Article Text

Abstract
Thinning or dehiscence of the superior semicircular canal may occur on the middle cranial fossa floor or adjacent to the superior petrosal sinus (SPS). However, no symptomatic cases of superior canal dehiscence by SPS have been previously described. A 45-year-old woman presented with left-side pulsating tinnitus, autophony and disequilibrium. Examination showed conductive hearing loss and decreased threshold of vestibular evoked myogenic potential in the left side. Sound and vibration stimuli and positive pressure insufflations into the left ear evoked mainly torsional nystagmus instead of vertical-torsional nystagmus. High-resolution temporal bone CT revealed a dehiscence of the superior canal close to the common crus, which was encased by SPS. Symptoms and signs resolved after plugging the dehiscence through a middle fossa approach. Deep groove of SPS may cause superior canal dehiscence close to the common crus, and costimulation of the superior and posterior canals may explain the mainly torsional nystagmus induced by sound and vibration stimuli.
- Semicircular canal
- cranial sinuses
- pulsatile tinnitus
- vertigo
Statistics from Altmetric.com
Introduction
Superior semicircular canal dehiscence (SCD) syndrome is characterised by auditory and vestibular hyper-responsiveness induced by intense sound and changes in middle ear or intracranial pressure due to a bony dehiscence of the superior semicircular canal (SC).1–5 High-resolution temporal bone CT, lowered threshold of vestibular evoked myogenic potential (VEMP) and typical vertical-torsional eye movements aligned with the plane of SC evoked by sound, vibration or pressure stimuli are the basis for the diagnosis of the SCD syndrome.1–5 The usual site of dehiscence is the arcuate eminence where the most superior part of SC faces the middle cranial fossa dura.2 According to a recent temporal bone survey,2 dehiscence or thinning of SC was also caused by the superior petrosal sinus (SPS) as well as the middle fossa floor. In contrast to the abundance of SCD on the middle fossa floor, a symptomatic case of SCD by SPS has not been previously reported. We hereby report a case of SCD in which the dehiscence was encased by SPS. The location of SCD was closer to the common crus than the usual sites of SCD, resulting in mainly torsional nystagmus induced by various stimuli.
Subject and methods
Subject
A 45-year-old woman visited a dizziness clinic for an evaluation of chronic disequilibrium for 3 years. She also experienced left-side pulsating tinnitus for 16 years, and autophony and audible body sounds for 10 years. The tinnitus was aggravated by Valsalva manoeuvres. The tympanic membranes were normal and spontaneous nystagmus was absent.
Diagnostic tests
Eye-movement recording with application of stimuli
Horizontal, vertical and torsional eye movements were recorded using three-dimensional video-oculography (resolution, 0.1°; sampling rate, 60 Hz; SMI, Teltow, Germany).6 For evaluation of the Tullio phenomenon, 500 Hz and 1 kHz short tone bursts (stimulation rates: 1.1/s, 2.1/s, 3.1/s; rise and fall time: 2 ms; plateau time: 3 ms; intensity: 93 dB nHL) were used. The vibratory stimuli were applied to one mastoid tip for up to 10 s and then moved to the contralateral side. The oscillation frequency was 100 Hz (±5%), and the contact area was 0.9 cm2 (VVIB 100, Synapsys, Marseille, France). The mean slow phase velocities of the spontaneous and induced nystagmus were measured during sound stimulation and vibration after excluding slow phases with additional blinks.
Vestibular evoked myogenic potentials
VEMPs were recorded with surface electrodes on the ipsilateral sternocleidomastoid muscle during contralateral neck rotation on supine position. Alternating tone bursts (500 Hz; rate: 2.1/s; rise-fall time: 2 ms, respectively; plateau time; 3 ms; 128 repetitions; Navigation Pro; Biologic Systems, Mundelein, Illinois) were provided to each ear. The threshold was obtained by lowering the sound stimulus from 93 dB nHL by 5 dB.
CT scanning
High-resolution temporal bone CT was performed with MX8000-IDT (Phillips Medical Systems, Best, The Netherlands) using the following parameters. Collimation: 4×0.75 mm; slice thickness: 0.75 mm; mode: high resolution; 250 mA and 120 kVp per slice. The images were displayed on IMPAX 4.5 diagnostic PACS system (AGFA healthcare, Mortsel, Belgium), and 3D multiplaner reconstruction was subsequently used to obtain an oblique coronal reformation image parallel to SC.
Clinical assessment
Audiometry showed conductive hearing loss with a maximum air-bone gap of 25 dB at 250 Hz in the left ear (figure 1A). However, the stapedial reflex was present, and the VEMP threshold was 58 dB in the left ear, 20 dB lower than that in the right ear (figure 1B). Tone burst stimulation to the left ear produced mainly clockwise (from the viewpoint of the patient) torsional nystagmus (4.5 °/s) with few vertical eye movements (figure 1C). Left-side mastoid vibration induced counterclockwise torsional (47.8 °/s) with left beating (11.4 °/s) nystagmus (figure 1C). During positive-pressure insufflations into the left ear canal with a Politzer bag, the patient showed subtle clockwise torsional eye movement.
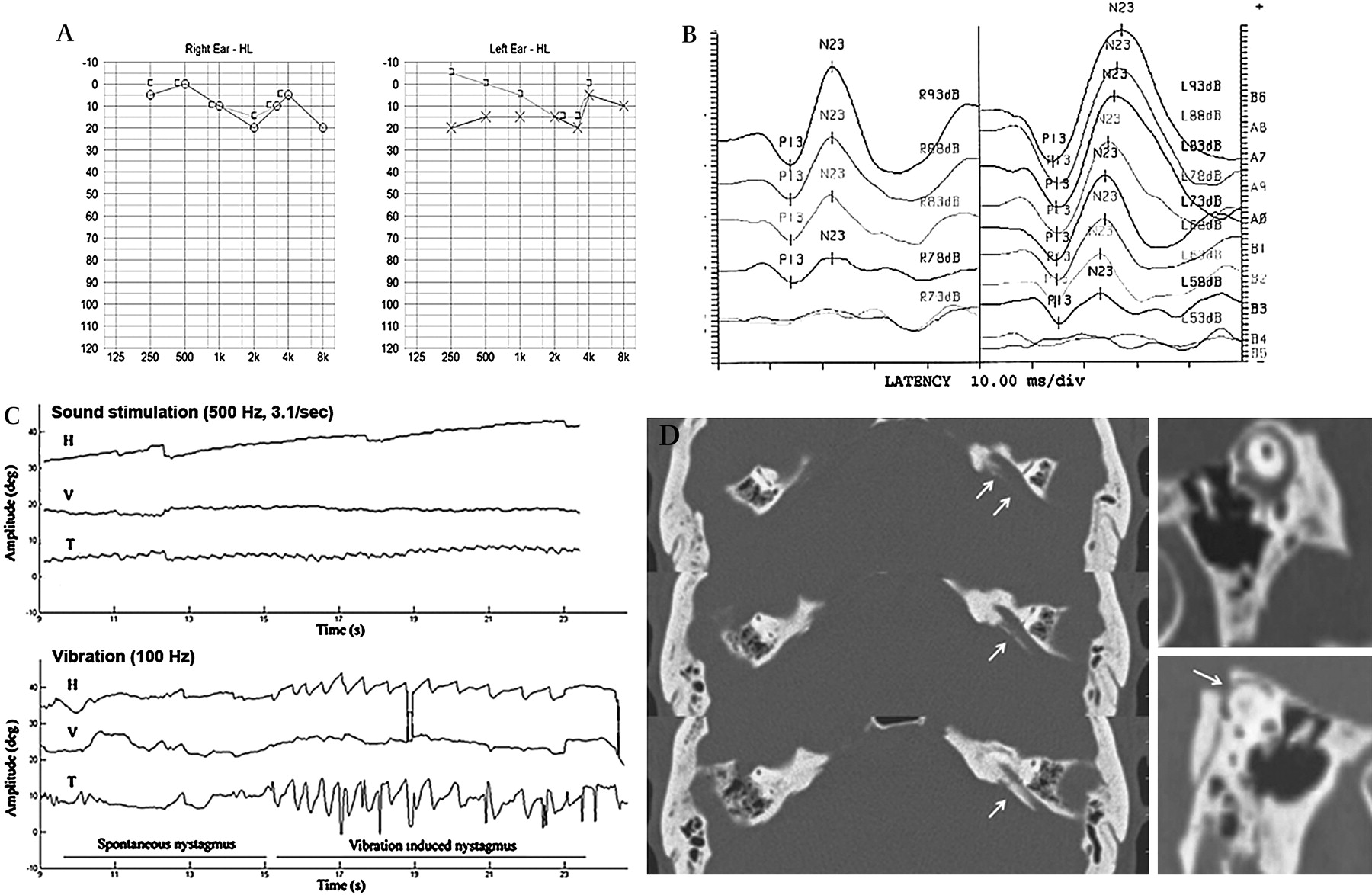
Diagnostic tests. (A) Pure tone audiometry showing conductive hearing loss with a maximum air-bone gap of 25 dB at 250 Hz in the left ear. (B) VEMP threshold: 58 dB in the left ear, 20 dB lower than that in the right ear. (C) Video-oculographic findings showing clockwise (from the viewpoint of the patient) torsional nystagmus (4.5 °/s) with few vertical eye movements of left ear by 500 Hz tone burst stimulation. Left-side mastoid vibration (100 Hz) inducing counterclockwise torsional (47.8 °/s) with left beating (11.4 °/s) nystagmus (H: horizontal, V: vertical, T: torsional). (D) High-resolution temporal bone CT showing the bony dehiscence of the left superior semicircular canal by the superior petrosal sinus (arrows).
On high-resolution temporal bone CT, left SPS ran lateral to the petrosal ridge on the middle cranial fossa and encased the posterior limb of SC, while right SPS ran along the medial side of the petrosal ridge (figure 1D).
Surgical procedure and postoperative results
Surgery was performed through a middle cranial fossa approach. The middle fossa dura was elevated to the site of SPS, and further dissection was performed in the anterior and posterior directions. During this procedure, the suspected area of the attachment between the dehiscence and SPS was preserved to avoid possible injury to the membranous labyrinth. Just after separating the SPS attachment from the dehiscence, the prepared soft tissue and bone plate were packed into the site of dehiscence, and then the temporalis fascia and a thin bony plate were positioned. Dissection was guided by a navigation system (In2Vision, Cybermed, Seoul, Korea) during the procedure. After surgery, pulsating tinnitus, autophony and disequilibrium were resolved. Induced nystagmus by sound and vibration also disappeared. Laboratory tests after 6 months showed closure of air-bone gap (figure 2A) and elevated VEMP threshold to 83 dB (figure 2B) on the left ear.

{kind=link}
{kind=link}
Six months after surgical intervention. Note that the air-bone gap is closed (A) and the left-side VEMP threshold (B) is increased to 83 dB nHL.
Discussion
The SPS runs along the crest of the petrous temporal bone, connecting the cavernous sinus to the transverse sinus. Normally, the SPS runs postero-laterally from the cavernous sinus. It runs along the superior petrosal sulcus of the temporal bone and enters the transverse sinus on the inner surface of the mastoid portion of the temporal bone.7 8 The SPS is the second closest structure to the SC next to the middle cranial fossa floor, and the possibility of SCD adjacent to SPS had been suggested previously through a temporal bone survey. In that survey, dehiscence of SC by the deep groove of SPS occurred in four ears, but none of the respondents reported clinical symptoms compatible with SCD syndrome. While individual ear symptoms might not be described in detail for the temporal bone collections, another speculation for the asymptomatic character of the SCD caused by SPS could be the size of the dehiscence. That is, the course of SPS and the plane of SC form almost a 90° angle, and if the two structures were to abut and form a dehiscence on the SC, the size of the window would be smaller than that of the SCD on the arcuate eminence.
Although the natural history of SCD is not completely understood, persistent CSF pulsation may efface the protruding bony structure exposing the subperiosteal layer of SC. When the window reaches a critical size, audiovestibular symptoms may occur. The presence of a third window increases inner-ear fluid displacement by oscillation of the stapes. Since the crista ampullaris of SC lies in the course from the oval window to the third window,9 SC would be the most vulnerable structure among the five vestibular sensory organs. The response of SC would be excitatory during inward mobilization of the stapes by positive pressure on the external ear, loud sounds or increasing middle ear pressure during Valsalva manoeuvres. Excitation of the left SC in turn would generate upward and clockwise eye movements by stimulating the ipsilateral superior rectus and contralateral inferior oblique.2 4 5 However, the vertical component of the induced nystagmus was very small in this patient, compared with those reported in previous patients.5 10 Considering that the location of the dehiscence by SPS was closer to the common crus rather than to the superior canal ampulla, the posterior canal seems to have been costimulated by oscillation of the stapes. Simultaneous stimulation of the left superior and posterior canals would generate rather pure torsional eye movements, since the vertical components would cancel each other out.
In summary, the SPS is the second closest structure to the SC, and the variation in the course of SPS may abut with SC, resulting in SCD syndrome. Results from audiometry and vestibular evoked myogenic potential test showed similar with SCD in arcuate eminence, but the pattern of induced nystagmus was different. It showed mainly torsional with few vertical components, since the location of dehiscence made by the deep groove of SPS was closer to the common crus. Surgical separation of the sinus from the membraneous labyrinth was successful in resolving symptoms and signs through a middle fossa approach.
References
Footnotes
Funding This article was supported by Seoul National University Bundang Hospital Research Fund (grant number 02-2007-009).
Competing interests None.
Patient consent Obtained.