Article Text

Abstract
Objective The optimal consensus concerning treatment of incidental small paraclinoid unruptured intracranial aneurysms (UIAs) remains controversial. The aim of this retrospective study was to reveal the natural history of small paraclinoid UIAs with the goal of informing the treatment plan.
Methods 524 patients harbouring 568 paraclinoid UIAs (≤5 mm) were retrospectively evaluated during the mean follow-up of 35.4 months. The aneurysms were divided into two groups with respect to arterial branch: related (ophthalmic and superior hypophyseal artery), and non-related. Medical records were reviewed concerning multiple variables, such as sex, age, hypertension (HTN), diabetes mellitus, smoking and aneurysmal factors (size, arterial relationship, multiplicity and the occurrence of rupture and growth). The cumulative risk and the risk factors of aneurysmal rupture and growth were analysed.
Results Two aneurysmal (0.35%) ruptures and 17 growths (3.0%) were observed during the follow-up of 1675.5 aneurysm-years with an annual rupture of 0.12% and an annual growth of 1.01%. The cumulative survival without aneurysmal growth reached a significant difference in aneurysms ≥4 mm (p=0.001), HTN (p=0.002), and arterial branch-related location (p=0.001). Multivariate analysis disclosed that aneurysm ≥4 mm (HR, 4.41; p=0.003), HTN (HR, 5.74; p=0.003), arterial branch-related location (HR, 6.04; p=0.002), and multiplicity (HR, 0.27; p=0.042) were significant predictive factors for aneurysm growth.
Conclusions Although incidental small paraclinoid UIAs have a relatively lower rupture and growth risk, patients with high-risk factors, including aneurysm ≥4 mm, HTN, arterial branch-related aneurysms, and multiple aneurysms must be monitored closely. The limitation of the retrospective nature of this study should be taken into consideration.
- Stroke
- Cerebrovascular Disease
- Vascular Surgery
Statistics from Altmetric.com
Introduction
Optimal consensus concerning the treatment of incidental small paraclinoid unruptured intracranial aneurysms (UIAs) remains unclear. Although small UIAs have a lower risk of rupture,1 up to 13% of ruptured cases involve aneurysms that are ≤5 mm in size.2 Such a discrepancy might arise from the heterogeneity of aneurysms in terms of anatomical variations in locations, shape, and formation period.3 ,4
Haemodynamic change and subsequent mechanical stimuli are responsible for aneurysm formation and growth. Differences in aneurysm location, size and extravascular circumstances can be associated with different haemodynamic patterns. Therefore, the management strategy for small paraclinoid aneurysms need to be set differently, not following the general treatment guidelines for small UIAs. However, small paraclinoid aneurysms have been treated by endovascular intervention since embolisation in the clinical field is reasonable,5 regardless of their lower rupture risk.6
Few studies have focused on the natural history of incidental small paraclinoid UIAs. The data have involved aneurysms of the internal carotid artery (ICA).4 Furthermore, no detailed information on the different haemodynamic factor, in particular, the presence of arterial branch relation is available for paraclinoid UIAs ≤5 mm.
This retrospective analysis was undertaken to reveal the natural clinical history of incidentally found small paraclinoid UIAs, with the goal of informing a treatment plan.
Patients and methods
Patient selection and data collection
A retrospective analysis was performed in patients diagnosed as an incidental small paraclinoid UIA (≤5 mm in size) from September 2001 to May 2011 at two affiliated hospitals. This study was approved by the Institutional Review Board at Seoul National University Hospital (H-1208-049-421) and Seoul National University Bundang Hospital (B-1301-186-110). A total of 936 patients harbouring 1004 paraclinoid aneurysms were recruited. After excluding 412 patients with 436 aneurysms who underwent endovascular treatment, 524 patients with 568 aneurysms were enrolled in this cohort. We treated patients with an endovascular approach mainly due to patient preference.
Patients with history of subarachnoid haemorrhage, extradural located aneurysms, fusiform aneurysm, poorly defined broad-necked aneurysm including blood blister shaped, and the UIA related with arteriovenous malformation or intracranial tumour were excluded due to possibility of the different natural history.7
Paraclinoid UIAs were divided into two groups according to arterial branch relation. Aneurysms arising from ophthalmic artery or superior hypophyseal artery were defined as arterial branch-related group. The endpoint of the study was the occurrence of aneurysmal rupture or growth during follow-up. Medical records were reviewed for both non-treated group and treated group concerning multiple variables such as sex, age, hypertension (HTN), diabetes mellitus (DM), smoking and the aneurysmal factors (size, arterial relationship, multiplicity, shape of bleb and the occurrence of rupture and growth) revealed by radiologic tests. Aneurysm rupture was assessed by the information at the last outpatient department visit. For patients lost to follow-up for more than 6 months, a telephone survey was conducted to confirm the neurologic events.
Follow-up radiologic test
Usual follow-up radiologic exams were conducted with three-dimensional (3D) time-of-flight magnetic resonance angiography (MRA) or digital subtraction angiography (DSA) every 6 months or 1 year according to patient clinical conditions in this retrospective study. Catheter angiography was conducted with an Integris Allura biplane system (Philips Medical Systems, Best, The Netherlands). After checking routine angiography, 3D rotational angiography was performed to obtain working projection images. In both radiologic tests, the same directional images were matched for the analysis. Every aneurysm diameter including maximum dimension, depth and neck was calculated using an electronic ruler by two neurosurgeons blinded to patient clinical information. Any discrepancies were re-evaluated by a third reader. Aneurysm growth was defined on the basis of serial images obtained by MRA or DSA: increase of maximum aneurysm size over 1.5 times and morphologic change including a bleb.8 During the follow-up period, endovascular coil embolisation was indicated for an aneurysm diameter exceeding 5 mm, rapid growth exceeding two times, and change in aneurysm appearance.
Statistical analysis
Continuous data are presented as the mean±SD. Fisher exact test and unpaired t test wer used to assess categorical and continuous variables, respectively. Interobserver agreements about aneurysm size were estimated using Kappa statistics. Univariate analysis to evaluate relevant factors of incidental small paraclinoid UIA growth was performed with Cox proportional hazards regression. Risk factors for aneurysm growth were determined using multivariable Cox proportional hazards model including variables p values <0.20. The average annual risk of aneurysm growth (≤5 mm) was calculated by the number of aneurysm enlargements divided by the number of aneurysm years of the follow-up periods. Kaplan–Meier product-limit estimator and generalised Wilcoxon tests were conducted to calculate the cumulative survival without aneurysm growth according to risk factors. p Values <0.05 were regarded as statistically significant. Statistics were performed with SPSS V.19 (SPSS, Chicago, Illinois, USA).
Results
Enrolled and censored cases
A total of 524 patients harbouring 568 small incidental paraclinoid UIAs were examined during the follow-up of 35.4±18.0 months. HTN (n=222, 39.1%), DM (n=63, 11.1%), and smoking (n=60, 10.6%) were noted. The interobserver agreements about aneurysm size obtained by MRA and DSA were excellent (k=0.89 and 0.84, respectively). Four aneurysms related with arterial branch (three ophthalmic arteries and one superior hypophyseal artery) were treated using coil embolisation during the follow-up interval. The reason for intervention was aneurysm diameter increase over 5 mm (n=3) and size increase of 2.2 times (n=1). Treated paraclinoid aneurysms were censored at the time of therapy. Two cases experienced aneurysm rupture, and four cases were lost to follow-up. No aneurysm enlargement or morphological change was noted until the last follow-up in patients with aneurysm rupture or follow-up loss. The estimation of the observation periods was performed from the date of diagnosis to the date of the last follow-up.
Characteristics of incidental small paraclinoid UIAs
Two hundred and fifty-nine (45.6%) arterial branch-related aneurysms, and 309 (54.4%) non-related aneurysms were found. Aneurysms related to arterial branch of ophthalmic and superior hypophyseal artery were noted in 76 and 183 cases, respectively. The most common size of aneurysms ranged from 3.0 mm to 3.9 mm (n=218, 38.4%). One hundred and twelve cases (19.7%) featured aneurysms exceeding 4 mm in diameter. Two hundred and thirty-one (40.7%) were multiple aneurysms. The category of multiple aneurysms was divided based on concomitant aneurysms. Forty-four (7.7%) cases combined with another paraclinoid aneurysms, and 187 (33.0%) with non-paraclinoid concomitant aneurysms were observed.
Comparison between non-treated group and treated group
To evaluate the possibility of selection bias, an inherent limitation of a retrospective study, we compared the predictive factors for rupture and growth between the non-treated group and the treated group. There was no statistically significant difference between the groups in multiple variables, such as sex, age, HTN, DM, smoking and aneurysmal factors (size, arterial relationship, multiplicity, shape of bleb (table 1). Especially, considering the shape of bleb as a surgical indication, there were three aneurysms with blebs in the treated group (0.7%).
Comparison of the baseline characteristics between non-treated group and treated group
Rupture and growth of incidental small paraclinoid UIAs
Two cases (0.35%) of aneurysm rupture (figure 1A–C) and 17 (3.0%) cases of aneurysm growth were observed during the follow-up of 1675.5 aneurysm-years with an overall annual rupture of 0.12% and an overall annual growth of 1.01%. The ruptured paraclinoid UIAs included the following characteristics: female, n=2; age, range 64–71 years; HTN, n=2; multiplicity, n=2; size, range 2.3–4.8 mm; rupture months, range 29–40; aneurysm growth, n=0. Specific growth rates in patients with risk factors were calculated as follows: 2.87% per year in aneurysm ≥4 mm versus 0.59% per year in aneurysm <4 mm; 1.99% per year with HTN versus 0.39% per year without HTN; and 1.85% per year with multiple aneurysms versus 0.41% per year with single aneurysm. Regarding aneurysm location based on relation with arterial branch, 1.8% per year of the arterial branch-related group and 0.42% per year of unrelated group were estimated. The cumulative survival without growth estimated by Kaplan–Meier analysis was as follows: overall, the values were 96.47% (95% CI 94.57% to 98.40%) of all cases; 89.20% (95% CI 81.76% to 97.31%) of aneurysms ≥4 mm versus 98.19% (95% CI 96.74% to 99.65%) of aneurysms <4 mm; 93.19% (95% CI 89.12% to 97.44%) with HTN versus 98.69% (95% CI 97.15% to 100%) without HTN; 92.51% (95% CI 88.43% to 96.78%) of arterial branch-related group versus 99.57% (95% CI 98.75% to 100%) of arterial branch-unrelated group; 98.09% (95% CI 95.87% to 100%) with single aneurysm versus 95.33% (95% CI 92.51% to 98.56%) with multiple aneurysms at 40 months. The cumulative survival without aneurysm growth reached significance for aneurysm ≥4 mm (p=0.001), HTN (p=0.002), arterial branch-related aneurysms (p=0.001). No statistical difference was observed between the multiple aneurysms and single aneurysm (p=0.08).
{kind=link}
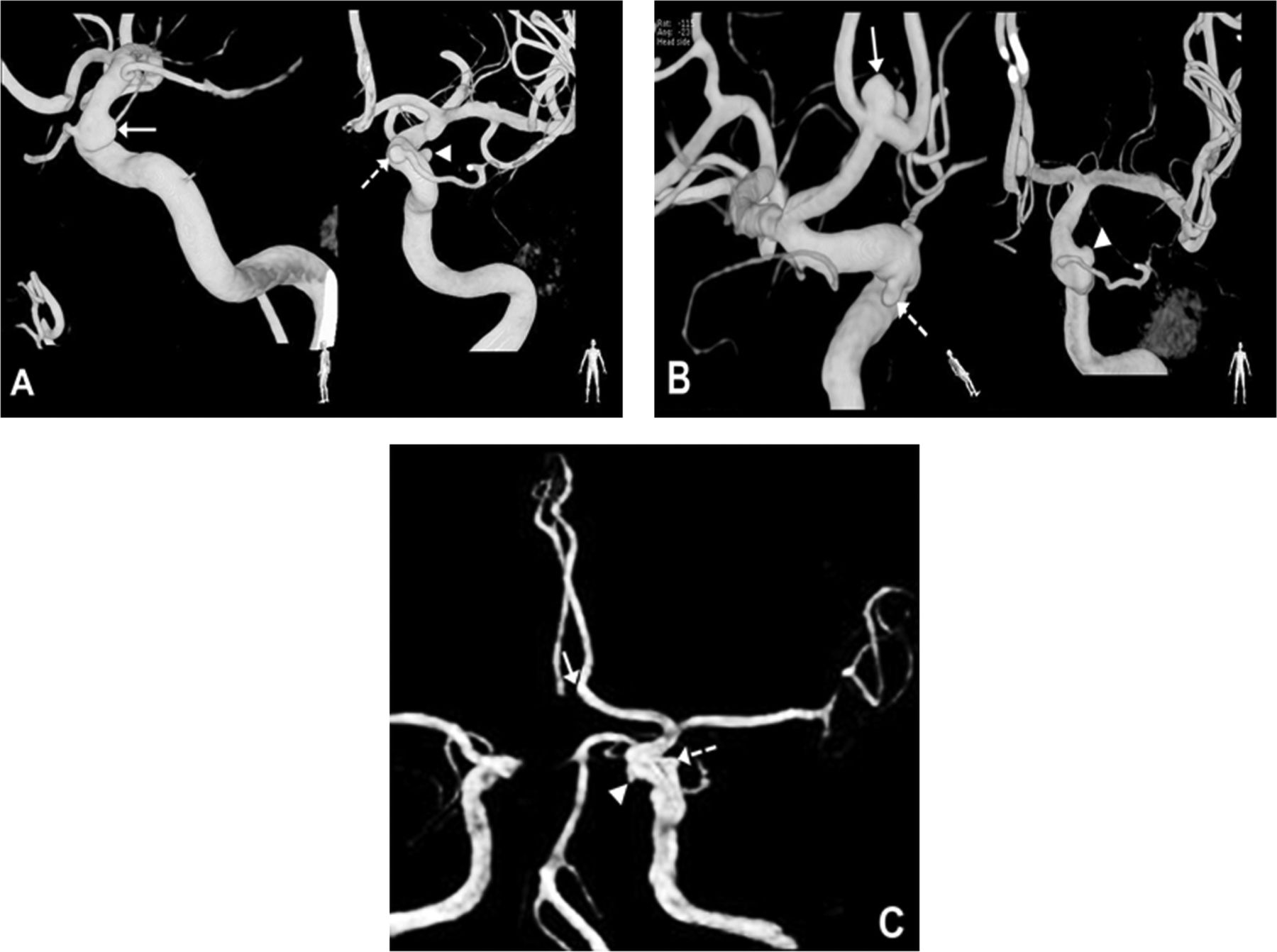
Two patients with aneurysmal rupture during the follow-up of incidental small paraclinoid unruptured intracranial aneurysms (UIAs). The first patient, a 71-year-old woman, harboured three UIAs during the evaluation of progressive bulbar palsy due to amyotrophic lateral sclerosis. Three-dimensional angiography shows right paraclinoid UIA with 3.56 mm×4.82 mm×1.72 mm in its diameter (solid arrow), left paraclinoid UIA at the origin of ophthalmic artery with 2.28 mm×2.10 mm×3.73 mm in diameter (broken arrow), and another left paraclinoid UIA with 2.21 mm×3.89 mm×1.94 mm in its diameter (arrowhead). One of three paraclinoid UIAs was presumed to have rupture during the follow-up (A). The second patient, a 64-year-old woman, also had three UIAs being found during the routine check-up: anterior communicating artery (Acom) UIA with 4.20 mm×6.46 mm×3.55 mm in its diameter (solid arrow); two left paraclinoid UIAs with 2.18 mm×2.96 mm×1.82 mm (broken arrow) and 3.38 mm×3.81 mm×2.68 mm (arrowhead) in their diameters (B). Acom aneurysm was treated by coil embolisation. The 2-year-follow up magnetic resonance angiography (MRA) showed that the coiled Acom aneurysm was well occluded (solid arrow) and two left paraclinoid aneurysms are stationary in size and shape (broken arrow and arrowhead) (C). 1 year after MRA, subarachnoid haemorrhage occurred by rupture of one of the paraclinoid aneurysms.
Risk factors for aneurysmal growth of incidental small paraclinoid UIAs
For aneurysm growth, univariate analysis revealed that aneurysms exceeding 4 mm in diameter (HR, 4.85; 95% CI 1.87 to 12.57; p=0.001), HTN (HR, 5.01; 95% CI 1.63 to 15.38; p=0.005), and arterial branch-related aneurysms (HR, 4.45; 95% CI 1.45 to 13.67; p=0.009) were associated with aneurysm growth. Other variables, such as female gender (p=0.71), age (p=0.25), multiplicity (p=0.06), DM (p=0.44) and smoking (p=0.28) did not differ significantly (table 2). The multivariate analysis disclosed that aneurysm exceeding 4 mm in diameter (HR, 4.41; 95% CI 1.68 to 11.57; p=0.003), HTN (HR, 5.74; 95% CI 1.84 to 17.91; p=0.003), arterial branch-related aneurysms (HR, 6.04; 95% CI 1.93 to 18.92; p=0.002), and multiplicity (HR, 0.27; 95% CI 0.08 to 0.95; p=0.042) were significant predictive factors of aneurysm growth (table 3).
Univariate analysis for predictive factors of incidental small paraclinoid unruptured aneurysm growth
Multivariate analysis for risk factors of aneurysmal growth
Discussion
Treatment indication for intracranial aneurysms includes ruptured and symptomatic unruptured cases. With advances in imaging, incidental small UIAs are being increasingly found. In a recent prospective study, the most common site of the incidental aneurysms was the middle cerebral artery, followed by paraclinoid ICA.9
Optimal treatment consensus over paraclinoid UIAs ≤5 mm in diameter remains debatable. Small paraclinoid UIAs pose a lower rupture risk.4 ,10 Komotar et al11 recommended that conservative management should be performed on incidental aneurysms <5 mm in size regardless of their locations, and that this treatment policy be adapted to small paraclinoid UIAs.12 However, with the advance in endovascular technology, small paraclinoid UIAs have been treated by coil embolisation in the clinical field.
Detailed information on the natural history of incidental small paraclinoid UIAs has been lacking. Previous studies4 ,10 investigated the incidence of rupture of paraclinoid UIAs as a part of ICA aneurysms. The studies involved moderate size of less than 250 small paraclinoid UIAs. A recent study of the natural course of unruptured cerebral aneurysms (UCAS)6 also analysed the rupture rate and its risk factors of ICA aneurysms without focusing on paraclinoid UIAs. Analysis of paraclinoid UIAs growth has not been fully clarified. Presently, this study reveals a relatively lower overall annual rupture of 0.12% and an overall annual growth of 1.01% in incidental small paraclinoid UIAs. Consequently, conservative treatment can become a first choice in the treatment of small paraclinoid UIAs.
The decision-making process for aneurysm treatment should be done considering various haemodynamic patterns and anatomical barriers according to the aneurysm. No clear contribution of haemodynamic stress for aneurysm rupture has been established. High or low12 wall shear stress (WSS) as a main aetiology for aneurysm progression has been suggested, but remains contentious. Minimum WSS and pressure loss coefficient can be responsible for aneurysm rupture. In particular, a larger proportion of the lower WSS within the sac has been suggested as a rupture risk of ICA aneurysm rupture.13 But, the results cannot apply to small incidental aneurysms because cases 5.0–10.0 mm in size were analysed. Tremmel et al14 focused on the size ratio (SR) between the aneurysm and the parent vessel. In the study, higher SR (>2) leads to rupture due to multiple vortices and complex flow patterns. Therefore, the relatively larger diameter of the parent ICA may contribute to a lower rupture risk of the small paraclinoid aneurysm. Tateshima et al15 reported that flow velocity and WSS within the sac were correlated negatively with the dome size of the aneurysm through comparative testing of ruptured and unruptured paraclinoid aneurysms. But, the result may not be compatible in small aneurysms because larger aneurysms (mean size, 11.5 mm; range, 5.8−19.9 mm) were enrolled for analysis. Additionally, sufficient cases for demonstration of haemodynamic parameters of aneurysm at different locations were not included. On the other hand, Chien et al16 suggested that high WSS may be a useful haemodynamic parameter for rupture of small ICA aneurysms (<10 mm). Results of a recent study indicated that a higher energy loss of flow may be related to the progression of aneurysms due to weakening of the wall by the transformed energy.17
Peak intravascular pressure at the arterial bifurcation site is 2–3 times higher than the pressure at the proximal parental artery.18 Thus, there may be a difference in intravascular pressure between arterial branch-related and non-related aneurysms. In our series, aneurysms arising from the arterial branch, such as ophthalmic artery or superior hypophyseal artery, were predictable risk factors of aneurysm growth (HR, 6.04; p=0.002).
During follow-up, aneurysm growth was observed in 17 (3.0%) cases. The result was lower than the 6.7% reported in the Small Unruptured Intracranial Aneurysm Verification (SUAVe) study4 which analysed overall intracranial aneurysms. The SUAVe study revealed that aneurysms >4 mm in size and multiplicity significantly increased aneurysm growth. In our series, aneurysm size exceeding 4 mm, HTN, arterial branch-related location, and multiplicity were related to the growth of incidental small paraclinoid UIAs.
The rupture risk of small aneurysms has been thought to be low. The ISUIA study10 reported a rupture rate of 0.8% per year. In particular, no aneurysm (<7 mm) rupture was noted in the anterior circulation, except in the posterior communicating artery. On the contrary, the SUAVe study4 disclosed one case of ICA aneurysm rupture (0.6%). But, the authors did not provide detailed description of the aneurysm location. The UCAS study6 also reported a lower rupture rate of ICA aneurysm, but detailed analyses according to the ICA location and size were not performed. In our cohort, two paraclinoid aneurysms experienced rupture, and the rupture rate was estimated as 0.35% per year. Interestingly, no aneurysm growth was observed during the follow-up interval of either 29 months or 40 months. In general, larger aneurysms and recently developed aneurysms have a higher chance of rupture.3 Therefore, more data concerning the aneurysm rupture, especially small size and the formation period, are needed to determine the risk factors for rupture of small paraclinoid UIAs.
There are three treatment modalities for incidental small paraclinoid UIAs: conservative, surgical, or interventional. Aneurysm obliteration by surgical clipping can be a more confirmative method than the endovascular approach,19 but the technique remains challenging due to anatomical difficulties. In particular, successful operation can require additional procedures, including proximal ICA control and bypass surgery.20 The surgery-related permanent morbidity rate of up to 6% has been reported.19 Endovascular intervention has shown good results for small UIA, but procedure-related rupture and thromboembolic complications are still a concern. Small aneurysms are more likely to experience rupture than larger aneurysms and still remain a technical challenge.21 Moreover, small aneurysms are usually packed with fewer coils, and may lead to recanalisation of the aneurysm.22 Recanalisation rates exceeding 2% have been reported in small UIAs after embolisation.21 ,23 Ihara et al24 proposed a treatment strategy according to anatomical locations, where direct surgery should be considered for superior projecting aneurysm and endovascular for other aneurysm locations. However, the change in principle concerning the management indication of paraclinoid UIA dimension from 3 mm to 5 mm did not involve without supporting data. In our cohort, incidental small paraclinoid aneurysms were initially treated conservatively. During the follow-up, 17 cases of paraclinoid aneurysm experienced enlargement. Among them, coil embolisation was performed for four cases due to an increase in size over 5 mm (n=3) and 2.2 times larger than the initial size (n=1).
Our study has several distinctive features. First, we focused on the natural history of the small paraclinoid UIAs. Moreover, detailed information was provided about the risk factors of aneurysm growth. Second, our cohort had a larger sample size of 568 paraclonid UIAs. Third, patients with conservative treatment were monitored strictly throughout the study. As a result, more accurate assessment of risk factors of aneurysm growth could be achieved. Fourth, more distributed populations across the country have been enrolled in this cohort (data not shown). Accordingly, regional bias can be avoided.
The major limitation of this study is its inherent nature of the retrospective study. Concerns remain the possibility of selection bias between treatment groups by the retrospective nature of our study. Comparing 568 non-treated and 436 treated incidental small paraclinoid UIAs in this study, there was no significant difference in all the variables analysed for the predictive factors of rupture and growth. A bleb change, which can lead to a definite selection bias, was only evident in three patients in the treated group, which may exclude a morphological difference between the treated and non-treated groups. This result may lessen the strength of the selection bias. Nevertheless, patients who underwent endovascular therapy for the presence of bleb could lead to underestimation of the true rupture and growth rate. Accordingly, the result might not apply to small paraclinoid UIAs with irregular shape.
Conclusions
Although incidental small paraclinoid UIAs have a relatively lower rupture and growth risk, patients with high risk factors, including aneurysm ≥4 mm, HTN, arterial branch-related aneurysms and multiple aneurysms must be monitored closely. The limitation of retrospective nature in this study should also be taken into consideration.
Acknowledgments
We would like to thank So-Hee Oh, Sung-Eun Kim and Ji-won Jeoung for their help with the data collection, and their valuable contribution to the statistical analysis.
References
Footnotes
-
Contributors J-EK devised the original study design. J-SJ, J-HA and W-H performed data collection and statistical analyses. Y-JS, C-HS, J-SB, H-SK and O-KK interpreted the results. J-SJ wrote the manuscript. J-EK and C-WO made revision.
-
Funding This study was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A102065), and by a grant of Seoul National University Hospital (0320120310, 2012–0581).
-
Competing interests None.
-
Ethics approval This study was approved by the Institutional Review Board at two participating centres. Institutional Review Board at Seoul National University Hospital (H1208049421) and Seoul National University Bundang Hospital (B1301186110).
-
Provenance and peer review Not commissioned; externally peer reviewed.