closed head injury, with continuous ICP and ABP measurements, with good quality bilateral MCA flow velocity recordings were included.
DATA CAPTURE AND ANALYSIS
Analogue outputs from the pressure monitors and the Neuro QTM unit were connected to the analog to digital converter fitted into a laptop computer. Data were sampled (sampling frequency 50 Hz), digitised, and stored on the computer hard disk using software designed for waveform recording.10 Data calculated within Neuro QTM were downloaded to the laptop computer via an RS 232 serial interface.
Both the Neuro QTM and computer digital time series were processed and compared. Time averaged (mean) values of ICP, ABP, and CPP (ICPm, ABPm, CPPm respectively (CPPm=ABPm−ICPm)) were calculated using time integration of waveforms for 5 second intervals.
Time averaged mean, systolic, and diastolic values of flow velocity (FVm, FVs, and FVd respectively) were calculated after careful spectral filtration to reduce the influence of artefacts or noise and averaged within the same 5 second periods.
The non-invasive CPP (nCPP) calculation was based on a formula previously published10: nCPP=meanABP×FVd/meanFV+14 mm Hg
The measurements were performed separately using left and right MCA flow velocities; left−right nCPP was designated as dCPP. The arithmetic mean of left and right nCPPs was designated as nCPP.
STATISTICAL ANALYSIS
An observational x-y scatterplot was used to visualise association between all 1 minute averages of measured nCPP and CPP. A Bland-Altman12 plot was presented using averaged values of measured parameters over the whole recording period (n=108). Regression analysis (CPP versus nCPP) was performed for independent data samples (n=25) averaged for each patient, and the 95% confidence interval for predictors was measured. Left to right differences of CPP were analyzed using values of left and right nCPP averaged over all measurements performed in individual patients with analysis of variance (ANOVA) (F test or Kruskall-Wallis test).
Results
CPP AND nCPP
One minute averages (n=12 275), daily averages (n=108), and patient averages (n=25) were analysed. The distributions of the absolute difference between calculated and estimated CPP is given in the table.
Per cent proportion of non-invasive estimator of CPP fitting 5, 10, and 15 mm Hg error ranges compared with direct (invasive) CPP (n=12725 1 minute averages)
A 1 minute average scatterplot visualising association between CPP and nCPP is presented in fig 1 A. Distribution of the absolute difference CPP-nCPP is presented in fig 1 B; 81% of 1 minute averages of nCPP were different from direct CPP by less than 10 mm Hg.

(A) Scatterplot of all 1 minute averages of CPP (x axis) and nCPP (y axis) with x=y unity line and ±10 mm Hg range. (B) Cumulative histogram showing percentage of samples when the absolute difference between nCPP and CPP was less than a value on the x axis.
A Bland-Altman plot is presented in fig 2 for daily averages of CPP. Day by day averaging increased the percentage of the measurements with an absolute difference nCPP-CPP less than 10 mm Hg to 89%.

Bland-Altman plot of all 108 day by day measurements of CPP=ABP-ICP and nCPP. Bias was non-significantly different from zero. Thick horizontal line shows ±10 mm Hg distance from bias.
Although direct ICP was measured routinely in the right hemisphere, there were no obvious differences between error distribution on the left and right side (table).
Using the analysis of patient averaged data, correlation between averaged CPP and nCPP proved to be significant (R=0.61; n=25; p=0.003). The lines limiting the 95% confidence region for predictors were distant from the regression line by no more than ±12 mm Hg when CPP varied from 70 to 95 mm Hg.
SIDE TO SIDE DIFFERENCES IN nCPP
The mean absolute value of dCPP was 6 (SD 5.8) mm Hg. Daily observations showed that the absolute value of dCPP progressively increased with time after injury (ANOVA; p<0.012). Similarly, the absolute value of the difference between left and right mean flow velocity increased with time elapsed from trauma (ANOVA; p<0.006). The dCPP was significantly correlated with side to side difference in mean flow velocity (R=0.78; p<0.0001).
In patients showing midline shift on CT (n=4), the estimated dCPP was significantly greater than zero (mean 12 (SD 6) mm Hg; p<0.04, Kruskall-Wallis test, fig 3 A). The swelling score was significantly associated with an increase in absolute value of dCPP (p<0.05, fig 3B). Finally, an absolute value of dCPP was significantly correlated with a mean ICP (fig 3 C).
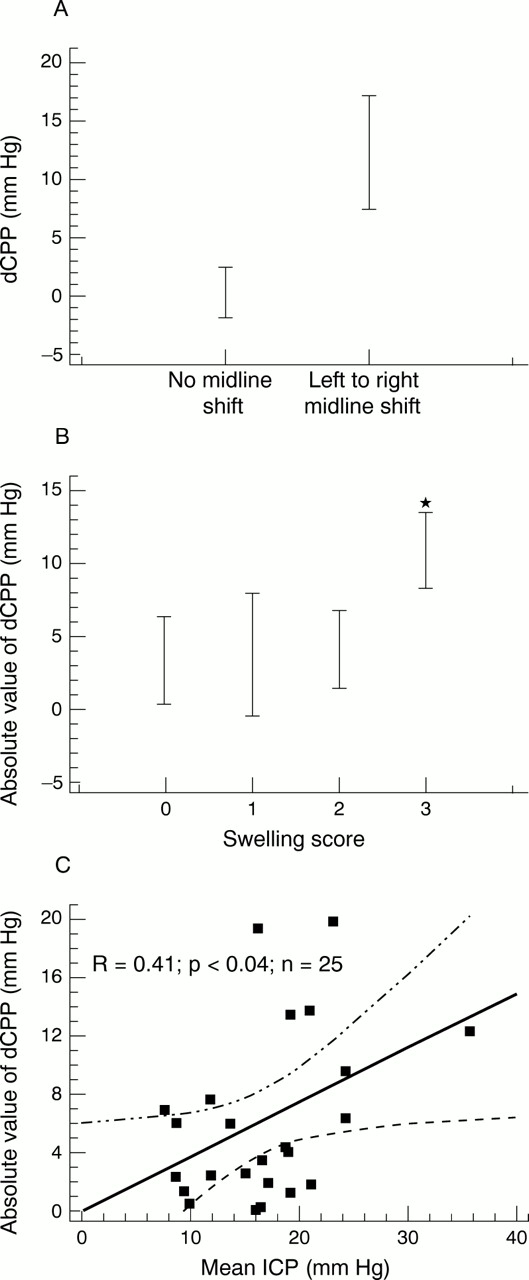
Statistical analysis of dCPP (dCPP= left side nCPP- right side nCPP; n=25 patients). (A) dCPP is significantly positive in patients with left to right midline shift (p<0.021; ANOVA; F test). (B) absolute value of dCPP is significantly increased in patients with the highest swelling score (p<0.026, ANOVA; F test). (C) absolute value of CPP increases when measured mean ICP increases (p<0.04, regression analysis).
OBSERVATIONS
An example of 11 consecutive daily recordings in a patient with head injury is presented in fig 4. In this patient the trends in CPP and nCPP were moderately correlated in time (R 2 =0.48). The greatest discrepancy between CPP and nCPP took place on day 4 (average CPP-nCPP=9 mm Hg), when the average ICP increased to above 40 mm Hg. This was followed by a significant and symmetric increase in blood flow velocity.
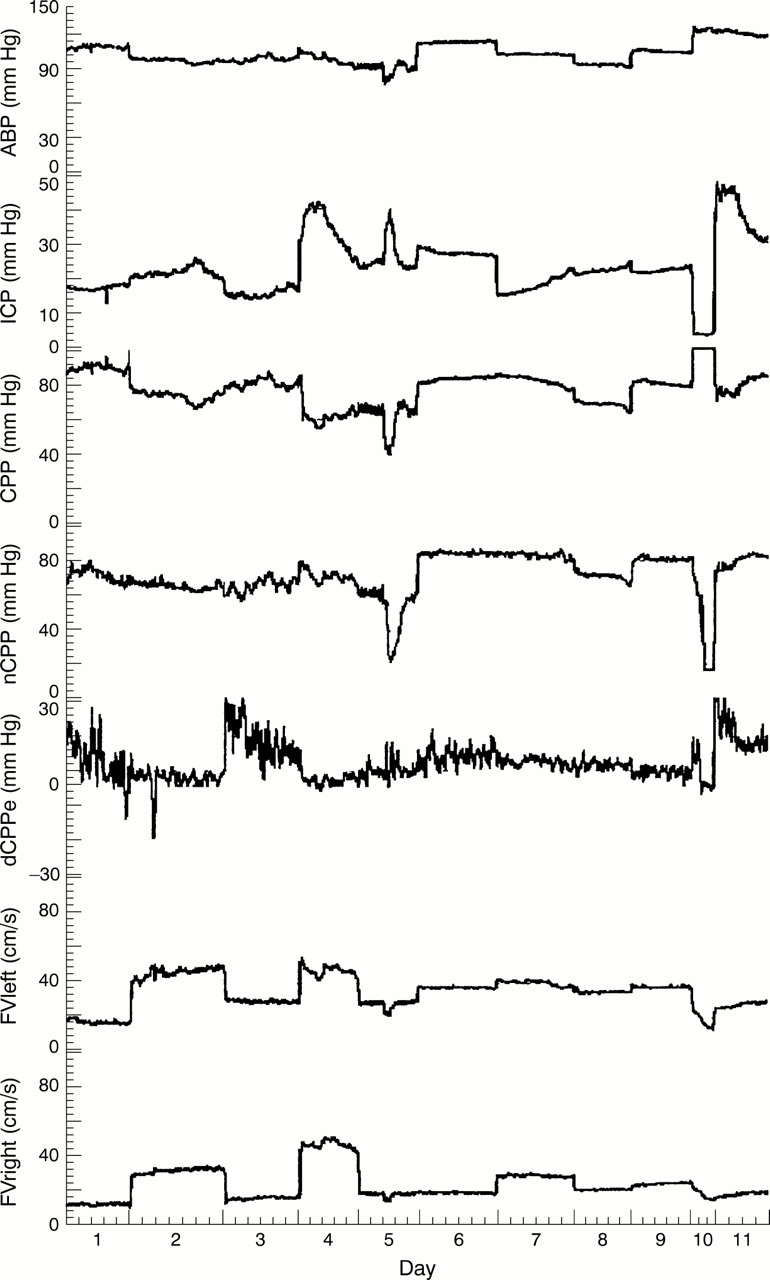
Daily recordings of mean ICP, arterial pressure (ABP), cerebral perfusion pressure (CPP=ABP-ICP), left and right mean flow velocity (FV left and FV right), non-invasive CPP (nCPP), and left to right difference in nCPP (dCPP) in a patient after head injury. Signals were recorded for at least 30 minutes each day.
A typical plateau wave was recorded on day 5, with a slight and symmetric drop in FV and good pattern of accordance between CPP and nCPP.
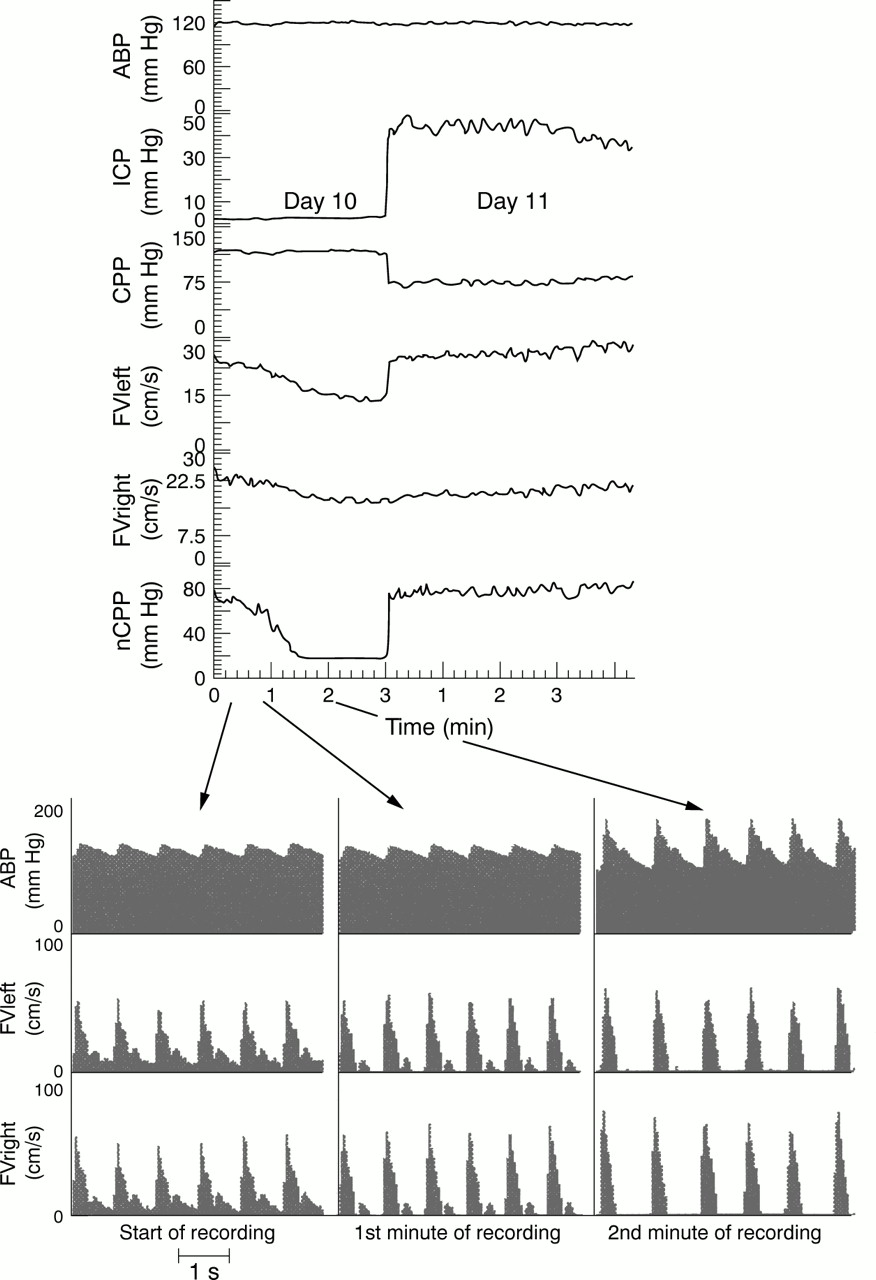
Recordings performed on days 10 and 11 illustrate the clinical significance of transcranial Doppler in the assessment of cerebrovascular haemodynamics (see details on fig 5). During the night between days 9 and 10, the ICP signal decreased significantly to a very low value with a poor pulsatility and CPP increased accordingly. This was caused by ICP transducer malfunction. On day 10 (fig 5) the CPP and nCPP were obviously different, due to faulty readings of the ICP. At this stage the mean FV decreased and nCPP dropped reaching an extremely low value (less than 20 mm Hg), consistent with a plateau wave.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Recording made on days 10 and 11 when the invasive ICP transducer was defective. CPP was obviously artefactual. nCPP demonstrated a deep decrease during the recording, which coincided with a characteristic change in flow velocity waveform (below) with normal (left graph-beginning of recording); diminishing (1st minute of recording) and absent diastolic blood flow (2nd minute of recording). On day 11 a new ICP sensor was inserted and the CPP was again close to nCPP.
The data illustrating changes in the FV pulsatility pattern are presented in fig 5. At the beginning of the recording the diastolic FV was normal. It then fell steeply towards 0 during the first 3 minutes of the recording. This pattern is characteristic of a plateau wave of ICP13 which has been detected using nCPP in an absence of direct CPP recording.
When, on day 11, a new ICP transducer had been inserted, the measured CPP was close to the nCPP recorded on the previous day at the baseline.
Discussion
In a broad sense, the CPP reflects the physiological conditions for blood flow. The perfusion pressure of any organ is defined as the arithmetic difference between the mean inflow and outflow pressures.
In the brain, the cerebral blood inflow pressure is considered to be close to the mean ABP. The cerebral blood outflow pressure is not far from the pressure in the bridging veins, which is near the mean ICP. Hence, the mean CPP can be estimated with the formula:
CPP=mean ABP−mean ICP
In clinical practice both variables ICP and ABP can be measured with limited accuracy. The case illustrated in fig 5 is a good example of the problems due to displacement of ICP microtransducer.
At the bedside, ICP measurements are normally confined to one hemisphere only, therefore any intracranial pressure gradients cannot be routinely monitored. Drift of ICP transducers14 can also be a source of gross misinterpretations. The measurement of ABP from the radial or dorsalis pedis arteries is not always representative for arterial pressure in the basal brain arteries, particularly under stress or in the presence of continuous infusion of active vasopresors.
CPP: NOT A NUMBER BUT A CONDITION FOR CEREBRAL BLOOD TO FLOW
In clinical practice, brain perfusion is better represented by global CBF, rather than by a numerical value of CPP. Therefore, monitoring of CBF with all its heterogeneity (both spatial and temporal) would seem more appropriate. However, at the present stage of medical technology, there is no method for continuous CBF monitoring available. Of course, MRI or PET would provide the best accuracy and spatial resolutions but their availability at the bedside is limited.15 Laser Doppler flowmetry, and brain tissue biochemical monitoring, although promising, give only localised readings.16 17 Jugular blood oximetry is useful, but technical problems often reduce its reliability. Moreover, in the supine body position, a significant fraction of the venous drainage from the brain takes place through the prevertebral venous plexus, rather than the jugular veins.
The use of transcranial Doppler flowmetry has many advantages. It is non-invasive and repeatable, signals may be obtained from different arteries at the same time, and continuous monitoring is possible with more efficient bilateral probe holders and with the advent of autofocusing piezo-array ultrasound transducers glued to the scalp.
The problem lies in how to interpret blood flow velocity as a volume flow. Some attempts, although only partially successful, have been made using a specific analysis of Doppler spectra.18 The most promising approach to monitor brain perfusion seems to be to use the distinctive features of the blood flow velocity waveform. Many authors have pointed out that either an increase in transcranial Doppler pulsatility,9 19 diminishing diastolic flow velocity,20 21 or a decrease of the ratio of diastolic to mean flow velocity10 reliably indicate decreased brain perfusion. Therefore, transcranial Doppler waveform can be “translated” to brain perfusion continuously. This translation does not necessarily need to be done on the “'number to number” basis. In fact, in clinical practice the most often asked question is whether perfusion is adequate or not adequate.
On the other hand, almost all therapy protocols are based on CPP as a number. This was a reason why the formula: ABP×FVd/FVm, was initially proposed.10
ACCURACY OF ESTIMATION OF CPP VIA nCPP
Both CPP=ABP−ICP and nCPP can be calculated with a limited accuracy and both are based on different physiological models which may not always be valid. Nevertheless, CPP calculated as the difference between ABP and ICP has become a gold standard with which an nCPP should be compared.
In our trial, the overall accuracy of this nCPP estimation was surprisingly good. The 95% confidence interval for predictor was more than 50% smaller than reported using previous methods.6 8 The clinician may expect that in 80% of cases the error will be less than 10 mm Hg and in 90% of cases less than 13 mm Hg. Apart from a value of nCPP, the conditions for brain perfusion can be visually assessed from the transcranial Doppler waveform. Confounding factors in the estimation of CPP using nCPP have been identified previously.10 These include changes in arterial blood CO2 concentration, hyperaemia, and probably vasospasm. Our study confirmed previous findings10 that a non-invasive technique to measure CPP can reliably detect dynamic phenomena such as “B waves” and plateau waves or other transitional changes in CPP.
SIDE TO SIDE DIFFERENCE IN nCPP
First attempts to demonstrate interhemispheric pressure gradients in the 1990s,22 all indicated poor correlation between side to side asymmetry based on CT and invasive ICP differences. Continuous measurement of bilateral nCPP may be useful in clinical practice in future, but the validity of this new parameter should be investigated thoroughly beforehand. Although our group analysis was limited (n=25) there was early evidence of clinical significance of side to side difference in nCPP (dCPP=left nCPP− right nCPP).
Firstly, dCPP obviously depends on how accurately the MCAs are insonated. Side to side differences in the angle of insonation are not crucial as the ratio of FVd/FVm does not depend on angle of insonation (providing the angle is not larger than 30o). However, when mounting ultrasound probes on a patient's head, care should be taken to optimise symmetry of the flow velocity readings on the screen.
The absolute value of dCPP increased significantly with increased mean ICP. Similar findings have been published in a report23 on bilateral jugular venous oxygen concentrations after head injury: side to side differences in sJO2 increased with intracranial hypertension.
The absolute value of dCPP correlated with our simplified brain swelling score: in severe swelling (score=3) the value of averaged side to side differences was significantly larger (fig 3 C) than in lower swelling score groups.
The number of patients with midline shift was small (n=4), therefore our findings concerning dCPP can be only interpreted as anecdotal. Nevertheless, in all four patients nCPP was significantly greater in the swollen hemisphere. Conventional wisdom says the opposite: if ABP on both sides is the same, and ICP on the “expanding” side is greater,22 a lower CPP would be expected on this side. Our finding of an increased nCPP in the swollen hemisphere can be explained by relative hyperaemia, perhaps associated with ipsilateral vasogenic oedema. This hypothesis can be supported by findings on bilateral ultrasongraphy after brain trauma,24 indicating that autoregulation of CBF is significantly impaired on the expanding side of the brain. Failure of autoregulation at an early stage after brain trauma is commonly caused by vasoplegia leading to a decrease of cerebrovascular resistance and functional hyperaemia (hyperperfusion associated with a greater than expected value of nCPP) on this side of the brain. Indeed, in our patients absolute blood flow velocity was significantly higher in the swollen hemisphere (p<0.05; n=4). Nevertheless, these early hypotheses and the real nature of dCPP need further clinical investigation.
Conclusion
The prototype transcranial Doppler based device for non-invasive bilateral monitoring of CPP showed satisfactory accordance with direct CPP measurements in a range from 60 to 100 mm Hg. The major advantage of the method lies in the ability to monitor patients in whom insertion of an ICP transducer cannot by justified and to detect whether CPP decreases, increases, or stays constant in a given case over time.
Acknowledgments
EAS received a scholarship from the University of Clermont-Ferrand, France. MC and SKP are on leave from Warsaw University of Technology, Poland. SKP received the “Fees Studentship” towards his PhD research from the Cambridge Overseas Trust, the “Overseas Research Studentship” awarded by the Committee of Vice-Chancellors and Principals of the Universities of the UK. MC acts as a consultant to Deltex, Chichester, UK.