Article Text

Abstract
Background Recent studies using colour-coded Doppler sonography showed that chronic impaired venous drainage from the central nervous system is almost exclusively found in multiple sclerosis (MS) patients. This study aimed to investigate the intracranial and extracranial venous anatomy and the intracerebral venous flow profile in patients with MS and healthy controls using magnetic resonance venography (MRV).
Methods Twenty patients with definite MS and 20 age- and gender-matched healthy controls were examined. MR imaging was performed on a whole-body 3T MR system including both 3D phase-contrast and dynamic 3D contrast-enhanced MRV as well as flow quantification of the internal cerebral veins and the straight sinus. Image analysis was performed by two experienced interventional neuroradiologists blinded to clinical data and structural brain imaging. The intracranial and extracranial neck veins were analysed for stenosis/occlusion and alternative venous drainage pattern.
Results A completely normal venous anatomy was observed in 10 MS patients and 12 controls. Anomalies of the venous system (venous stenosis/occlusions) were found in 10 MS patients and eight healthy controls. An anomalous venous system in combination with associated alternative venous drainage was observed in six MS patients and five healthy controls. Flow quantification showed no venous backflow in any MS patient or control.
Conclusions Findings suggestive of anomalies of the cranial venous outflow anatomy were frequently observed in both MS patients and healthy controls. Given the normal intracranial venous flow quantification results, it is likely that these findings reflect anatomical variants of venous drainage rather than clinically relevant venous outflow obstructions.
- Multiple sclerosis
- MRA
- neuroradiology
- MRI
- cerbrovascular
Statistics from Altmetric.com
Introduction
Multiple sclerosis (MS) is considered to be an immune-mediated disease of the central nervous system (CNS) characterised by inflammation, demyelination and neurodegeneration. The current pathophysiological concept is based on a complex interaction of autoreactive T- and B cells recognising myelin antigens of CNS.1 2 Clinically and radiologically, MS is characterised and defined by clinical symptoms and signs that reflect lesion dissemination in space and time.3 4
Recently, the concept of chronic cerebrospinal venous insufficiency (CCSVI) in MS has been postulated. The concept of CCSVI suggests that venous drainage from the CNS is frequently impaired in MS patients but not in healthy control subjects.5 6 It has been proposed that chronic venous reflux and hypertension might lead to increased iron deposition in the brain, which might lead to subsequent MS pathology including inflammation and neurodegeneration.7 8 The initial data on CCSVI stem from studies using extracranial colour-Doppler (ECD) and transcranial colour-coded Doppler sonography (TCCS) showing 288 normal and 257 abnormal findings in MS patients compared with 861 normal and 24 anomalous parameters in healthy controls. One of the criteria defining abnormal cerebrospinal venous drainage was the presence of reflux in the deep cerebral veins. These findings in combination distinguished MS with a sensitivity, specificity, positive and negative predictive values of 100%.5
Given the major implication of these findings in terms of both MS pathogenesis and treatment concepts, independent research is needed in order to confirm or refute the original findings. A major point of criticism is that the concept of CCSVI is mainly based on ECD and TCCS methods, which are strongly operator-dependent, and that intracranial venous blood flow is difficult to measure. In contrast, magnetic resonance venography (MRV) is a non-invasive, sensitive, operator-independent technique for the evaluation of venous anatomy and pathological changes, and is widely used in the clinical setting.9 10 Such an objective imaging technique is also needed in case treatment of a morphological abnormality is contemplated. However, data on MRV in the detection of venous outflow abnormalities suggestive of CCVSI are rather limited.
The aim of our study was to investigate the cerebral and cervical venous outflow anatomy in patients with MS and matched healthy controls with MRV. Using MR flow quantification, the second aim was to determine whether certain venous drainage patterns might be associated with pathological intracranial venous backflow.
Patients and methods
Patients
This study was designed as a comparative cross-sectional in patients with definite MS and age- and sex-matched healthy control subjects. The study was approved by the institutional review board of the VU University Medical Center Amsterdam, and written informed consent was obtained from all participants. Inclusion criteria were: diagnosis of MS according to the revised International Panel criteria, age 18–50 years, ambulant or healthy volunteer.3 Exclusion criteria were: history of other immunological and or malignant diseases, pregnancy, contraindication for MRI (eg, pacemaker), claustrophobia, allergic reactions to gadolinium-based contrast media and impaired renal function. Twenty patients with the diagnosis of MS presenting to our MS outpatient clinic were included. Nineteen patients had a relapsing-remitting and one patient a primary progressive disease course. Additionally, 20 age- and gender-matched healthy controls were selected. The demographic and clinical characteristics of the study population are given in table 1.
Characteristics of multiple sclerosis patients and healthy control subjects
MRI acquisition
MRI was performed on a whole-body 3T MR system (Signa HDXt, General Electric, Milwaukee, Wisconsin) using an eight-channel head coil with a maximum slew rate of 150 mT/m/s and a maximum gradient amplitude of 50 mT/m.
The MRI protocol consisted of a multisequence protocol including the following pulse sequences:
Structural brain imaging: axial two-dimensional (2D) proton-density/T2-weighted fast spin echo (matrix 416×320, field of view (FOV) 25×19 cm2, slice thickness 3.0 mm, repetition time (TR) 4100 ms, echo time (TE) 20/112 ms, echo train length (ETL) 24, number of signal averages (NSA) 2), sagittal 3D fluid-attenuated inversion-recovery (FLAIR) (matrix 224×224, FOV 25×25 cm2, slice thickness 1.2 mm, TR 8000 ms, TE 2352 ms, inversion time 124 ms, ETL 230, NSA 1), axial 2D T1-weighted spin echo (matrix: 224×224, FOV 25×19 cm2, slice thickness 3.0 mm, TR 580, TE 8 ms, NSA 1) after intravenous administration of contrast media (0.1. mmol/kg/bodyweight Gadobutrol, Gadovist, Bayer Schering Pharma, Germany). 3D FLAIR images were reformatted into axial orientation (3 mm slice thickness).
MRV: 3D (Inhance) phase-contrast angiography (FOV 32×26 cm2, slice thickness 1.4 mm, TR 11.6 ms, TE 4.9 ms, flip angle (FA) 8°, 19 projection images, flow encoding 15 cm/s). Multiphase 3D contrast-enhanced MR angiography (matrix 320×224, FOV 32×24 cm2, slice thickness 3.0 mm, TR 4.3 ms, TE 1.4 ms, FA 30 degrees, five dynamic acquisitions). After acquisition, images of all five dynamic acquisitions were subtracted from the base image for each location. The Inhance 3D MRA was sagitally acquired covering the head and neck, and reformatted into 18 maximum intensity projections around the CC axis. The FOV of the phase-contrast angiography included the whole brain and at least the distal half of the neck, and the FOV multiphase 3D contrast-enhanced MR angiography ranged from the aortic arch to the confluens sinuum. Therefore, the crucial area of the skull base and the upper neck (most of the described cases of venous stenosis were located in this area) was depicted by both angiographic methods.
Phase-contrast flow quantification: a phase-contrast gradient echo sequence was acquired to quantify the flow in the internal cerebral veins and straight rectus: 2D acquisition, TR 11.2 ms, TE 4.1 ms, matrix 448×448, FA: 8°, FOV: 26×26 cm2, slice thickness 5 mm, cardiac-gated, reconstructed with 30 cardiac phases and four views per segment. Velocity encoding: 50 cm/s. The flow quantification was done in two planes perpendicular to the internal cerebral veins and the straight sinus. Postprocessing and analysis of the data were performed on an AW workstation by a rater (physicist, WDG) who was blinded to the structural and angiographic images as well as to the clinical data of the study subjects. Both internal cerebral veins and the straight sinus were analysed separately. Flow plots were made and checked for reflux or almost stationary flow (figure 1).
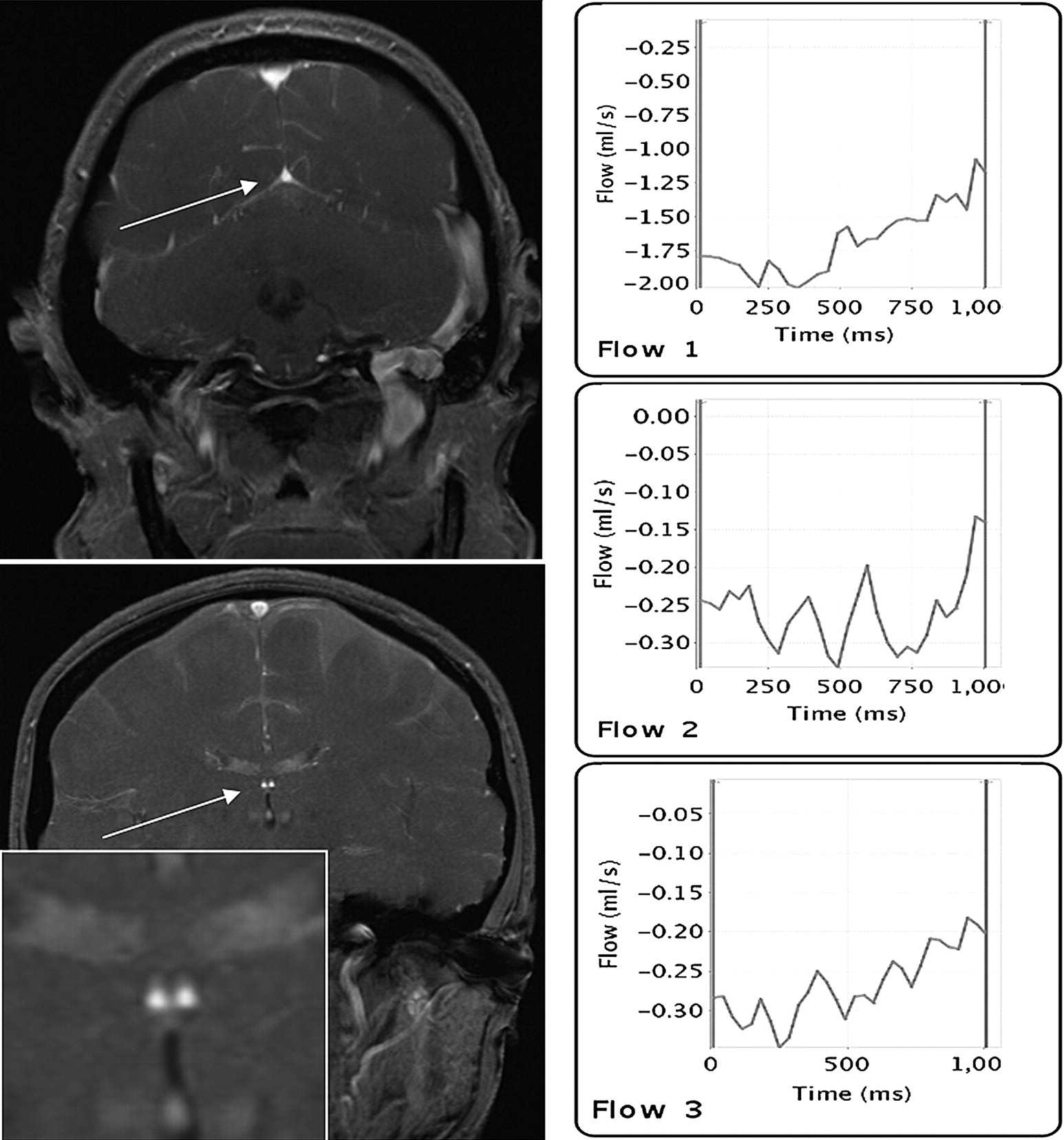
Venous blood-flow quantification in the straight sinus and internal cerebral veins. Left-hand side: regions of interest, placed on coronal phase-contrast images for quantitative flow measurement in the straight sinus (top) and both internal cerebral veins (bottom). Measurements were performed in planes perpendicular to vessel directions. Right-hand side: example of quantitative flow patterns of a healthy control with normal findings for quantitative flow profiles and without any evidence of venous backflow/reflux in the straight sinus (top) and internal cerebral veins (middle and bottom).
Image analysis
As a first step, image annotations and identifiers were removed and replaced by new unique identification numbers. The structural MR images (PD/T2-weighted, FLAIR and T1-weighted images) and angiographic images were stored separately.
All angiographic images were scored by two interventional neuroradiologists (RVDB, JCB) in consensus. Both readers only had access to the angiographic series but not to the structural MR images, and were blinded to the demographic (except date of birth) and clinical information of all study subjects.
The following intracranial and extracranial venous structures were analysed separately for possible abnormalities (aplasia, hypoplasia, stenosis and occlusion). Extracranial: external jugular veins, internal jugular veins. Intracranial: superior sagittal sinus, inferior sagittal sinus, straight sinus, transverse sinus, sigmoid sinus, great cerebral vein (of Galen), internal cerebral veins. A stenosis was defined as a narrowing of the vessel of at least 50%, and an occlusion was defined as no patency of the vein without any flow on both the phase-contrast and contrast-enhanced MRV.
In addition, the entire intracranial and extracranial venous system was scored for alternative venous drainage with or without associated stenosis of certain venous structures. Indicator of alternative drainage pattern also considered venous structures/pathways which were not scored for abnormalities in the first step such as superficial cerebral veins, cortical veins, basal vein (of Rosenthal), vein of Trolard, choroidal veins, thalamostriate (terminal) veins, superior and inferior petrosal sinus, cavernous sinus, occipital sinus, epidural veins, occipital plexus, vertebral plexus and deep cervical veins. Physiologically asymmetrical venous drainage patterns in particular of the transverse and sigmoid sinus were not considered as pathological.
The final conclusive classification of the venous systems in terms of findings suggestive of an anomalous intracranial venous drainage according to our imaging protocol and rating systems was based on the following definition:
No evidence of anomalous venous anatomy: normal/physiological venous drainage without evidence of venous stenosis and/or alternative venous drainage;
Anomalous venous anatomy: presence of an extra- and/or intracranial venous stenosis in combination with or without alternative (compensatory collateral) venous drainage;
possibly anomalous venous anatomy: presence of an extra- and/or intracranial venous stenosis without alternative venous drainage pattern;
probably anomalous venous anatomy: presence of an extra- and/or intracranial venous stenosis in combination with alternative (compensatory collateral) venous drainage.
Results
MRV
An anomalous venous system was found in 10 MS patients compared with eight healthy controls (table 2). An intracranial and/or extracranial venous stenosis was observed in 10 MS patients and eight healthy controls; two MS patients showed a combination of an intracranial and extracranial venous stenosis. One MS patient and one healthy control had a bilateral intracranial venous stenosis; four MS patients and three healthy controls showed a bilateral extracranial venous stenosis. Two MS patients showed a combination of a stenosis of the internal and external jugular vein. Figures 2–7 present examples of normal and anomalous venous outflow anatomy in MS patients and healthy controls.
Magnetic resonance venography results of multiple sclerosis patients and healthy controls
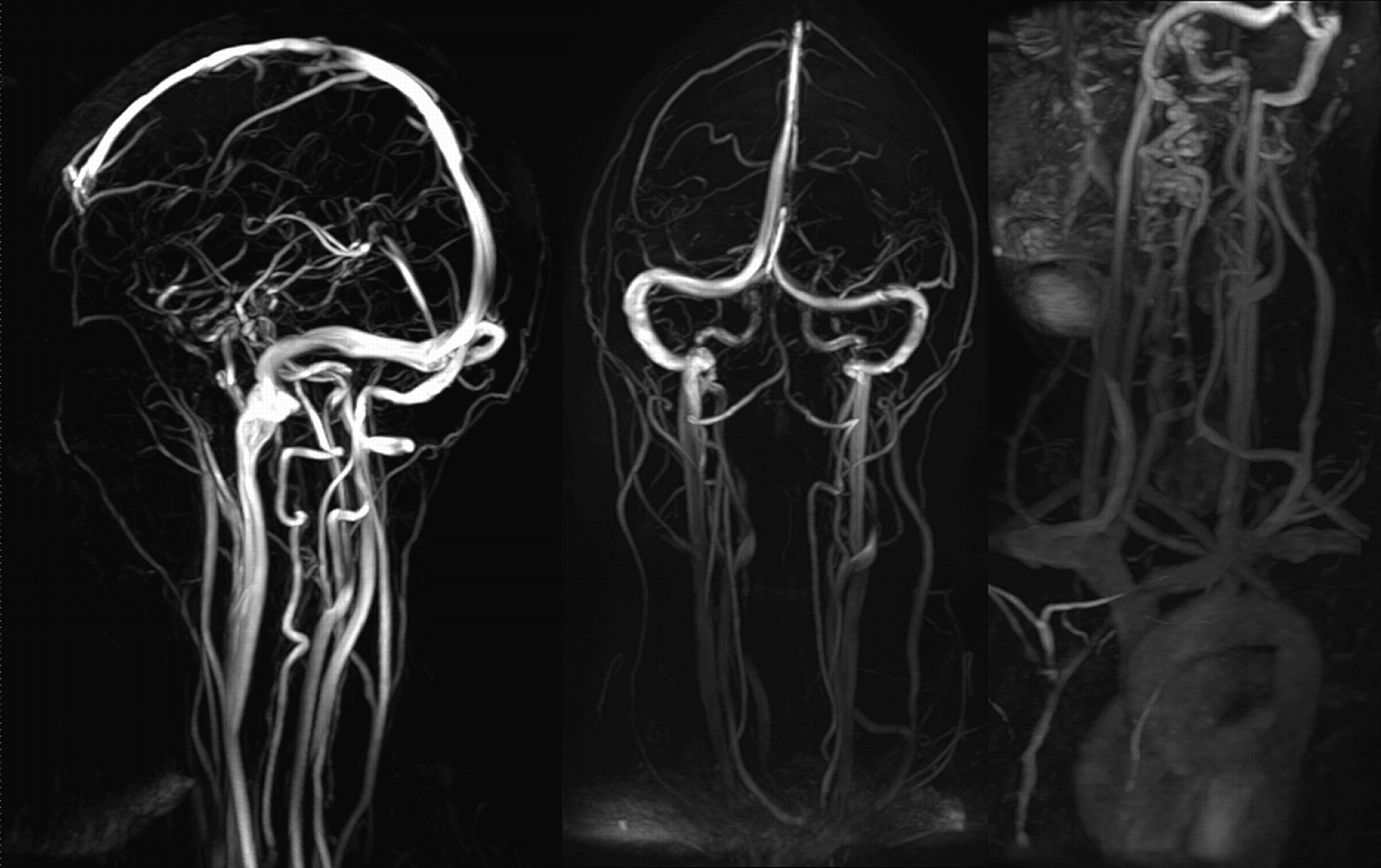
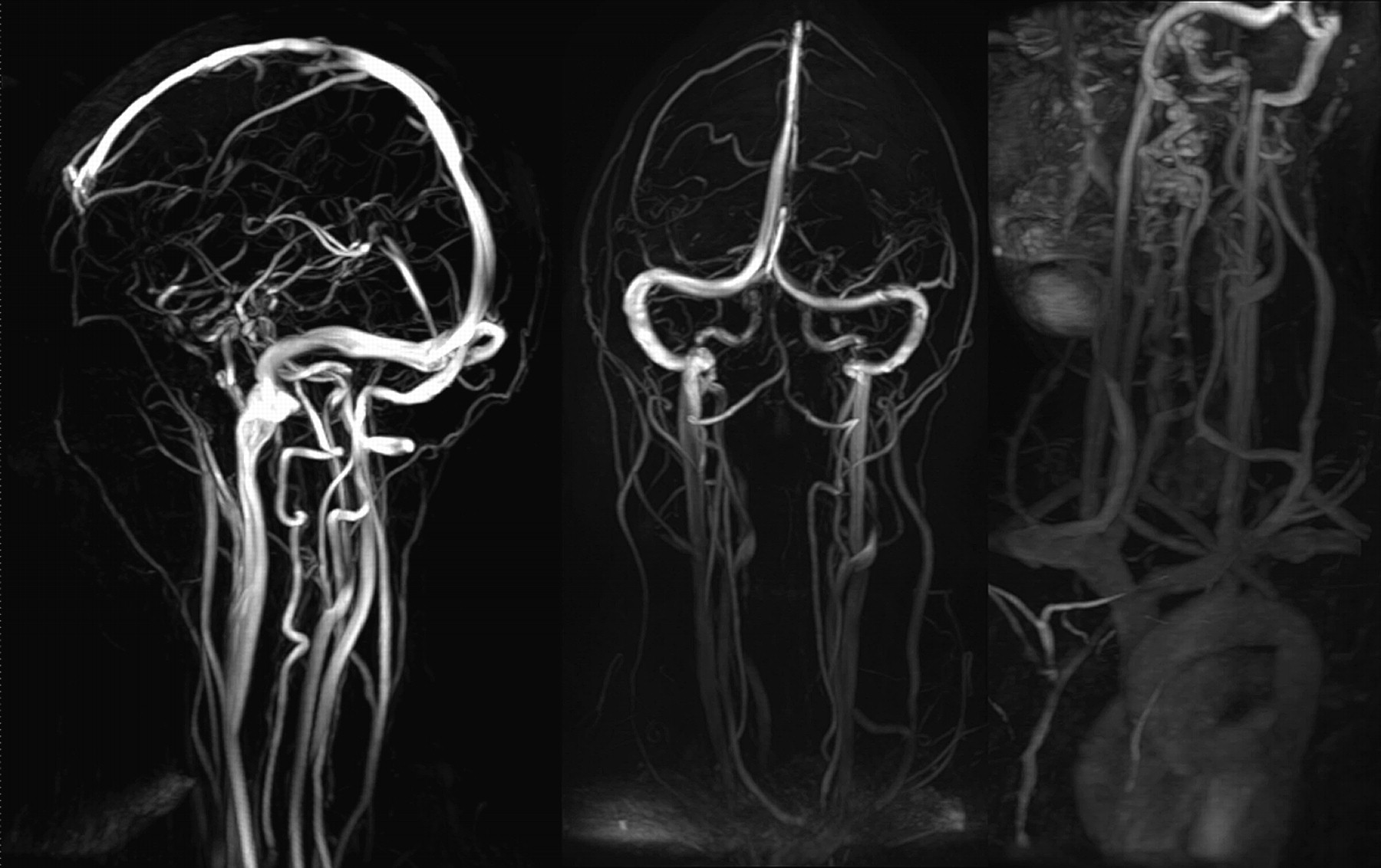
Maximum intensity projection images of the phase-contrast (left, middle) and contrast-enhanced (right) magnetic resonance venography obtained from a healthy control. Intracranial and cervical venous anatomy was classified as normal without any evidence of venous stenosis and/or alternative venous drainage.

Maximum intensity projection images of the phase-contrast (left, middle) and contrast-enhanced (right) magnetic resonance venography of a 44-year-old MS patient. The intracranial and cervical venous anatomy was classified as normal without evidence of venous stenosis and/or alternative venous drainage. Note the prominent deep cervical vein (arrow) without any signs of congestion, which was considered as a normal anatomical variant.

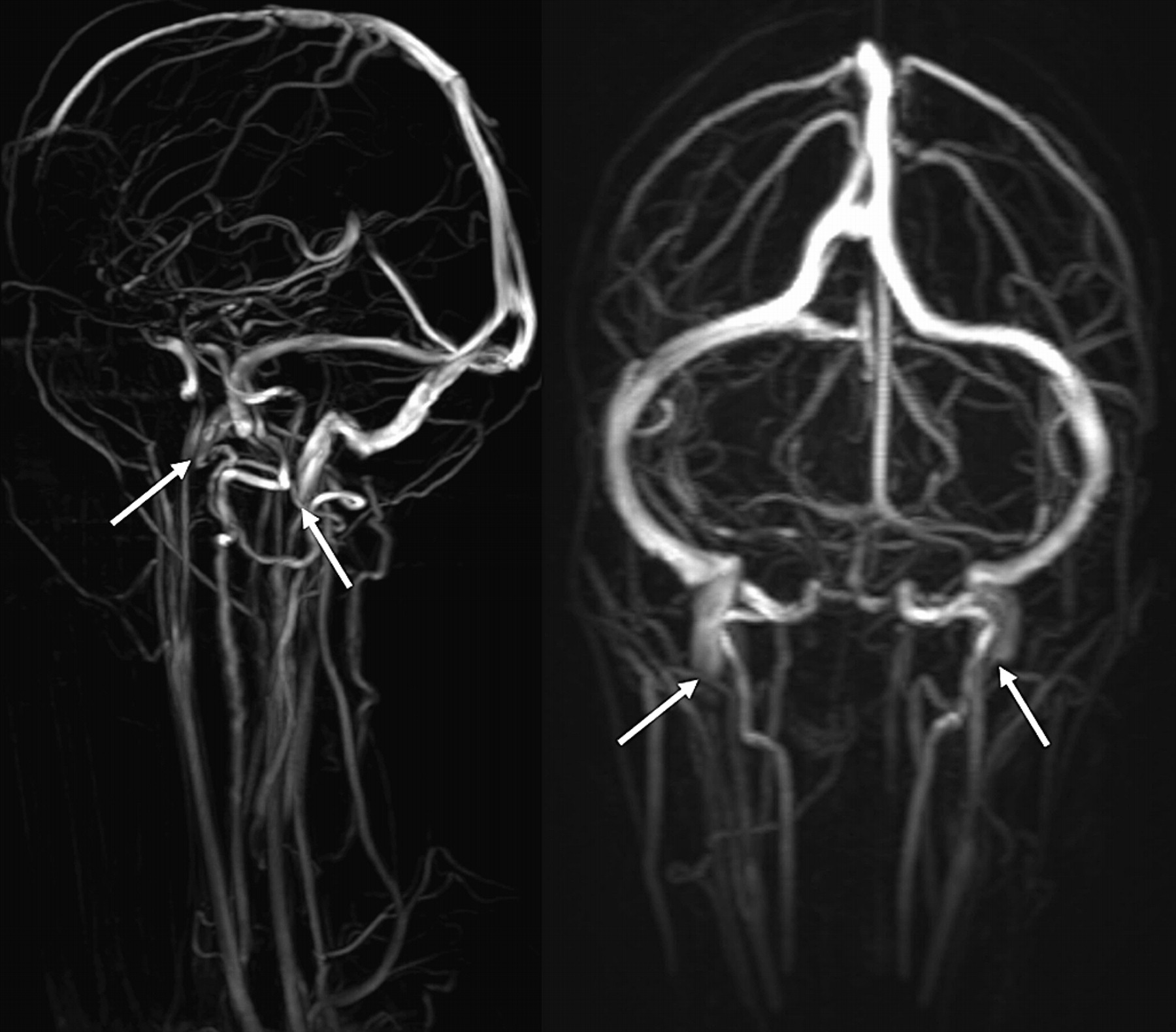
Maximum intensity projection images of the phase-contrast (left, middle) and contrast-enhanced (right) magnetic resonance venography of a 25-year-old MS patient with a bilateral stenosis (arrows) of the internal jugular vein, which could be easily identified on the phase-contrast magnetic resonance venography. In particular, the contrast-enhanced magnetic resonance venography showed a prominent cervical and occipital venous drainage pattern including the occipital vein and external jugular vein (arrows) with signs of congestion.

Maximum intensity projection images of the phase-contrast (left, middle) and contrast-enhanced (right) magnetic resonance venography of a 47-year-old healthy control with a persistent bilateral stenosis of the internal jugular vein (closed head arrows) and a dilatation and congested appearance of the cervical and occipital venous drainage system including the occipital vein and external jugular vein.
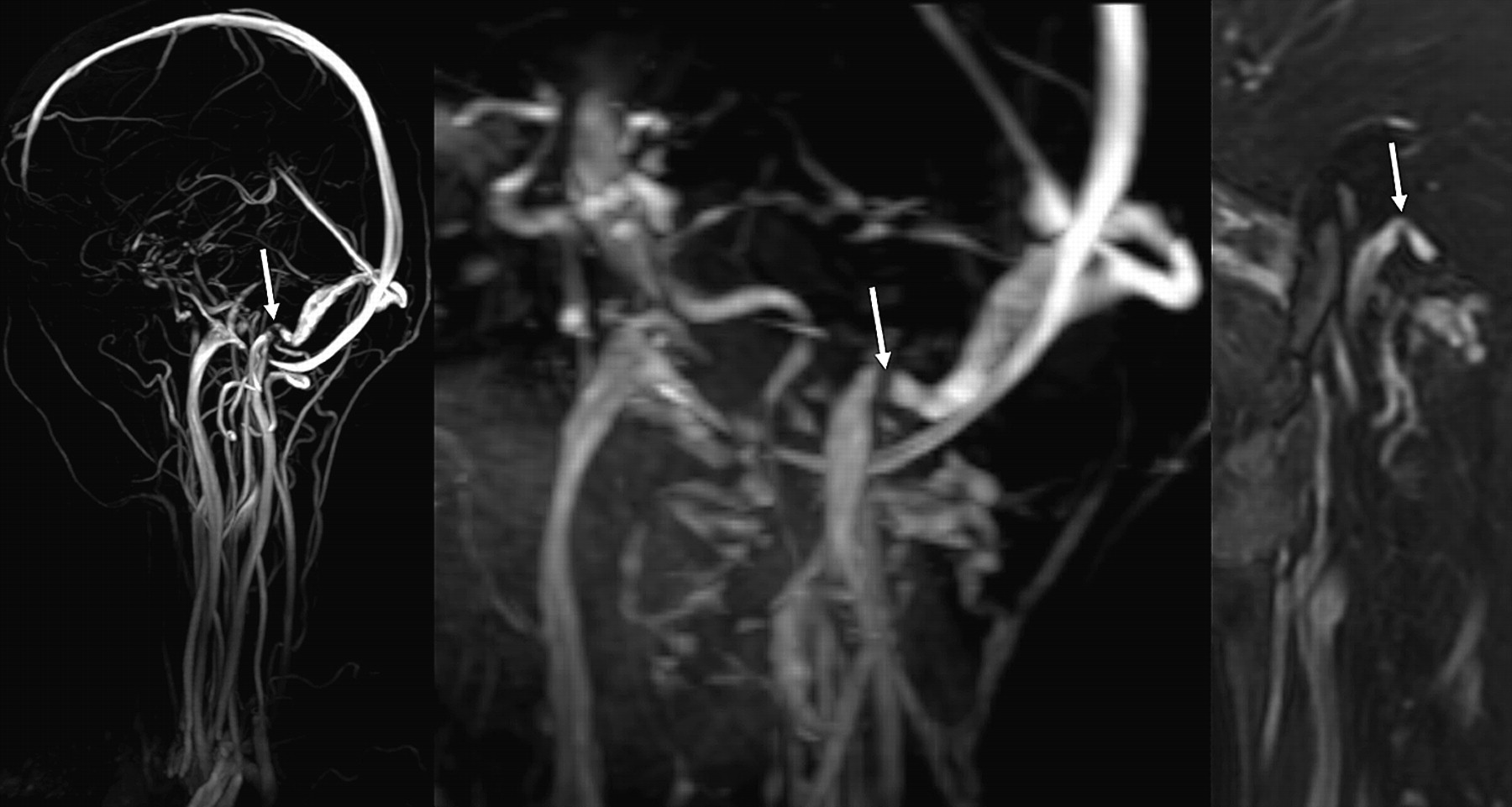
Maximum intensity projection images of the phase-contrast (left) and contrast-enhanced (middle) magnetic resonance venography showing a stenosis of the right sigmoid sinus (arrows) of a 35-year-old MS patient without any signs of associated abnormal (collateral) drainage. This stenosis could also be identified on the source images of the contrast-enhanced MRV (right).
Maximum-intensity projection images of the phase-contrast magnetic resonance venography of a 27-year-old healthy control with a bilateral stenosis of the internal jugular veins (arrows) without any signs associated abnormal (collateral) venous drainage. In particular, no dilatation and congestion on the cervical and occipital venous drainage pathway could be observed.
In those healthy controls presenting with an alternative drainage pattern, the associated venous obstruction was located in the internal jugular vein (two bilateral stenosis, one unilateral stenosis, one occlusion) and in the sigmoid sinus (one subject). The location of venous obstruction in all MS patients with an associated alternative venous drainage was in the internal jugular vein (bilateral in four patients). The most frequent alternative drainage pattern was a drainage via the occipital, paravertebral and/or cervical venous plexus or external jugular vein in combination with a venous obstruction located in the internal jugular vein (in all six MS patients and four healthy controls).
Flow quantification
Among all study subjects, a total number of three veins were only visible on the MRV but not visible on the quantitative flow sequence scan probably due to slow flow: both internal cerebral veins could not be observed in one MS patient, and the left internal cerebral vein could not be observed in a healthy control. Overall, venous backflow/reflux could not be observed in a healthy control subject or in any MS patient (figure 8). In seven veins at some point during the cardiac cycle, an almost zero flow velocity was observed when compared with the main velocity. This occurred in two subjects (one MS patient and one healthy control each) in the straight sinus and in two other subjects (one MS patient and one healthy control each) in the left internal cerebral vein. In three other subjects (two MS patients, one healthy control) this flow pattern was observed in the right internal cerebral vein. However, backflow/reflux was not observed in any of these patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examples of quantitative venous blood flow analysis in the straight sinus (top row) and internal cerebral veins (middle and bottom row) of healthy controls (HCs) and multiple sclerosis (MS) patients who were classified as having a normal (left columns), possibly anomalous (middle columns) and probably anomalous (right columns) venous outflow anatomy. No venous backflow/reflux could be observed in any MS patient or HC.
Discussion
The recently introduced pathophysiological concept of CCSVI in MS patients and its possible implications on MS pathophysiology and treatment have raised great interest in both patient and medical community. So far, this theory is mainly based on ECD and TCCS. Doppler-encoded ultrasound is a strongly operator-dependent image modality and not easy to blind in terms of clinical features. In addition, TCCS is strongly dependent on a transcranial insonation window and angle, and has a limited resolution. The challenges of ECD and TCCS in terms of the diagnosis of venous outflow obstruction in MS patients is underscored by the fact that the initial findings suggesting the concept of CCSVI could not have not been reproduced by another recent ultrasound study.11
In this study, we aimed to investigate the cranial venous outflow anatomy of MS patients as well as age- and gender-matched healthy control subjects in order to validate the ultrasound based findings of venous outflow obstruction in MS patients. Using MR venography, a sensitive and reproducible imaging modality widely used in the clinical setting, we were not able to reproduce earlier ultrasonographic findings. A classical normal appearance of the intracranial and cervical venous system according to the anatomy textbooks was observed in about 50% of the MS patients and healthy controls. Cases with a possibly or probably anomalous venous outflow anatomy were almost equally distributed between MS patients and healthy controls. Our results are in line with a recently published venous and cerebrospinal fluid flow study including 21 MS patients and 20 healthy controls. The authors did not find any significant differences between MS patients and healthy controls concerning the blood flow in the internal jugular veins and prevalence of reflux in the internal jugular veins.12 These results underscore the fact that the venous vascular system of the brain and neck is quite complex and that variants of the classical venous anatomy can be observed in a substantial proportion of humans.13–16 The most important question remains the correct interpretation of these variants in terms of possible pathophysiological relevance, clinical consequences and the necessity of treatment.
In order to address the crucial question as to whether the observed findings suggestive of venous outflow abnormality effectively lead to a chronic venous backflow as described in Doppler ultrasound studies in MS patients, we performed MR phase-contrast flow quantification of the straight sinus and internal cerebral veins. Venous backflow/reflux could not be observed in any of our study participants, including those subjects diagnosed as having probably anomalous cranial venous outflow. Therefore, these results do not support the pathophysiological relevance of these alternative venous outflow patterns. In addition, it is unlikely that the anomalous venous anatomy is directly associated with MS symptoms and disease course or even the cause of MS.17 Even in patients with a real pathological venous outflow anatomy such as cerebral venous thrombosis or radical neck dissection removing jugular veins, higher incidences of MS have not been reported.18 Taking these facts into consideration, in our view this should lead to reluctance with respect to therapeutic interventions.19
It is difficult to compare our results directly with those obtained from previous Doppler ultrasound studies, since both methods are based on different techniques with their own advantages and drawbacks. A recently published study on intraindividual comparison between neck MRV, Doppler sonography and selective venography for the diagnosis of CCSVI in MS patients and healthy controls reported a substantial difference between MRV and Doppler ultrasound.20 However, the crucial question remains which of these diagnostic tests have to be considered as the gold standard. Some authors consider catheter angiography as the gold standard in the detection of cranial venous outflow anatomy. However, regardless of the imaging modality used, the crucial question remains whether findings suggestive of venous outflow obstruction reflect real pathologically and pathophysiologically relevant conditions or rather an anatomical variant. The work-up of possible venous obstructions requiring treatment would need to focus on identification of morphological lesions—this would require anatomical imaging (catheter angiography or MRV) rather than physiological evaluations (like blood-flow measurements with ultrasound).
We have to be aware that all available standard imaging approaches for the evaluation of the cranial venous system represent rather a snapshot. The venous blood flow is influenced by many different physiological factors and their interaction such as respiratory changes, swallowing, central venous pressure, position of the patient (supine, sitting, upright), muscle contraction, etc. Regarding the analysis of the intracranial and cervical venous systems, it is almost impossible to take all of these factors into account, regardless of the imaging modality used.
A limitation of our study is the limited number of MS patients and healthy control subjects, which limits the ability to draw definite conclusions. The sample size number was based on the suggested almost absolute difference in presence of venous abnormalities between MS patients and healthy controls. Nevertheless, the present sample size would allow one to find a difference of 50% or more with a power of about 0.8. In addition, our results based on MRV have not been confirmed or refuted by another imaging modality such as Doppler sonography. However, our study represents the largest case–control dataset of MRV in the evaluation cranial venous outflow in MS patients and healthy controls so far. Given the fact that the initial results suggesting that MS is associated with a pathological venous outflow anatomy presented sensitivity, specificity, positive and negative predictive values of 100%, our study population is large enough to refute these data. In addition, MRV results in this context using MR flow quantification have not yet been validated. However, larger studies using different imaging approaches are necessary to reproduce and validate these data.
In conclusion, these data suggest that the cranial and cervical venous system on MRV is very complex and highly variable in normal healthy controls as well as in MS patients. Findings suggestive of anomalous cranial venous outflow in terms of venous stenosis alone or in combination with alternative venous drainage pattern are equally distributed between MS patients and healthy controls. Given the fact that these findings are not associated with venous backflow based on MR flow quantification, it is more likely that these situations represent anatomical variants rather than pathological conditions that might be causally associated with MS pathology.
Acknowledgments
The authors wish to thank T Schweigman and K Barbiers, for technical assistance; S van der Kruijs, for administrative assistance; and M Harzheim and G Krings, for their helpful comments. The Inhance sequence was kindly provided by GE Medical Systems.
References
Footnotes
See Editorial Commentary, p 355
Linked articles 228098.
Funding The MS Center Amsterdam is supported by the Dutch Foundation for MS Research, Voorschoten, The Netherlands (06-538C).
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the VU University Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.