Article Text

Abstract
Objective To investigate the MRI manifestation pattern of asymptomatic natalizumab-associated progressive multifocal leukoencephalopathy (PML) in patients with multiple sclerosis (MS).
Methods 18 patients with MS with natalizumab-associated PML lesions on MRI were included. In 6 patients, the PML lesions were identified on MRI prospectively and in 12 patients PML lesions were identified retrospectively. MRI sequences were analysed for PML lesion distribution, appearance, grey matter/white matter involvement and possible signs of inflammation. Lesion probability maps were created to demonstrate lesion distribution pattern.
Results The frontal lobe was involved in 14 patients (77.8%) and the parietal lobe in 4 patients (22.2%). Most patients presented with focal lesions (13 patients, 72.2%) involving one single lobe (12 patients, 66.7%). The cortical grey matter was affected in 15 patients (83.3%) and 13 patients (72.2%) presented with a combination of cortical grey and white matter involvement. Signs of inflammation were detected in 7 patients (38.8%). Among patients with available diffusion-weighted imaging, 6 patients (40%) did not show high-signal-intensity lesions. A classical imaging pattern including unilateral and unilobar focal lesions in the frontal lobe affecting the cortical grey matter or the cortical grey and adjacent white matter was observed in 8 patients (44.4%).
Conclusions Asymptomatic natalizumab-associated PML manifestations on MRI show a rather localised disease, frequently located in the frontal lobes, affecting the cortical grey matter and adjacent juxtacortical white matter. Awareness of this lesion pattern facilitates an earlier diagnosis of natalizumab-associated PML in an asymptomatic stage associated with a more favourable prognosis.
- INFECTIOUS DISEASES
- MRI
- MULTIPLE SCLEROSIS
- NEURORADIOLOGY
Statistics from Altmetric.com
Introduction
Natalizumab is a monoclonal antibody against α4-integrin, approved for the treatment of relapsing multiple sclerosis (MS) with beneficial effects on clinical and MRI outcomes.1 ,2 A serious side effect of natalizumab treatment is the occurrence of progressive multifocal leukoencephalopathy (PML), an opportunistic infection of the central nervous system (CNS) due to reactivation and replication of the John Cunningham virus (JCV).3 ,4
As of 4 February 2014, a total of 437 cases of natalizumab-associated PML have been documented in more than 100 000 MS patients treated with natalizumab.5 The diagnosis of PML is based on the clinical presentation, the identification of JCV DNA in the CNS (e.g., in the cerebrospinal fluid) and imaging findings, preferably on MRI.6 ,7 Compared with other PML populations, the imaging findings in natalizumab-associated PML have been described as heterogeneous and fluctuating.8–11 However, MRI has high sensitivity in the detection of PML lesions and is able to detect PML pathology months before first symptoms occur, with lesions demonstrated prospectively or retrospectively on MRI obtained several months before clinical symptoms of PML became apparent.12–19
It has been shown that the detection of natalizumab-associated PML in an asymptomatic stage is associated with a better survival and functional outcome compared with those patients being symptomatic at the time of diagnosis.18 Therefore, it is crucial to increase the number of patients diagnosed in an asymptomatic stage by using MRI in drug surveillance programmes. Recent case series have summarised the imaging findings in patients with symptomatic natalizumab-associated PML trying to identify involvement patterns.8 ,9 However, the imaging findings in asymptomatic patients are rather subtle and difficult to interpret and have never been systematically analysed so far.
The aim of this study is to investigate the MRI findings of natalizumab-associated PML in an asymptomatic stage and try to identify MRI patterns, which could aid in establishing an asymptomatic PML diagnosis probably leading to a more favourable patient outcome.
Methods
Standard protocol approvals, registrations and patient consents
The study was approved by the local institutional review board and written informed consent for the use of the clinical and imaging data in research and education was obtained from all participants.
Patient selection
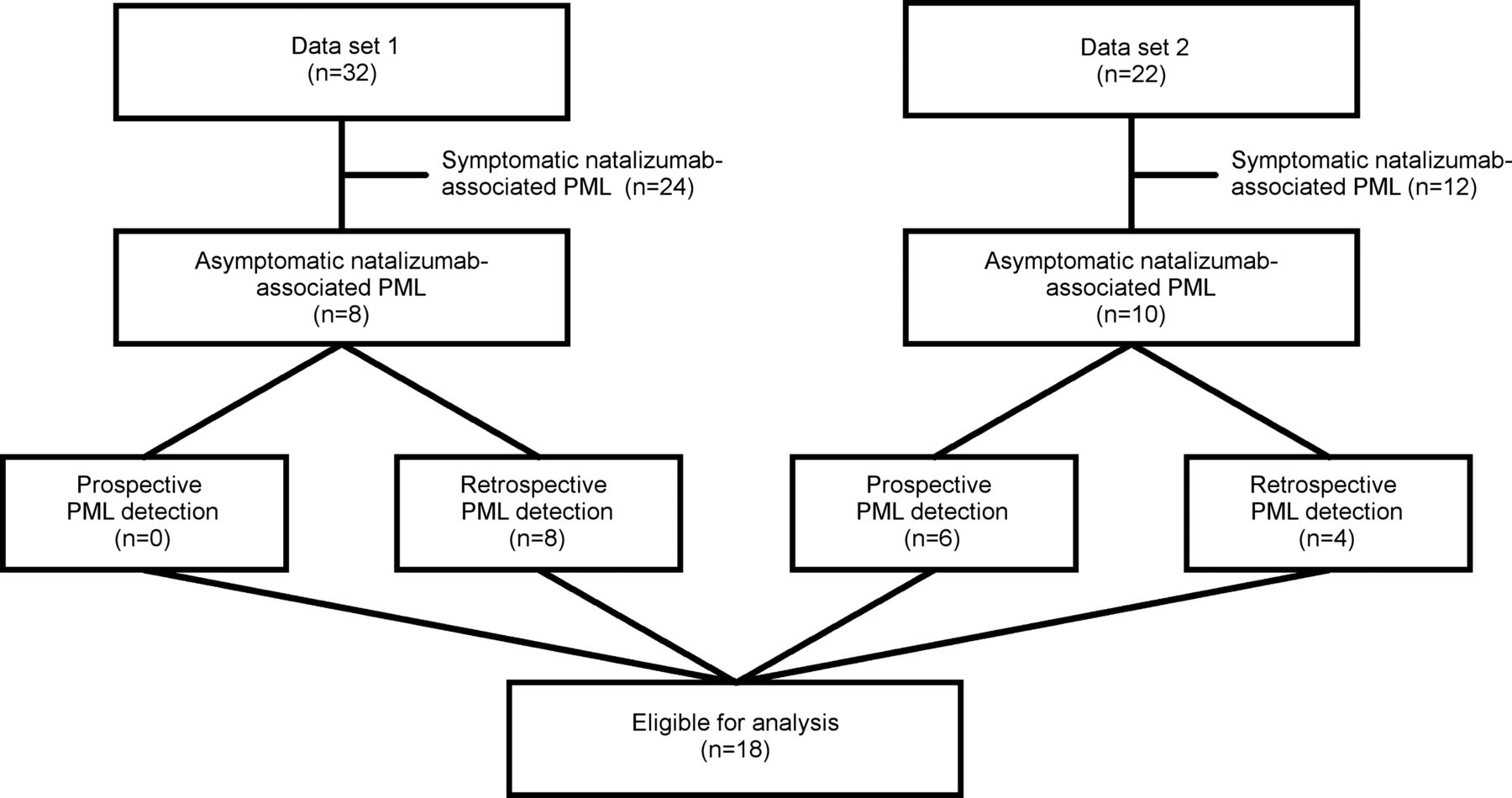
Patients were selected from two different data sets. The first data set (Data set 1, figure 1) included 32 natalizumab-treated patients who had been diagnosed with PML between 2004 and 2008 in a postmarketing setting and identified by the US Food and Drug Administration safety information and the adverse event reporting programme MedWatch (http://www.fda.gov./ForConsumers/ConsumersUpdates/ucm107970.htm). The imaging material as well as the demographic and clinical information was provided by Biogen Idec. This data set has been used previously to describe the basic imaging pattern and the functional outcome of patients with acute natalizumab-associated PML.8 ,9 ,18 The second data set (Data set 2, figure 1) included data prospectively collected from the Dutch natalizumab-associated PML cohort consisting of 22 patients. Three patients with prospective asymptomatic PML have been described previously in a case series focusing on the challenge in diagnosing asymptomatic natalizumab-associated PML according to the American Academy of Neurology (AAN) diagnostic criteria.20 In all cases, the PML diagnosis including the interpretation of the imaging studies and cerebrospinal fluid (CSF) analysis was made by a referring local neurologist who was responsible for the treatment and monitoring of each patient; all patients have been classified according to the AAN PML diagnostic criteria.6

Flow chart demonstrating patient enrolment (PML, progressive multifocal leukoencephalopathy).
Inclusion criteria were applied according to a recent published expert panel on MRI in natalizumab-associated PML9: showing no symptoms suggestive of PML while PML lesion(s) were visible on MRI and the availability of Digital Imaging and Communication in Medicine (DICOM) imaging data with sufficient image quality of the MRIs. The definition of asymptomatic natalizumab-associated PML was:
Prospective detection of asymptomatic PML lesions: PML lesions prospectively detected on MRI compared with a previous MRI during natalizumab surveillance for PML screening while the patient does not show any clinical symptoms suggestive of PML.
Retrospective detection of asymptomatic PML lesions: patients with symptomatic natalizumab-associated PML showing lesions suggestive of PML on (historical) MRIs obtained before clinical symptoms suggestive of PML were apparent.
MRI protocol
All patients underwent a multisequence MRI protocol with diverging sequences, magnetic field strengths, acquisition parameters and parameters related to spatial resolution. Fluid-attenuated inversion recovery (FLAIR) and T2-weighted MR images were available in all patients. Diffusion-weighted images (DWI) and contrast-enhanced T1-weighted images were available in 15 patients (83.3%). In a given patient, similar MRI protocols were available before and/or after the onset of the PML lesion.
Image analysis
All images were analysed by an experienced neuroradiologist with special expertise in the field of inflammatory diseases of the CNS. All MRIs were presented in a digital fashion on workstations. The scorings scheme of the PML lesions included the location (frontal lobe, parietal lobe, occipital lobe, temporal lobe, basal ganglia and infratentorial), involvement of the tissue types (white matter only, grey matter only, mixed grey matter/white matter and deep grey matter), distribution (unilobar, multilobar, widespread, unilateral and bilateral), lesion characteristics (focal: one or two focal lesions, multifocal: three or more focal lesions, confluent: lesions with a confluent appearance and diffuse: lesions with characteristics of diffuse abnormal white matter) and signs of inflammation (contrast enhancement, small lesions in the vicinity of the main lesion as described earlier).9 The lesion distribution categories were defined as follows: unilobar (confined to one lobe), multilobar (involving two or more contiguous lobes) and widespread (involving two or more non-contiguous lobes and/or present in both hemispheres).
The rating of the PML lesions was based on T2-weighted and FLAIR images. The signs of inflammation were scored on T2-weighted (small lesions in the vicinity of the main lesion) and contrast-enhanced T1-weighted images. In addition, DWI was separately evaluated for high-signal-intensity lesions suggestive of PML.
Lesion probability map
A lesion probability map (LPM) was constructed to obtain a visual representation of the distribution of the asymptomatic PML lesions as follows. First, for each patient, a PML lesion mask was determined manually using MIPAV software (http://mipav.cit.nih.gov/) using the T2-weighted or FLAIR image. Then, the Brain Extraction Tool (BET) was used to extract the brain tissue (part of FMRIB Software Library (FSL) 5.0.4, http://www.fmrib.ox.ac.uk/fsl).21 Subsequently, the brain extracted image of each patient was linearly registered to MNI152 standard space using FLIRT (also part of FSL) with the correlation ratio as the cost function.22 The resulting transformations and nearest neighbour interpolation were used to transform the lesion masks to standard space. An LPM was obtained by accumulating all registered lesion masks.
Results
Patient's characteristics
A total number of 18 asymptomatic patients with PML lesion(s) on MRI met the inclusion criteria and were included in this study. In 6 patients, the asymptomatic PML diagnosis was established prospectively and in 12 patients MRI lesions suggestive of PML were detected retrospectively before clinical symptoms suggestive of PML occurred. Five patients in the prospective asymptomatic PML group fulfilled the AAN diagnostic criteria of probable PML (positive MRI findings and detection of JCV in the CSF). One asymptomatic patient in this prospective group with MRI lesions highly suspicious of PML, had no detectable JCV DNA in the CSF and did not formally fulfil the AAN diagnostic criteria of probable or possible PML (not PML). However, the clinical and imaging follow-up demonstrated a classical PML immune reconstitution inflammatory syndrome (PML-IRIS) manifestation (based on clinical and imaging findings as recently described3 ,10 ,11) confirming the diagnosis of possible PML (symptomatic and imaging findings suggestive of PML) at a later disease stage. The clinical manifestations and MRI findings of this particular patient and two other patients with prospective asymptomatic PML have been described in detail previously.20 Ten patients of the retrospective PML cases fulfilled the AAN diagnostic criteria of definite PML and two patients fulfilled the criteria of possible PML (no JCV DNA detected in the CSF) at the time of PML diagnosis at the later symptomatic stage. All patients in whom, retrospectively, MRI lesions suggestive of PML were detected before clinical symptoms occurred, presented with clinical symptoms at the time the PML diagnosis was established. The detailed patient's characteristics are presented in table 1.
Patient's characteristics
Imaging findings
Detailed imaging findings are presented in table 2. The frontal lobe was involved in the majority of the patients (14 patients, 77.8%) followed by the parietal lobe (4 patients, 22.2%). Most patients presented with a more localised disease involving one single lobe (12 patients, 66.7%) whereas five patients (27.8%) showed a widespread involvement and one patient a multilobar (5.6%) lesion distribution. Among the five patients with a widespread lesion distribution, two presented with a bilateral frontal lobe and one patient with a bilateral posterior fossa involvement. The remaining 2 patients showed bilateral lesion manifestations involving the frontal and parietal lobes. The majority of patients (13, 72.2%) presented with focal lesions and 5 patients (27.8%) with confluent lesions. The cortical grey matter was affected in 15 patients (83.3%) and the white matter in 15 patients (83.3%). The majority of patients (13, 72.2%) presented with a combination of cortical grey and white matter involvement. Signs of inflammation (either small punctuate lesions in the vicinity of the main lesions or contrast-enhancing lesions) were seen in a considerable number of patients (7 patients, 38.9%). Taken together, the most frequent imaging pattern was a unilobar focal lesion distribution in the frontal lobe affecting the cortical grey matter or the cortical grey and adjacent white matter, as observed in 8 patients (44.4%; figure 2). In those patients with small focal lesions on MRI, these lesions were located in the cortical grey matter or in the cortical grey matter–white matter junction (figure 2). Among the 15 patients with DWI sequences available at the time of PML lesion manifestation on MRI, 6 patients (40%) did not show high-signal intensity in the area of the PML lesion(s) visible on T2-weighted and/or FLAIR sequences.
Detailed overview of imaging findings

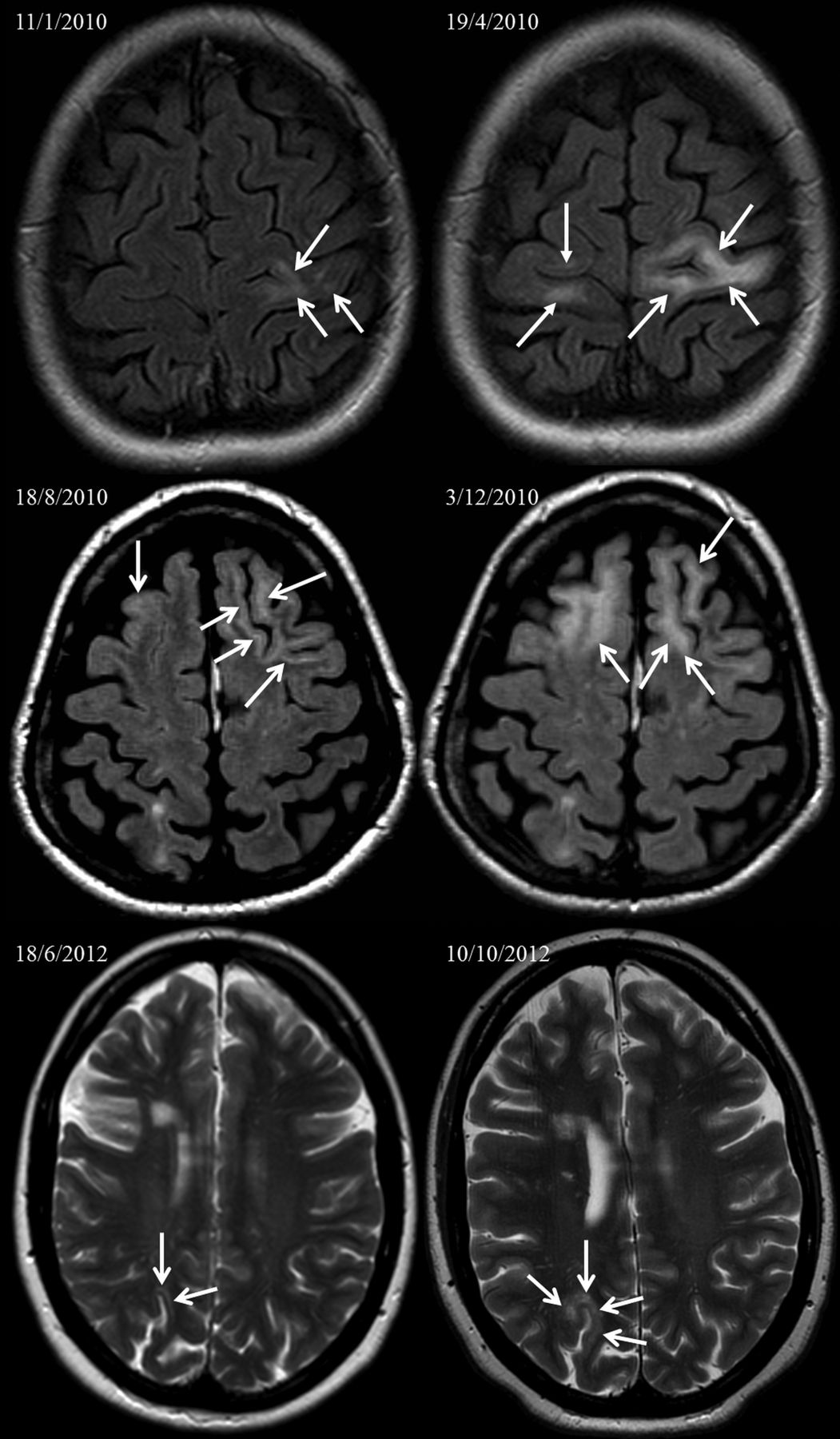
Examples of MRI findings in asymptomatic patients with natalizumab-associated progressive multifocal leukoencephalopathy (PML; left column) and the lesion evolution during follow-up after the patients have become symptomatic (right column). Top row: axial fluid-attenuated inversion recovery (FLAIR) images showing lesions in the left frontal lobe affecting the subcortical white matter, juxtacortical white matter and the adjacent cortical grey matter. At the asymptomatic stage the lesion distribution was classified as unilobar (left). MRI performed at the symptomatic stage (right) showed lesion progression particularly in the deep white matter and the occurrence of new lesions in the contralateral hemisphere (closed head arrows). At that stage the PML lesion dissemination was classified as widespread. Middle row: axial FLAIR images showing PML lesion predominantly affecting the juxtacortical white matter and adjacent cortical grey matter of both frontal lobes (arrows). Even at the asymptomatic stage, the PML lesion dissemination had to be classified as widespread. After becoming symptomatic, the patient showed lesion progression in both frontal lobes also affecting substantial parts of deep white matter (right). Bottom row: axial T2-weighted MRI of an asymptomatic patient with PML developing a small PML lesion in the juxtacortical white matter and the adjacent cortical grey matter (arrows), indistinguishable from a focal multiple sclerosis lesion. After developing symptoms, the lesion showed progression with cortical grey matter spreading and pronounced involvement of the adjacent white matter.
Lesion probability map
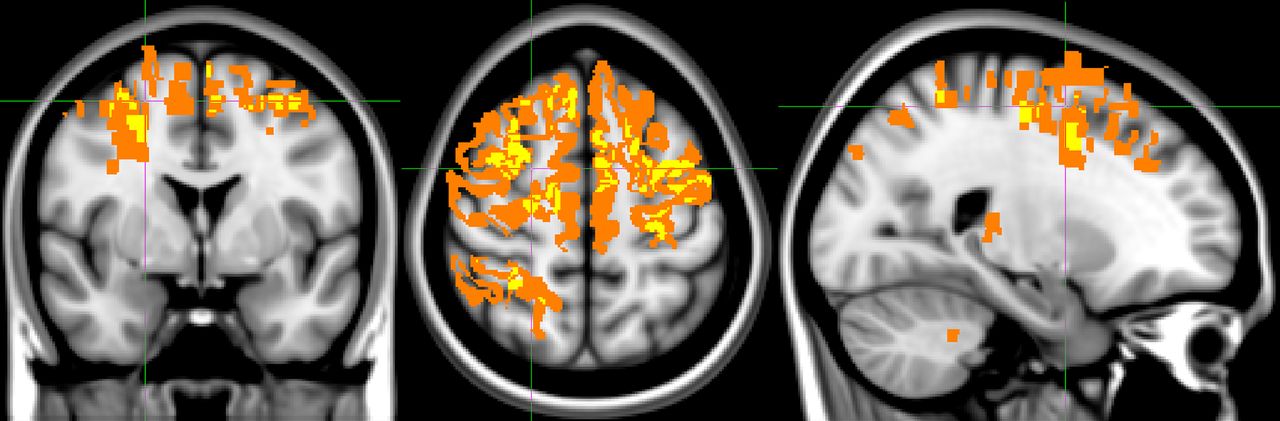
The LPM showed clustering of PML lesions in the frontal lobe and to a minor degree in the parietal lobe. Most of the lesions were located in the peripheral areas of the subcortical white matter, and extended to the juxtacortical white matter and the adjacent cortical grey matter (figure 3). More central or infratentorial white matter structures were less frequently involved.
{kind=link}
{kind=link}
{kind=link}
Lesion probability map in the axial (middle), coronal (left) and sagittal (right) orientation displaying the spatial distribution of natalizumab-associated asymptomatic progressive multifocal leukoencephalopathy lesions in MNI space (x=67, y=126, z=128). An orange colour indicates a lesion occurence in a single patient in a specific voxel whereas yellow indicates the presence of a lesion in at least 2 patients. Lesions occur in a rather localised pattern, particularly involving the juxtacortical white matter and cortical grey matter of the frontal and to a lesser extent of the parietal lobe.
Discussion
Compared with the available imaging data obtained from patients with symptomatic natalizumab-associated PML, this is the first study describing the imaging pattern in patients being asymptomatic when MRI lesions suggestive of PML were detected. The clinical relevance of identifying PML lesions on MRI in asymptomatic patients has been stressed by recent data suggesting a more favourable outcome in terms of survival and functional outcome measures such as Expanded Disability Status Scale (EDSS) and Karnofsky performance scale (KPS).18 ,23 ,24 Our data suggests an imaging pattern that includes a frequent PML lesion manifestation in the frontal lobe, involving subcortical and juxtacortical white matter structures but also quite frequently the adjacent cortical grey matter. Occasionally, particularly in patients presenting with very small lesions, a PML onset exclusively located in the cortical grey matter can be observed. The involvement of cortical grey matter in natalizumab-associated PML has been highlighted by previous case studies.10 ,25 ,26 In a case series including 22 patients with natalizumab-associated PML, cortical involvement has been identified in 50% of the patients.9 However, the topic of grey matter involvement in PML has been neglected for a long time. Fortunately, several histopathological studies have conclusively demonstrated that cortical pathology in terms of neuronal infection and cortical demyelination are important features in PML or JCV infection in general.27–32 This is also reflected by subtypes of JCV infection such as granule cell neuropathy and JCV associated encephalopathy.29 ,32 ,33 In other words, PML is not a white matter disease as the term “leukoencephalopathy” might suggest.
Compared with symptomatic PML, in which the lesion dissemination tends to involve multiple lobes affecting both hemispheres, patients with asymptomatic PML present more frequently with a rather localised disease with unilobar and focal lesion, which can be confirmed by our data set.18 However, interestingly, some asymptomatic patients might present with widespread disease. Looking in more detail, some of these patients classified as widespread PML do have a rather localised disease involving one lobe in both hemispheres. In our data set, two of the five patients with widespread PML had single lobe (frontal lobe) involvement of both hemispheres and one patient had involvement of both cerebellar hemispheres.
Compared with other PML populations, contrast-enhancement can be observed quite frequently in natalizumab-associated PML, occurring in about 30% of the cases at the time of diagnosis and can be the leading imaging sign in asymptomatic patients.8 ,12 ,34 The significance of this enhancement in terms of whether it reflects an inflammatory PML subtype or already a first stage of PML-IRIS is still a matter of debate.10 ,34 A second sign of possible inflammation consisting of small punctiform lesions in the vicinity of the main PML lesion associated with contrast-enhancement and possible PML-IRIS manifestation has been introduced.9 Signs of inflammation, either contrast-enhancement or small punctiform lesions, were observed in 38.9% of the patients, stressing the fact that inflammation can already be observed at the earliest stage of PML.
It has been suggested that DWI is a suitable method in the detection of acute demyelination in PML leading to swelling of oligodendrocytes and astrocytes, which is reflected by high-DWI signal intensity.35 In acute natalizumab-associated PML stages, almost all PML lesions show a high-signal intensity, which has led to the assumption that DWI might be a good screening sequence in the context of MRI surveillance for the detection of PML lesions in asymptomatic patients.8 ,9 However, DWI can be negative in patients with asymptomatic natalizumab-associated PML. In our patients with available DWI sequences, 40% did not show high-signal-intensity DWI lesions in the area of the PML lesions on the T2-weighted and/or FLAIR images. This can be explained by the smaller size of PML lesions in these asymptomatic patients or the lesion location (at least to a fractional extent) in the cortical grey matter with an intrinsic high cellularity. In addition, in very early (asymptomatic) PML stages, the degree of oligodendrocytic and astrocytic damage is presumably milder compared with the tissue damage in symptomatic patients.
The above discussed imaging features of patients with asymptomatic natalizumab-associated PML have considerable consequences for current and future concepts of natalizumab surveillance even months after the natalizumab treatment has been discontinued.36 ,37 It is important to realise that we are dealing with a more localised disease on MRI, which can be indistinguishable from MS disease activity. Small focal PML lesions can share major imaging features with MS lesions, particularly small lesions in the juxtacortical white matter and/or cortical grey matter. Although (cortical and juxtacortical) PML lesions show some differences compared with MS lesions in terms of histopathology,31 these differences can hardly be assessed at an asymptomatic stage on standard MR sequences. In addition, DWI can be of limited value in these lesions. Given the fact that JCV DNA detection in CSF can also be negative in these cases, the diagnosis of PML at an asymptomatic stage can be even more difficult to establish. Therefore, dedicated guidelines, algorithms and diagnostic tests such as the CSF-JCV antibody index are required in order to manage this diagnostic challenging situation.38
A limitation of our study is the rather small sample size of patients with asymptomatic PML and the study design of analysing data obtained from a prospective and retrospective data collection. However, since asymptomatic lesions are visible in the minority of natalizumab-associated PML cases, we think that this approach is justifiable to create a sufficient data set without influencing or biasing the conclusion of the results. Another limitation might be not having performed a comparison between asymptomatic and symptomatic PML lesions. However, symptomatic lesions are usually larger, involving several lobes. Therefore, we think that the approach of identifying a lesion pattern including a LPM in patients with symptomatic PML has limited relevance and has already been published.9
In conclusion, the MRI manifestation pattern of asymptomatic natalizumab-associated PML follows an imaging pattern frequently showing a rather localised lesion distribution involving the juxtacortical white matter and cortical grey matter structures of the frontal and parietal lobe. This knowledge of the lesion manifestation in these patients is of special clinical relevance since it likely aids in the diagnosis of natalizumab-associated PML at an asymptomatic stage leading to a higher survival rate and improved functional outcome.
Acknowledgments
The authors wish to thank the patients with PML for agreeing to the use of their MRIs and (para)clinical data for research and educational purposes.
References
Footnotes
Contributors All authors were involved in the drafting/revising of the manuscript; study concept or design; and the analysis or interpretation of the data. MPW and NDR were involved in the acquisition of the data. MPW and MDS contributed in the statistical analysis. MPW, MDS and AV conducted the study supervision or coordination.
Competing interests MPW serves as a consultant for Biogen-Idec. He serves on the editorial board of European Radiology. JK has accepted consulting fees from Merck-Serono, Teva, Biogen and Novartis. VU Medical Center has received financial support for research activities from Bayer Schering Pharma, Biogen-Idec, GlaxoSmithKline, Merck Serono, Novartis and Teva. DAS reports personal fees from Novartis and Genzyme. STFMF reports grants, personal fees and other from Biogen Idec and Novartis; personal fees and other from Genzyme; grants and other from Teva Aventis; and other from Roche and Merck Serono. NDR is a senior neurology fellow in clinical development at Biogen Idec. FB serves on the editorial boards of Brain, European Radiology, Neuroradiology, Multiple Sclerosis and Radiology and serves as a consultant for Bayer-Schering Pharma, Sanofi-Aventis, Biogen Idec, Teva, Novartis, Roche, Synthon BV, Genzyme and Jansen Research.
Ethics approval Institutional Review Board VUMC, Amsterdam, The Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.